Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 13(4); 2022 > Article
-
Original Article
Menstrual hygiene management and its determinants among adolescent girls in low-income urban areas of Delhi, India: a community-based study -
Suneela Garg1
 , Nidhi Bhatnagar1, Mongjam Meghachandra Singh1, Saurav Basu1,2, Amod Borle1, Yamini Marimuthu1, Falak Azmi1, Yomri Dabi1, Indu Bala1
, Nidhi Bhatnagar1, Mongjam Meghachandra Singh1, Saurav Basu1,2, Amod Borle1, Yamini Marimuthu1, Falak Azmi1, Yomri Dabi1, Indu Bala1 -
Osong Public Health and Research Perspectives 2022;13(4):273-281.
DOI: https://doi.org/10.24171/j.phrp.2022.0127
Published online: August 31, 2022
1Department of Community Medicine, Maulana Azad Medical College, New Delhi, India
2Indian Institute of Public Health–Delhi, Public Health Foundation of India, Gurugram, India
- Corresponding author: Saurav Basu Indian Institute of Public Health–Delhi, Public Health Foundation of India, Sector 44, Plot 47, Gurugram, Haryana 122002, India E-mail: saurav.basu1983@gmail.com
© 2022 Korea Disease Control and Prevention Agency.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Abstract
-
Objectives
- Menstrual hygiene management (MHM) in developing countries is linked to human rights, social justice, and the education and empowerment of young girls. The objective of this study was to assess menstrual hygiene practices and their determinants among adolescent girls, including school dropouts, and the effects of pad distribution programs in urban resettlement areas of Delhi, India.
-
Methods
- A cross-sectional study was conducted from March 2019 to February 2020 in urban resettlement colonies and 2 villages of Delhi among 1,130 adolescent girls aged 10 to 19 years, who were interviewed face to face.
-
Results
- In total, 954 participants (84.4%) used only disposable sanitary pads, 150 (13.3%) used both sanitary pads and cloths, and 26 (2.3%) used only cloths (n=1,130). Most school-going girls utilized the scheme for pad distribution, but only two-thirds of the girls who were out of school utilized the scheme. In the adjusted analysis, girls with lower educational status, those who had dropped out of school, and those from the Muslim religious community were more likely to use cloths for MHM.
-
Conclusion
- More than 4 out of 5 adolescent girls in Delhi in low-income neighborhoods preferred sanitary pads for MHM. The government free pad scheme reached near-universal utilization among school-going girls (97%), but the subsidized pad scheme for girls who did not attend school was insufficiently utilized (75%).
- Menstruation is a recurrent biological phenomenon beginning during adolescence and occurring in women throughout their reproductive lifespan [1]. Adolescence, the age from 10 to 19 years, represents the transition from childhood to adulthood, and among girls it is also a time for learning to manage their menstrual health needs safely and effectively [2].
- Healthy menstrual hygiene management (MHM) includes the usage of safe materials to adsorb or collect menstrual blood that can be changed as frequently as required and in privacy, cleaning private parts with soap and water, and enabling access to facilities for the safe disposal of the materials used for menstrual management [3,4]. However, millions of adolescent girls in developing countries of Asia and Africa are unable to meet their MHM needs due to diverse factors including taboos and stigma related to menstruation, a lack of access to water, hygiene and sanitation (WASH) facilities, and the lack of accessibility, affordability, and confidence in using modern and safe menstrual management materials [5,6]. The inability to achieve menstrual hygiene and protection may cause adolescent girls to identify the process of menstruation with embarrassment, stigma, and an undignified recurrent experience until menopause, as well as rendering them vulnerable to reproductive tract infections [7,8]. A study in urban slums of Lucknow in North India reported that young women experienced shame and embarrassment from the non-normalization and a lack of support for menstruation in their schools [9]. Menstrual hygiene is therefore a significant public health issue that is also linked to human rights, social justice, and the education of girls, which are necessary for achieving gender equality [10].
- According to the National Family Health Survey-5 (2019–2020), a nationally representative, multistage random, cross-sectional survey in India, 50.2% (95% confidence interval [CI], 49.8%–50.5%) adolescent girls aged 15 to 19 years reported utilizing cloths to meet menstrual needs [11]. Furthermore, young women in India, especially those from a low socioeconomic background, often lack correct awareness of MHM particularly in relation to the appropriate duration and frequency of changing pads and their safe disposal [12].
- Consequently, to improve MHM among adolescent girls in India, the government of India, in 2011, launched the Menstrual Hygiene Scheme (MHS) under the aegis of the National Rural Health Mission, which is a landmark initiative of the government of India for improving the health determinants of Indians living in rural areas. The MHS promulgated 3 key objectives for menstrual hygiene promotion: increasing awareness, ensuring access to “high quality napkins,” and ensuring their safe disposal in an environmentally friendly manner [13]. The MHS was planned to provide menstrual hygiene support including delivery of pads at highly subsidized prices to over 15 million adolescent girls (10–19 years) in 152 districts across 20 states of India [14]. Nevertheless, the MHM since its inception has been challenged by an irregular supply chain and inconsistent pad quality [15].
- In 2019, the government of the state of Delhi proposed a revamped MHS that was named “UDAAN” (flight) for out-of-school adolescent girls. In addition, the state initiated another MHS for girls attending government schools that was funded by the Directorate of Education [16]. Adolescent girls living in low-income areas such as resettlement colonies and urban slums constitute the most important target population for urban MHM schemes. There is a paucity of information on pad utilization and pad quality supplied through government schemes and factors influencing their acceptability, which is also unavailable from existing secondary data sources such as the National Family Health Surveys (NFHS).
- The present study was therefore conducted with the objective of assessing menstrual hygiene practices and their determinants among adolescent girls, including school dropouts, and the effect of pad distribution programs in urban resettlement areas of Delhi.
Introduction
- Study Design and Setting
- We conducted a community-based cross-sectional study from March 2019 to February 2020 in 4 urban resettlement colonies of Delhi, which are low-income areas and populated by residents relocated from urban slums including a large proportion of North Indian migrants employed in both informal and formal small-scale industries, retail shops, and construction sites.
- The study was approved by the Institutional Ethics Committee, Maulana Azad Medical College & Associated Hospitals (F.1/IEC/MAMC/(65/05/2018/no378). Written and informed assent with parental consent from minors and written and informed consent from adult participants were obtained.
- Study Population
- We enrolled adolescent girls (10–19 years) living in the selected areas for at least 6 months. Five girls were excluded as they were incapable of responding to the questions due to mental or physical handicaps.
- Study Outcomes
- The study outcomes were the proportions of adolescent girls using sanitary pads (napkins) and cloths, as well as the frequency of change of sanitary pads during menstruation.
- Sample Size Calculation and Sampling Method
- The sample size for this cross-sectional study at 95% CIs, 20% relative precision, expecting a 12.7% frequency of satisfactorily changing menstrual absorbent materials, and considering a design effect of 1.5 was calculated to be 1,022 using OpenEpi ver. 3 (Open Source Epidemiological Statistics for Public Health, Georgia, GA, USA), the target sample size was further increased to 1,130 to increase power [17].
- A multistage sampling technique was applied to select the study areas. Four out of the 11 districts in the state were initially selected using simple random sampling (SRS). Subsequently, from each of these districts, 1 urban resettlement colony was subsequently selected, again using SRS. The selected urban resettlement colonies and the number of participants in each were estimated based on the population proportion to sample size (PPS) method. These included Gokalpuri in the North East District (n=234), Sarai Kale Khan in the South District (n=288), Mangolpuri in the North West District (n=398) and Kalyanpuri in the East District (n=180).
- The adolescents in the resettlement colonies were selected using the systematic random sampling method after the following steps. (1) A list of the total number of blocks in each urban resettlement colony was obtained. (2) The number of participants recruited from each block was calculated as the desired sample size from the district (and also the urban resettlement colony) divided by the total number of blocks within that urban resettlement colony. (3) The sampling interval was calculated as the total number of houses in each block divided by the number of participants required to be enrolled from each block. (4) Within households with more than 1 eligible participant, participant selection was conducted using the Kish selection grid [18].
- In addition, a total of 30 participants were also selected from a rural area of Delhi according to the PPS method since only 2.5% of Delhi’s population is considered rural. The participants were selected from 2 villages that were selected through convenience sampling; households with adolescent girls were located with the help of frontline health workers functioning in that area.
- Methodology
- An orientation meeting was conducted at every site among the investigators, local schoolteachers, frontline health workers, and the medical officer in charge of the Delhi government dispensary or urban primary health centers of the area to plan for enhancing community engagement. In total, 30 accredited social health activists (ASHAs), 30 schoolteachers, and 6 medical officers participated in these meetings. These meetings discussed the significance of MHM particularly in context of underserved communities, government schemes available, and experiences and feedback of locals regarding these schemes and their future expectations. The processes of community sensitization for enhancing community responsiveness and participation in the survey were also delineated.
- Survey Procedure
- A team of 2 trained field investigators and a research associate, all of female gender, conducted the community survey with assistance from frontline health workers in the area.
- Operational Definitions
- 1. Proper disposal of menstrual absorbent material was defined as wrapping the pad and disposing of it in a dustbin.
- 2. Improper disposal included throwing it in the open or in a dustbin without wrapping, flushing in the toilet, digging and disposing of it in the earth, and washing the absorbent before disposal.
- 3. The socioeconomic status of the participants was based on their per-capita income updated according to the consumer price index for industrial workers for 2019 [19,20].
- Description of the UDAAN and the school MHS for adolescent girls
- To implement the scheme, Indian frontline health workers known as the ASHAs were provided training on menstrual hygiene issues in adolescents by master trainers using predesigned modules. The ASHAs were responsible for distributing sanitary pads to the eligible beneficiaries. A pack of 6 sanitary pads labeled as “Freedays” were sold to adolescent girls that were out of school at a price of INR 6 per pack. The sale and purchase of the pads were planned at designated government primary health facilities known as anganwadis once every week, preferably on Wednesdays. The ASHA was required to maintain a record of the demographic details of all beneficiaries to be reported monthly to the district administration. ASHAs received an incentive of INR 2 per pack sold along with a free pack for their personal use each month. For school-going adolescents studying in any government school in Delhi, a pack of 6 pads was provided free of cost each month from the sixth standard (i.e., grade or year in school) onwards. The pads were distributed within classrooms by schoolteachers [16].
- Statistical Analysis
- Data were analyzed using IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA). Summary statistics were reported for the outcome variables. The independent variables associated with the use of sanitary pads during menstruation in the bivariate analysis (p=0.20) were included in a binomial logistic regression model, and the associations were expressed as adjusted odds ratios (ORs) with 95% CIs. A p-value less than 0.05 was considered statistically significant.
Materials and Methods
- Sociodemographic Characteristics
- In total, 1,130 adolescent girls were enrolled in the study. The response rate of the survey was 100%. There were 474 participants (41.9%) aged below <16 years, while 656 girls (58.1%) were aged 16 to 19 years. A majority (86%) of the participants lived in nuclear families, while 14% lived in intergenerational families. Only 20 participants (1.8%) were married, and 32 (2.8%) were employed (Table 1).
- A total of 768 (68.0%) of the participants were school-going, while 240 (21.2%) were school dropouts, 105 (9.3%) had completed school, and 17 (1.5%) were illiterate. The SES of the participants measured by the per-capita income of the families and assessed using the BG Prasad scale was class I (highest) in 56 (5.0%), class II in 159 (14.1%), class III 234 (20.7%), class IV 372 (32.9%), and class V (lowest) in 306 (27.1%) (n=1,127, missing=3).
- Menstruation-Related Characteristics
- At the time of menarche, 735 participants (65.2%) were 11 to 13 years old, 351 (31.1%) were 14 to 16 years old, 35 (3.1%) were 8 to 10 years old, and 9 (0.8%) achieved delayed puberty (i.e., after the age of 16 years).
- There were 827 participants (73.2%) who usually had menstrual periods that lasted for 3 to 5 days and 303 (26.8%) whose periods lasted for ≥6 days. A total of 1,006 participants (89.0%) reported having regular and 124 (11.0%) irregular menstrual cycles in the previous 3 months. The interval between menstrual cycles was 26 to 35 days in 987 participants (87.3%), ≤25 days in 74 (6.5%), and ≥36 days in 18 (1.6%), and 52 participants (4.6%) reported usually having irregular intervals.
- Knowledge of Menstruation and Menstrual Hygiene
- Trusted sources of menstruation-related information for the participants were their mothers (53.7%), teachers (25.5%), friends and relatives (25.5%), sisters (17.0%), mass media (2.7%), and frontline community health workers (0.7%). Table 2 reports the awareness of menstruation and menstrual hygiene among the participants. Preparedness for menarche was absent in a majority (51.2%) of the participants. A total of 675 participants (59.8%) reported usually consulting a person outside the formal health system for menstruation-related problems, of whom 572 (84.7%), 54 (8.0%), 40 (5.9%) and 9 participants (1.3%) consulted their mothers, sisters, relatives, and friends, respectively. The frequency of changing absorbent material each day during menstruation was correctly reported to be 3 to 4 times by 834 participants (73.8%). Younger participant age (<15 years) was associated with a lack of awareness of the optimal frequency of changing menstrual absorbent material (p=0.003), but educational status was not (p=0.274) (Table 2).
- Menstrual Hygiene Management
- Among the study participants, 954 participants (84.4%) used only disposable sanitary pads, 150 (13.3%) used both sanitary pads and cloths, and 26 (2.3%) used only cloths (n=1,130). Among the participants who used cloths or both cloths and pads (n=176), 171 (97.1%) discarded cloths after using them, whereas 4 (0.3%) reused cloths after washing them with soap and water and drying them in the sunlight. In the bivariate analysis, education limited to middle school, not going to school, lack of awareness, lack of good hygiene, and the Muslim religion were associated with the absence of exclusive use of pads as an adsorbent material (Table 1). However, in the adjusted analysis, the participants with education beyond the eighth standard had 1.5 times higher odds of using only pads during menstruation (OR, 1.7; 95% CI, 1.1–2.2), those belonging to the Hindu religion had 1.9 times higher odds of using only pads (OR, 1.9; 95% CI, 1.2–2.9), and those currently going to school had 2.4 times higher odds of using only pads (OR, 2.4; 95% CI, 1.7–3.6) (Table 3).
- The frequency of changing pads or cloths during a typical menstrual cycle was reported as ≤6 pads per cycle by 183 (16.2%), 7 to 10 pads per cycle by 426 (37.7%), 11 to 15 pads per cycle by 183 (16.2%), and ≥15 pads (29.9%) per cycle. The frequency of changing adsorbent material per day during menstruation was reported as 1 to 2 times by 273 (24.2%) and ≥3 times by 857 participants (75.8%). A suboptimal frequency of adsorbent change per day (1–2 times) was significantly associated with limited education (up to middle school; p=0.001) but not with the family’s per-capita income (p=0.083).
- The usual domestic site for change of adsorbent material among the participants was within their homes in 1,105 participants (97.8%) and in community toilets by 25 participants (2.2%). Among the school/college/working participants (n=792), 420 participants (53.0%) changed their soaked material in toilets, while 372 adolescent girls (47.0%) reported never changing their soaked adsorbent material at school or workplaces. Most girls had access to an individual toilet at home (90.2%), or an improved community toilet (9.2%), along with a continuous running water source within those toilets (83.0%). Furthermore, 1,051 (93.3%) reported correctly disposing the used adsorbent material, while 81 (7.2%) performed improper disposal.
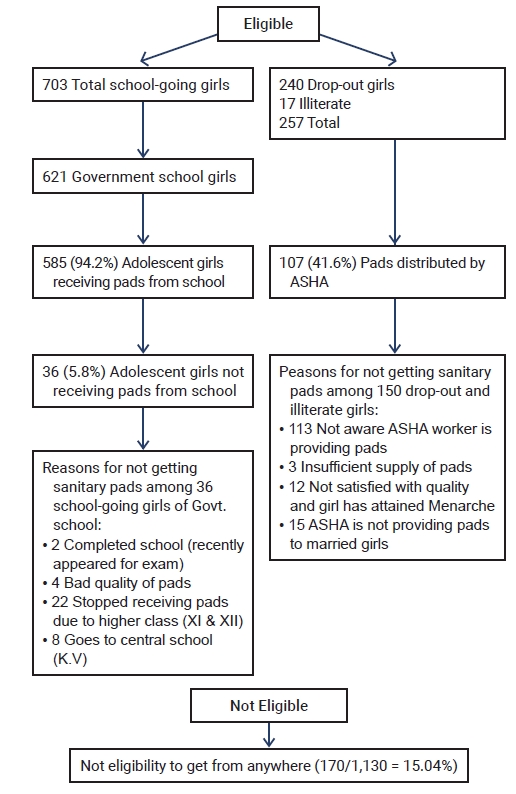
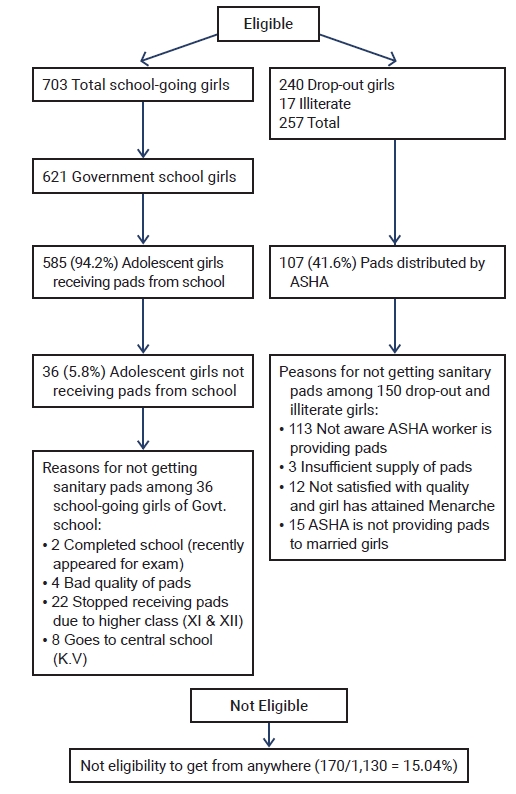
- Access to Sanitary Pads
- The extent of utilization of the UDAAN MHS by the participants is depicted in Figure 1. In total, 936 participants (82.8%) in this study were eligible to receive sanitary pads through the UDAAN scheme. Among the school-going adolescents studying in government schools of Delhi, 97% received pads without cost as per the provisions of the scheme. However, among those girls who had dropped out of school (n=238) and eligible to receive pads through purchase at highly subsidized rates from their local ASHAs, only 155 (65.1%) utilized the scheme. Some girls attributed their reason for not buying pads through the scheme to their “poor quality compared to those available in the market.” Moreover, the ASHAs reported that among the girls from lower socioeconomic classes, there were challenges in affordability of the pads even at the very low rates, which undermined the feasibility of sustained pad use. Girls who had completed school (9.3%) or were studying in open schools (4.2%), private schools (2.6%), and colleges (6.1%) were not eligible to receive pads through the UDAAN.
- Difficulty in purchasing sanitary pads was reported by 313 participants (27.7%), of whom 195 (62.3%) attributed it to financial constraints, 149 (47.6%) felt ashamed when buying pads, and 4 (1.2%) were unaware of their availability.
Results
- Healthy MHM ensures equity in the health, educational, and social domains of a society. The present community-based study conducted among adolescent girls living in the urban resettlement colonies of Delhi ascertained a high prevalence of exclusive use of pads as absorbent material for MHM (84.4%), which was significantly higher than the national average reported in previous studies (55%) and the 5th round of the NFHS (64%) [12,13]. However, nearly 1 in 4 girls reported a suboptimal frequency of absorbent change due to their use beyond the recommended period, predisposing them to a risk of reproductive tract infections.
- In this study, menstruation preparedness was present in nearly half (48.8%) of the participants, a significantly higher proportion than reported in previous studies conducted in both urban and rural settings in India [21−24]. However, like in previous studies, the main resource for MHM was reported to be the girls’ mothers in this study [23,24]. Furthermore, very few girls obtained information on MHM from their schoolteachers or frontline health workers, which reflects a missed opportunity to educate them about the best MHM practices and dispel their ignorance on menstrual health issues. Another observation is that a majority of the girls changed their menstrual absorbent material at schools, signifying an advancement in the sensitization, availability of privacy, and WASH facilities in government schools, compared to earlier studies from India [25].
- The present study shows that despite a high level of acceptance and preference for sanitary pads and the rapid replacement of cloths as an absorbent material, the affordability of pads is a continued challenge for adolescent girls belonging to low-SES families. Consequently, these girls are dependent upon the government’s free and subsidized pad distribution schemes, whose financial viability and sustainability are necessary. Moreover, for girls that have dropped out of school, economic vulnerability is likely to be higher and the affordability of pads, even at subsidized rates, is a difficult proposition.
- A significant proportion of girls in this study reported feeling ashamed in buying pads, indicating the high prevalence of stigma associated with menstrual pads, a false perception that contributed to lowering of their self-efficacy in achieving healthy MHM. These problems need to be addressed through community sensitization and effective information, education, and communication (IEC) campaigns.
- From the perspective of the UDAAN MHM scheme, there are 2 key policy implications. First, the program must incorporate an effective IEC and Behavior Change Communication (BCC) component to promote awareness of healthy MHM among the beneficiaries, which is currently lacking, particularly related to appropriate duration of absorbent material use and correct frequency of pad and the risks associated with non-compliance. Moreover, an increasing educational level among the girls did not translate into an improved knowledge of changing absorbent materials in a way that would meet menstrual hygiene requirements, signifying gaps in the incorporation of MHM in the educational curriculum.
- For girls that prefer to use both cloths and pads, instructions for their proper washing and drying in sunlight merit attention. Second, nearly 1 in 5 adolescent girls living in urban resettlement colonies are not eligible to receive pads through these schemes, and this factor was significantly associated with the absence of pad use. Furthermore, girls from low SES may not avail themselves of discounted pad schemes because they expect to receive the products for free and have problems with pad affordability. Achieving universal pad use among adolescent girls in India therefore needs stronger government commitment to the provision of pads to economically vulnerable groups, while also maintaining good pad quality to meet client expectations and improve affordability. The economic sustainability and feasibility of the increasing financial allocations required for continuing and expanding coverage under such schemes also necessitate a health impact assessment and economic evaluation.
- The strengths of this study are that it was conducted among adolescent girls living in urban resettlement colonies, who often constitute a socioeconomically vulnerable population and are prioritized for government welfare schemes.
- The limitations of this study are the cross-sectional study design, due to which the incidence of reproductive tract infections and health outcomes associated with suboptimal MHM could not be assessed. Moreover, any variation in MHM of the girls or changes in the availability and quality of pads through the UDAAN and school MHS could not be prospectively assessed in this study. Finally, urban-rural variations in MHM were not compared in this study since the Delhi population is mostly urbanized.
- In conclusion, more than 4 in 5 adolescent girls in Delhi in low-income neighborhoods preferred sanitary pads for MHM, although their knowledge of the appropriate frequency of pad changes was suboptimal. The government free pad scheme reached near-universal utilization among school-going girls (97%), but the subsidized pad scheme for girls who did not attend school was insufficiently utilized (75%).
Discussion
-
Ethics Approval
The study was approved by the Institutional Ethics Committee, Maulana Azad Medical College & Associated Hospitals (F.1/IEC/MAMC/(65/05/2018/no378). Written and informed assent with parental consent from minors and written and informed consent from adult participants were obtained.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
This project received financial support from the Delhi State Health Mission under grant number F4-19/6/2019-Adolescent Health/2375. The funding agency had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
-
Availability of Data
The datasets are not publicly available, but are available from the corresponding author upon reasonable request.
-
Authors’ Contributions
Conceptualization: SG, NB, MMS, SB; Data curation: FA, YD, IB; Formal analysis: NB, YM, SB; Funding acquisition: SG, MMS; Investigation: SG, NB, MMS; Methodology: all authors; Project administration: SG, MMS, NS, YM; Resources: SG; Supervision: SG, NB, AB; Validation: SG, NB, MMS; Writing–original draft: SB; Writing–review & editing: all authors.
Article information
| Variable | Total (n=1,130) | Using clothsa) | Using pads | p-value |
|---|---|---|---|---|
| Educational status | ||||
| Up to the eighth standard | 281 (24.9) | 67 (23.8) | 214 (76.2) | <0.001 |
| Ninth standard and above | 849 (75.1) | 109 (12.8) | 740 (87.2) | |
| Religion | ||||
| Hindu | 952 (84.2) | 129 (13.6) | 823 (86.4) | <0.001 |
| Muslim | 167 (14.8) | 47 (28.1) | 120 (71.9) | |
| Going to school/college | ||||
| Currently going to school | 768 (68.0) | 87 (11.3) | 681 (88.7) | <0.001 |
| Completed school | 105 (9.3) | 15 (14.3) | 90 (85.7) | |
| Dropped out | 257 (22.7) | 74 (28.8) | 183 (71.2) | |
| Awareness of menstruation before menarche | ||||
| Present | 552 (48.8) | 72 (13.0) | 480 (87.0) | 0.022 |
| Absent | 578 (51.2) | 104 (18.0) | 474 (82.0) | |
| Awareness about schemes related to menstruation | ||||
| Present | 157 (13.9) | 15 (9.6) | 142 (90.4) | 0.025 |
| Absent | 973 (86.1) | 161 (16.5) | 812 (83.5) | |
| Bathing during menstruation | ||||
| Yes | 1,012 (89.6) | 145 (14.3) | 867 (85.7) | <0.001 |
| No | 118 (10.4) | 31 (26.3) | 87 (73.7) | |
| Cleaning one’s private parts during menstruation | ||||
| Yes | 1,089 (96.4) | 163 (15.0) | 926 (85.0) | 0.0037 |
| No | 41 (3.6) | 13 (31.7) | 28 (68.3) | |
| Per-capita income (in Indian rupees) | ||||
| ≥1,051 | 824 (72.9) | 119 (14.4) | 705 (85.6) | 0.106 |
| ≤1,050 | 306 (27.1) | 57 (18.6) | 249 (81.4) |
| Awareness | Correct response | |
|---|---|---|
| Awareness of menstruation before menarche | 552 (48.8) | |
| Menstruation is a physiological process | 554 (49.0) | |
| Normal duration of menstruation | 835 (73.9) | |
| Women stop menstruation as they grow older | 817 (72.3) | |
| Menstrual blood does not contain impurities | 203 (18.0) | |
| Pain during menstruation is normal | 848 (75.0) | |
| Frequency of changing adsorbent material | 834 (73.8) | |
| Consultation of a healthcare provider is necessary for menstruation-related problemsa) | 174 (15.4) |
- 1. Matsumoto S, Nogami Y, Okhkuri S. Statistical studies on menstruation; a criticism on the definition of normal menstruation. Gunma J Med Sci 1962;11:294−318.
- 2. Hennegan J, Shannon AK, Rubli J, et al. Women's and girls' experiences of menstruation in low- and middle-income countries: a systematic review and qualitative metasynthesis. PLoS Med 2019;16:e1002803.ArticlePubMedPMC
- 3. WHO/UNICEF Joint Monitoring Programme. Meeting report of the JMP Post-2015 global monitoring working group on hygiene. Washington, DC: WHO/UNICEF; 2012.
- 4. Sommer M, Sahin M. Overcoming the taboo: advancing the global agenda for menstrual hygiene management for schoolgirls. Am J Public Health 2013;103:1556−9.ArticlePubMedPMC
- 5. Phillips-Howard PA, Caruso B, Torondel B, et al. Menstrual hygiene management among adolescent schoolgirls in low- and middle-income countries: research priorities. Glob Health Action 2016;9:33032. ArticlePubMedPMC
- 6. Hussein J, Gobena T, Gashaw T. The practice of menstrual hygiene management and associated factors among secondary school girls in eastern Ethiopia: The need for water, sanitation, and hygiene support. Womens Health (Lond) 2022;18:17455057221087871. ArticlePubMedPMCPDF
- 7. Das P, Baker KK, Dutta A, et al. Menstrual hygiene practices, WASH access and the risk of urogenital infection in women from Odisha, India. PLoS One 2015;10:e0130777.ArticlePubMedPMC
- 8. Anand E, Singh J, Unisa S. Menstrual hygiene practices and its association with reproductive tract infections and abnormal vaginal discharge among women in India. Sex Reprod Healthc 2015;6:249−54.ArticlePubMed
- 9. McCammon E, Bansal S, Hebert LE, et al. Exploring young women's menstruation-related challenges in Uttar Pradesh, India, using the socio-ecological framework. Sex Reprod Health Matters 2020;28:1749342. ArticlePubMedPMC
- 10. Sommer M, Hirsch JS, Nathanson C, et al. Comfortably, safely, and without shame: defining menstrual hygiene management as a public health issue. Am J Public Health 2015;105:1302−11.ArticlePubMedPMC
- 11. International Institute for Population Sciences (IIPS). National Family Health Survey (NFHS-5), 2019−21: India report [Internet]. Mumbai: IIPS; 2022 [cited 2022 Aug 20]. Available from: https://dhsprogram.com/pubs/pdf/FR375/FR375.pdf.
- 12. van Eijk AM, Sivakami M, Thakkar MB, et al. Menstrual hygiene management among adolescent girls in India: a systematic review and meta-analysis. BMJ Open 2016;6:e010290.ArticlePubMedPMC
- 13. National Health Mission. Scheme for promotion of menstrual hygiene among adolescent girls in rural india [Internet]. National Health Mission; 2016 [cited 2021 Jul 11]. Available from: https://nhm.gov.in/WriteReadData/l892s/61090433691481276612.pdf.
- 14. National Rural Health Mission. Operational guidelines: promotion of menstrual hygiene among adolescent girls (10-19 years) in rural areas [Internet]. New Delhi: National Rural Health Mission. [cited 2021 Jul 11]. Available from: http://www.nrhmhp.gov.in/sites/default/files/files/MHP-operational-guidelines.pdf.
- 15. Bhattacharya S, Singh A. How effective is the menstrual hygiene scheme? An evaluation study from North India. Int J Community Med Public Health 2016;3:2584−6.Article
- 16. Government of National Capital Territory of Delhi. Directorate General of Health Services. Annual report (2020-21) [Internet]. Delhi: Government of National Capital Territory of Delhi [cited 2022 May 1]. Available from: http://health.delhigovt.nic.in/wps/wcm/connect/5d0a188045e977739e3cfe6876edb3cf/AR20211.pdf?MOD=AJPERES&lmod=-501219937&CACHEID=5d0a188045e977739e3cfe6876edb3cf.
- 17. Goel P, Kumar R, Meena GS, et al. Association of sociodemographic characteristics with KAP regarding menstrual hygiene among women in an urban area in Delhi. Trop J Obstet Gynaecol 2018;35:158−64.Article
- 18. Gaziano C. Comparative analysis of within-household respondent selection techniques. Public Opin Q 2005;69:124−57.Article
- 19. Sharma R. Revision of Prasad's social classification and provision of an online tool for real-time updating. South Asian J Cancer 2013;2:157. ArticlePubMedPMC
- 20. Sharma R. Real-time update for the Prasad's Social Classification (or the BG Prasad scale) [Internet]. [cited 2021 Jul 11]. Available from: www.prasadscaleupdate.weebly.com.
- 21. Kamath R, Ghosh D, Lena A, et al. A study on knowledge and practices regarding menstrual hygiene among rural and urban adolescent girls in Udupi Taluk, Manipal, India. Global J Med Public Health 2013;2:1−9.
- 22. Mahajan A, Kaushal K. A descriptive study to assess the knowledge and practice regarding menstrual hygiene among adolescent girls of Government School of Shimla, Himachal Pradesh. CHRISMED J Health Res 2017;4:99−103.Article
- 23. Chandra-Mouli V, Patel SV. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low- and middle-income countries. Reprod Health 2017;14:30. ArticlePubMedPMCPDF
- 24. Coast E, Lattof SR, Strong J. Puberty and menstruation knowledge among young adolescents in low- and middle-income countries: a scoping review. Int J Public Health 2019;64:293−304.ArticlePubMedPMCPDF
- 25. Sharma S, Mehra D, Brusselaers N, et al. Menstrual hygiene preparedness among schools in India: a systematic review and meta-analysis of system-and policy-level actions. Int J Environ Res Public Health 2020;17:647. ArticlePubMedPMC
References
Figure & Data
References
Citations
- Menstrual Hygiene Problems and Challenges Faced by Adolescent Females in Rural Areas: A Narrative Review
Vijiya Kashyap, Sonali G Choudhari
Cureus.2023;[Epub] CrossRef - Perceived difficulties in maintaining menstrual hygiene practices among indigenous adolescents during seasonal water scarcity periods in Bandarban hill district of Bangladesh: A cross-sectional study
Imdadul Haque Talukdar, M.A. Rifat, Plabon Sarkar, Nobonita Saha, Mesfin Kassaye Tessma, Md. Ibrahim Miah
International Journal of Hygiene and Environmental.2023; 254: 114268. CrossRef - Menstrual hygiene practices among adolescent women in rural India: a cross-sectional study
Aditya Singh, Mahashweta Chakrabarty, Shivani Singh, Rakesh Chandra, Sourav Chowdhury, Anshika Singh
BMC Public Health.2022;[Epub] CrossRef
 Cite
Cite