Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 12(5); 2021 > Article
-
Review Article
Severe acute respiratory syndrome coronavirus 2 and respiratory syncytial virus coinfection in children -
Milad Zandi1,2
 , Saber Soltani1,2, Mona Fani3, Samaneh Abbasi4, Saeedeh Ebrahimi5, Ali Ramezani6,7
, Saber Soltani1,2, Mona Fani3, Samaneh Abbasi4, Saeedeh Ebrahimi5, Ali Ramezani6,7 -
Osong Public Health and Research Perspectives 2021;12(5):286-292.
DOI: https://doi.org/10.24171/j.phrp.2021.0140
Published online: October 1, 2021
1Department of Virology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
2Research Center for Clinical Virology, Tehran University of Medical Sciences, Tehran, Iran
3Department of Pathobiology and Laboratory Sciences, School of Medicine, North Khorasan University of Medical Sciences, Bojnurd, Iran
4Department of Microbiology, School of Medicine, Abadan University of Medical Sciences, Abadan, Iran
5Department of Medical Microbiology, Faculty of Medicine, Kerman University of Medical Sciences, Kerman, Iran
6Department of Virology, School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
7Infectious Diseases Research Center, Birjand University of Medical Sciences, Birjand, Iran
- Corresponding author: Samaneh Abbasi, Department of Microbiology, School of Medicine, Abadan University of Medical Sciences, Ayatollah Taleghani Blvd, Abadan, Iran E-mail: s_abbasi80@yahoo.com
© 2021 Korea Disease Control and Prevention Agency
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
- Abstract
- Introduction
- Severe Acute Respiratory Syndrome Coronavirus-2
- Respiratory Syncytial Virus
- Incidence of COVID-19 and RSV Infection in Children
- Causes of Viral Coinfection
- Symptoms of COVID-19 and RSV in Children
- SARS-CoV-2 and RSV Diagnosis in Children
- SARS-CoV-2 and RSV Treatment in Children
- Conclusion
- Article information
- References
Abstract
- Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which has infected many people around the world. Children are considered an important target group for SARS-CoV-2, as well as other viral infections such as respiratory syncytial virus infection. Both SARS-CoV-2 and respiratory syncytial virus can affect the respiratory tract. Coinfection of SARS-CoV-2 and respiratory syncytial virus can pose significant challenges in terms of diagnosis and treatment in children. This review compares the symptoms, diagnostic methods, and treatment of COVID-19 and respiratory syncytial virus infection in children.
- Coronavirus disease 2019 (COVID-19), which causes viral pneumonia, has recently challenged the global healthcare system. COVID-19 is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which belongs to the Coronaviridae family [1]. As it spread rapidly to more than 100 countries all over the world, the World Health Organization declared COVID-19 as a pandemic on March 11, 2020 [2]. Meanwhile, acute lower respiratory tract infections are the cause of death for about 160,000 neonates and more than 760,000 infants annually [3]. Studies have shown that Streptococcus pneumoniae and Haemophilus influenzae type b are common causes of bacterial pneumonia in children [4,5]. Furthermore, postmortem studies of SARS-CoV-2-positive patients have also reported coinfections of SARS-CoV-2 with respiratory viruses such as respiratory syncytial virus (RSV), influenza virus, human bocavirus, parainfluenza virus, and human metapneumovirus [6].
- It has been estimated that 22% of episodes of acute lower respiratory infections in children younger than 5 years are associated with RSV [7]. RSV can affect the bronchioles of the lungs. Coinfection of RSV with SARS-CoV-2 can be a key factor in the development, diagnosis, and treatment of COVID-19 in children.
Introduction
- SARS-CoV-2 affects both the upper and lower respiratory tracts, as well as involving other organs such as the liver, heart, kidney, and brain [8]. Acute lung injury is observed in COVID-19 patients, as well as uncontrolled production of various cytokines and changes in the balance of immune cells, which eventually lead to acute respiratory distress syndrome (ARDS) [9]. Both sexes and all ages are affected by COVID-19, and older individuals and people with underlying diseases are classified as high-risk groups [10]. SARS-CoV-2 can also infect children and infants; although COVID-19 tends to be milder in children than in adults, children can carry and transmit SARS-CoV-2 [11]. Coinfection of SARS-CoV-2 with other respiratory agents can complicate the diagnosis, treatment, and prognosis of COVID-19, as well as increasing patients’ susceptibility (morbidity, symptom severity, and mortality) to COVID-19 [12]. Netea et al. [13] reported that COVID-19 is mild in most cases, although coinfections with other respiratory agents can increase the susceptibility of patients to severe disease.
Severe Acute Respiratory Syndrome Coronavirus-2
- RSV was first identified in chimpanzees in 1955; after a short time, it was confirmed that RSV could be pathogenic in humans. Human RSV is a single-stranded, negative-sense RNA virus that belongs to the genus Pneumovirus in the Pneumoviridae family [14,15]. RSV, which is recognized as one of the most common respiratory viruses that infect children worldwide [16], usually causes bronchiolitis in young children; however, it sometimes can develop into pneumonia. Studies have shown that RSV can infect 90% of children in the first 2 years of life [17]. It has been estimated that RSV annually causes 33 million lower respiratory tract infections, as well as 199,000 deaths in children under 5 years of age in the world [18]. Studies have reported that underlying lung or heart diseases may increase the severity of RSV infection. Premature infants, young children, adults, and older adults with weakened immune systems are at especially high risk for severe illness resulting from RSV [19]. Exposure to smoke is an important environmental risk factor for infant respiratory infections, such as RSV infection [20]. McConnochie and Roghmann [21] reported that exposure to passive smoke may be an important risk factor for bronchiolitis in infants. In RSV infection, host immune responses including cellular immunity and humoral immunity are involved. Cellular immunity plays a key role in the clearance of RSV infection, and the immunopathogenesis of RSV bronchiolitis is affected by cellular immunity. However, neutralizing antibodies against RSV are not stable, and their levels decrease over time [22].
Respiratory Syncytial Virus
- COVID-19 and RSV infection are both infectious respiratory diseases, but they are caused by different viruses. It has been reported that children have a lower COVID-19 incidence rate than adults [23]. However, the real incidence of COVID-19 in children is unclear because of the lack of widespread diagnostic testing and the prioritization of testing for those with severe disease and adults. Studies showed that hospitalization for COVID-19 is more common among adults than among children, reflecting the higher severe illness rate in adults [24]. The susceptibility rate of children and adolescents to SARS-CoV-2 is lower than that of adults [25].
- RSV affects nearly all children in the first 2 years of life. It has been reported that about 0.5% to 2.0% of all children are hospitalized with lower respiratory tract illnesses, of whom 50% to 90% have lung infections and 5% to 40% show pneumonia [26]. RSV can infect people of all age groups, but infants, children under 2 years of age, and elderly people are at particularly high risk [27]. The mortality rate of RSV is higher than that of seasonal influenza infections [28]. In the general population, the frequency of RSV-positive hospitalizations is about 1% to 3%, although the proportion among premature infants is approximately 10% to 25% [29].
- Coinfection of RSV and SARS-CoV-2 may have a substantial effect on the treatment and prognosis of the disease. Viral coinfection may be associated with the need for a higher level of care, increased length of stay, and progression to ARDS [30]; furthermore, coinfection can result in more serious damage to the immune system [31]. In other words, patients with COVID-19 and other viruses have a more serious problem, their treatment is more complicated, and their treatment cycle is longer [32]. The progress and outcome of SARS-CoV-2 coinfections with other viruses including RSV are related to the host immune response [33,34].
- Several literature reviews have investigated coinfections of SARS-CoV-2 with other respiratory pathogens, such as RSV. Alvares [35] analysed 32 pediatric patients under 24 months of age hospitalized with COVID-19, and found that 18.7% of cases were coinfected with RSV. These patients had a significantly longer length of stay. However, no significant differences were observed in terms of the need for intensive care, mechanical ventilation, or mortality rate. In a study in Wuhan, among 250 patients diagnosed with COVID-19, RSV was detected in 12 patients (4.8%). That study showed that patients coinfected with viral pathogens had longer hospital stays than patients coinfected with atypical bacterial pathogens [36]. In the study of Hazra et al. [37] in 459 SARS-CoV-2-positive cases, there were no positive cases of RSV infection. In a study in Ontario, Canada that included 7,225 SARS-CoV-2-positive cases, 177 (2.4%) were coinfected with RSV. Their results showed that patients with viral coinfections were more likely to be younger than 65 years of age and male, and patients with SARS-CoV-2 coinfections mostly showed mild respiratory signs, including fever and cough [38].
Incidence of COVID-19 and RSV Infection in Children
- The mechanisms of viral coinfection may include virus-induced airway damage, reduced mucociliary clearance, and damage to the immune system [39]. Furthermore, several viruses can destroy the airway epithelium, which might lead to enhanced viral coinfection. Virus-associated immune system disorders can increase the risk of infection with other viruses [40,41].
Causes of Viral Coinfection
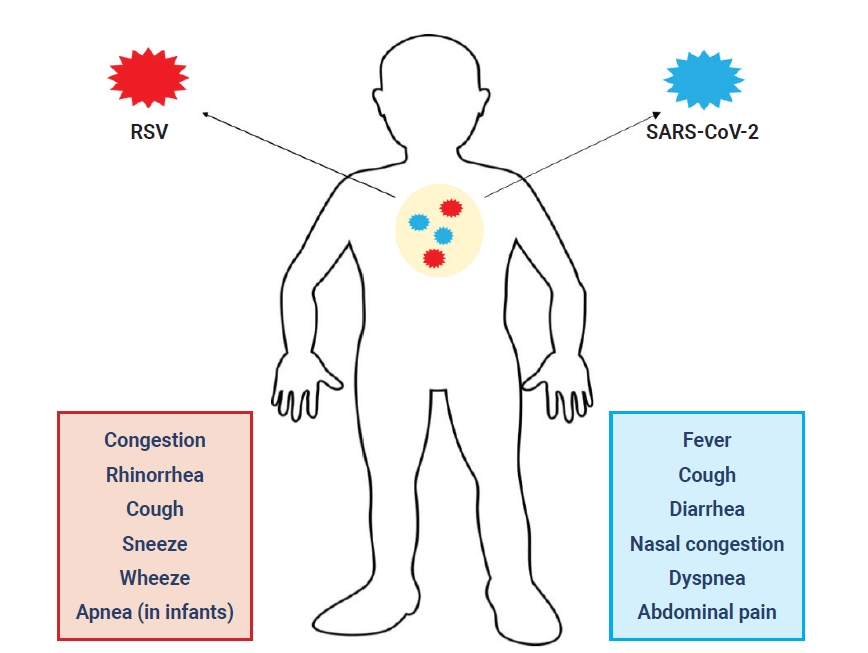
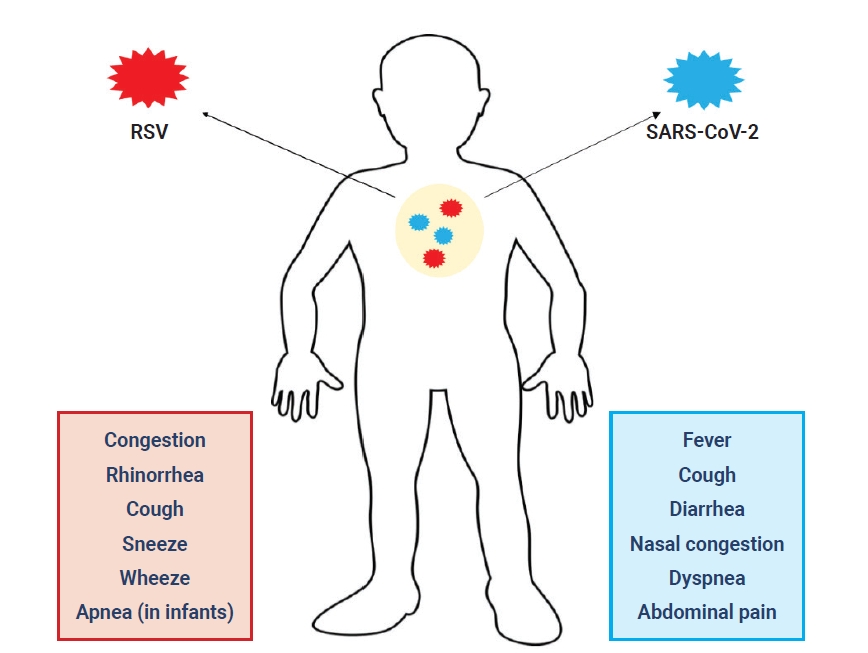
- The clinical manifestations of COVID-19 are milder in children than in adults [42]; however, fever, cough, diarrhea, nasal congestion, dyspnea, and abdominal pain are the most common symptoms of COVID-19 in children (Figure 1). The incubation period of SARS-CoV-2 is 2–5 days [43,44].
- Multisystem inflammatory syndrome in children (MIS-C) is a hyperinflammatory condition wherein various body parts can become inflamed, such as the heart, lungs, kidneys, brain, skin, eyes, or gastrointestinal organs [25]. MIS-C develops about 2 to 6 weeks after COVID-19 infection. The disease usually affects children with a median age of 8 years [45]. The presenting clinical features in children with MIS-C included persistent fever, abdominal pain, vomiting, diarrhea, cardiac dysfunction, rash, conjunctivitis, headache, and meningismus [46]. Although the specific risk factors for MIS-C are not well understood, it has been hypothesized that lower pre-existing immunity to coronaviruses can elevate individuals’ risk [47]. MIS-C is a progressive disease, and patients who initially have mild symptoms can progress to severe disease with multi-organ dysfunction within a few days of symptom/sign onset. Serious symptoms and signs can include hemodynamic instability, tachycardia, left ventricular dysfunction, and respiratory distress, which might be primary or caused by cardiac dysfunction [48]. The laboratory findings of MIS-C include lymphopenia, anemia, and thrombocytopenia; increased levels of liver enzymes, creatinine, pro-brain natriuretic protein, and troponin; and coagulation [49].
- RSV infection in young children is often mild in the early phase, but in children under 3 years of age, RSV may cause coughing, wheezing, congestion, rhinorrhea, sneezing, and apnea [49]. RSV is the most common cause of bronchiolitis and pneumonia in children under 1 year of age, and the incubation period of RSV is about 2 to 8 days [50]. In children, RSV can lead to severe respiratory disease requiring hospitalization, and causes death in some rare cases. Other RSV symptoms common among infants include listlessness, poor or diminished appetite, and fever [16–18]. RSV and COVID-19 coinfection may increase the severity of disease in children.
Symptoms of COVID-19 and RSV in Children
- The early and accurate diagnosis of SARS-CoV-2 is an important tool for limiting and controlling COVID-19. Contact with infected individuals is a key way to transmit SARS-CoV-2 in both children and adults [51].
- Molecular and serological tests are recommended by the Centers for Disease Control and Prevention to diagnose patients with SARS-CoV-2 infection. COVID-19 can result in significant alterations in the white blood cell count, elevated number of neutrophils and decreased number of lymphocytes have been reported in patients with severe COVID-19 [52]. Some laboratory predictors of COVID-19 have been identified in children, including increased or decreased levels of markers such as procalcitonin, D-dimer, and creatine kinase, as well as elevated liver enzymes [41].
- The radiological imaging findings of COVID-19 pneumonia include lung changes (e.g., ground-glass opacities), bronchial changes, and pleural changes. However, the symptoms and radiological findings are similar to other respiratory viral infections [53]. Hence, determining the type and number of viruses present in a patient based on imaging findings and the medical history may be difficult, and misdiagnoses of COVID-19 and other respiratory viruses are possible. Radiographic images and clinical signs can only be used as diagnostic auxiliaries, and patients cannot be diagnosed solely on the basis of these 2 modalities [54].
- Analyses of laboratory findings have shown that SARS-CoV-2 infection was associated with lymphopenia, prolonged prothrombin time, and elevated levels of lactate dehydrogenase, alanine aminotransferase, aspartate aminotransferase, D-dimer, neutrophils, eosinopenia, C-reactive protein, and troponin [55]. The most common laboratory data include a decreased lymphocyte count and increased high-sensitivity C-reactive protein levels. When combined with other viral infections, these results might change. Laboratory finding results are often influenced by the degree of disease progression and the pathogens that infect the patient, so they can only be used as a reference for diagnosing the disease [56]. Multiplex reverse transcription-polymerase chain reaction can simultaneously detect respiratory viruses such as SARS-CoV-2 and RSV. Nevertheless, this technique may cause some false-negative results because of certain factors during sample recovery, processing, or transportation. Thus, repeat nasopharyngeal testing is important for confirming the diagnosis [57].
- Computed tomography (CT) is used as another diagnostic tool for SARS-CoV-2, but it is less specific in children than in adults. The radiologic results in children with COVID-19 include unilateral or bilateral infiltrates and ground-glass opacities on CT [58].
- Two main predictors are important for the diagnosis of RSV infection: the physical examination and patient history. Children typically present with cough, rhinitis, and wheezing. Laboratory testing and chest radiography are not required for a diagnosis. The white blood cell count is not abnormal, but it may be increased in some cases. The results of chest radiography in children with bronchiolitis sometimes are abnormal [59]. Thus, laboratory tests and chest radiography are not routinely recommended for RSV infection.
SARS-CoV-2 and RSV Diagnosis in Children
- Combinations of antiviral agents and immunomodulators (oseltamivir + hydroxychloroquine + Kaletra [lopinavir + ritonavir]) are used to treat COVID-19 pneumonia in children [60], while RSV treatment is based on supportive care; however, palivizumab is recommended to prevent serious complications of RSV infection. Supportive care is the key treatment for RSV bronchiolitis [61]. Most infants can be managed at home, although hospitalization is necessary for children with RSV infection who are ill-appearing, have poor feeding, are dehydrated, have apnea, develop respiratory distress, or require supplemental oxygen [61].
- Supportive care includes hydration, using saline nose drops to clear nasal obstruction, suction with a nasal bulb in the hospital, and adequate nutrition for the patient. Oxygen is recommended in some cases to keep oxygen saturation >90% [62]. Mechanical ventilation is needed in some otherwise healthy infants with RSV infection who are hospitalized and infants with underlying diseases such as chronic lung disease, congenital heart disease, or immunosuppression [63].
SARS-CoV-2 and RSV Treatment in Children
- Both SARS-CoV-2 and RSV are infectious causes of respiratory disease in children. RSV and SARS-COV-2 coinfection in children can be considered a serious problem in the context of the COVID-19 pandemic. The pathogenicity of SARS-CoV-2 in children is unclear, but coinfection of RSV with SARS-CoV-2 may promote severe disease in children, as well as affecting the diagnosis and treatment of disease. Although several studies have investigated viral respiratory coinfections in COVID-19 patients, no study has evaluated the rate of RSV coinfection in SARS-CoV-2-positive samples from children. The clinical data of SARS-CoV-2 coinfection are of considerable value for the treatment of COVID-19. In patients with severe COVID-19, the rate of coinfections (e.g., RSV infection) is significantly higher than in those who have not been severely affected. Therefore, it is very important to prevent coinfection with SARS-CoV-2 and other viruses, including RSV, as a step towards preventing and controlling the spread of COVID-19. To prevent transmission, social distancing must be encouraged. In the process of diagnosing and treating patients with other viral infections, it is best to provide a separate room for specific individuals in the clinical setting so that they can be isolated and treated after evaluating the risk of transmission. These actions facilitate the accurate prevention and treatment of infectious complications and effective reduction of mortality in patients with COVID-19.
Conclusion
-
Ethics Approval
Not applicable.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
The current study was financially supported by Abadan University of Medical Sciences (Ethics No: IR.ABADANUMS.REC.1399.218).
-
Availability of Data
All data generated or analyzed during this study are included in this published article. For other data, these may be requested through the corresponding author.
-
Additional Contributions
Conceptualization: MZ; Data curation: SS, MF, SE; Investigation: SS, MF, AR; Supervision: SA; Writing–original draft: SS, MF, AR; Writing–review & editing: MZ, SA.
Article information
- 1. Salahshoori I, Mobaraki-Asl N, Seyfaee A, et al. Overview of COVID-19 disease: virology, epidemiology, prevention diagnosis, treatment, and vaccines. Biologics 2021;1:2−40.Article
- 2. Navand AH, Soltani S, Moghadami M, et al. Diabetes and coronavirus infections (SARS-CoV, MERS-CoV, and SARS-CoV-2). J Acute Dis 2020;9:244−7.Article
- 3. Matsuno AK, Gagliardi TB, Paula FE, et al. Human coronavirus alone or in co-infection with rhinovirus C is a risk factor for severe respiratory disease and admission to the pediatric intensive care unit: a one-year study in Southeast Brazil. PLoS One 2019;14:e0217744.ArticlePubMedPMC
- 4. Wahl B, O’Brien KL, Greenbaum A, et al. Burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in the era of conjugate vaccines: global, regional, and national estimates for 2000-15. Lancet Glob Health 2018;6:e744−57.ArticlePubMedPMC
- 5. Factor SH, LaClaire L, Bronsdon M, et al. Streptococcus pneumoniae and Haemophilus influenzae type B Carriage, Central Asia. Emerg Infect Dis 2005;11:1476−9.ArticlePubMedPMC
- 6. Hashemi SA, Safamanesh S, Ghasemzadeh-Moghaddam H, et al. Report of death in children with SARS-CoV-2 and human metapneumovirus (hMPV) coinfection: is hMPV the trigger? J Med Virol 2021;93:579−81.ArticlePubMed
- 7. Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet 2010;375:1545−55.ArticlePubMedPMC
- 8. Gavriatopoulou M, Korompoki E, Fotiou D, et al. Organ-specific manifestations of COVID-19 infection. Clin Exp Med 2020;20:493−506.ArticlePubMedPMC
- 9. Yang L, Liu S, Liu J, et al. COVID-19: immunopathogenesis and immunotherapeutics. Signal Transduct Target Ther 2020;5:128. ArticlePubMedPMC
- 10. Clark A, Jit M, Warren-Gash C, et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling study. Lancet Glob Health 2020;8:e1003−17.ArticlePubMedPMC
- 11. Moghadam SO, Afshar D. A review on coronavirus disease 2019 (COVID-19) in pediatric patients. Arch Pediatr Infect Dis 2020;8:e104225.Article
- 12. Lansbury L, Lim B, Baskaran V, et al. Co-infections in people with COVID-19: a systematic review and meta-analysis. J Infect 2020;81:266−75.ArticlePubMedPMC
- 13. Netea MG, Giamarellos-Bourboulis EJ, Dominguez-Andres J, et al. Trained immunity: a tool for reducing susceptibility to and the severity of SARS-CoV-2 infection. Cell 2020;181:969−77.ArticlePubMedPMC
- 14. Hall CB, Simoes EA, Anderson LJ. Clinical and epidemiologic features of respiratory syncytial virus. Curr Top Microbiol Immunol 2013;372:39−57.ArticlePubMed
- 15. Rima B, Collins P, Easton A, et al. ICTV virus taxonomy profile: pneumoviridae. J Gen Virol 2017;98:2912−13.ArticlePubMedPMC
- 16. Schweitzer JW, Justice NA. Respiratory syncytial virus infection. Treasure Island (FL): StatPearls Publishing LLC.; 2021.
- 17. Wennergren G, Kristjansson S. Relationship between respiratory syncytial virus bronchiolitis and future obstructive airway diseases. Eur Respir J 2001;18:1044−58.ArticlePubMed
- 18. Esteban I, Stein RT, Polack FP. A durable relationship: respiratory syncytial virus bronchiolitis and asthma past their golden anniversary. Vaccines (Basel) 2020;8:201. ArticlePubMedPMC
- 19. Falsey AR, Walsh EE. Respiratory syncytial virus infection in adults. Clin Microbiol Rev 2000;13:371−84.ArticlePubMedPMC
- 20. DiFranza JR, Masaquel A, Barrett AM, et al. Systematic literature review assessing tobacco smoke exposure as a risk factor for serious respiratory syncytial virus disease among infants and young children. BMC Pediatr 2012;12:81. ArticlePubMedPMC
- 21. McConnochie KM, Roghmann KJ. Wheezing at 8 and 13 years: changing importance of bronchiolitis and passive smoking. Pediatr Pulmonol 1989;6:138−46.ArticlePubMed
- 22. Domachowske JB, Rosenberg HF. Respiratory syncytial virus infection: immune response, immunopathogenesis, and treatment. Clin Microbiol Rev 1999;12:298−309.ArticlePubMedPMC
- 23. Leeb RT, Price S, Sliwa S, et al. COVID-19 trends among school-aged children: United States, March 1-September 19, 2020. MMWR Morb Mortal Wkly Rep 2020;69:1410−5.ArticlePubMedPMC
- 24. Swann OV, Holden KA, Turtle L, et al. Clinical characteristics of children and young people admitted to hospital with covid-19 in United Kingdom: prospective multicentre observational cohort study. BMJ 2020;370:m3249. ArticlePubMed
- 25. Godfred-Cato S, Bryant B, Leung J, et al. COVID-19-associated multisystem inflammatory syndrome in children: United States, March-July 2020. MMWR Morb Mortal Wkly Rep 2020;69:1074−80.ArticlePubMedPMC
- 26. Paes BA, Mitchell I, Banerji A, et al. A decade of respiratory syncytial virus epidemiology and prophylaxis: translating evidence into everyday clinical practice. Can Respir J 2011;18:e10−9.ArticlePubMedPMC
- 27. Walsh EE. Respiratory syncytial virus infection: an illness for all ages. Clin Chest Med 2017;38:29−36.PubMed
- 28. Kwon YS, Park SH, Kim MA, et al. Risk of mortality associated with respiratory syncytial virus and influenza infection in adults. BMC Infect Dis 2017;17:785. ArticlePubMedPMC
- 29. Newby B, Sorokan T. Respiratory syncytial virus infection rates with limited use of palivizumab for infants born at 29 to 31+6/7 weeks gestational age. Can J Hosp Pharm 2017;70:13−8.ArticlePubMedPMC
- 30. Chen X, Liao B, Cheng L, et al. The microbial coinfection in COVID-19. Appl Microbiol Biotechnol 2020;104:7777−85.ArticlePubMedPMC
- 31. Tay MZ, Poh CM, Renia L, et al. The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol 2020;20:363−74.ArticlePubMedPMC
- 32. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 2020;8:475−81.ArticlePubMedPMC
- 33. Coutinho A, Riaz A, Makan A, et al. Lessons of the month: co-infection with SARS-CoV-2 and influenza B virus in a patient with community-acquired pneumonia. Clin Med (Lond) 2020;20:e262−3.ArticlePubMedPMC
- 34. Zhu X, Ge Y, Wu T, et al. Co-infection with respiratory pathogens among COVID-2019 cases. Virus Res 2020;285:198005. ArticlePubMedPMC
- 35. Alvares PA. SARS-CoV-2 and respiratory syncytial virus coinfection in hospitalized pediatric patients. Pediatr Infect Dis J 2021;40:e164−6.ArticlePubMed
- 36. Ma L, Wang W, Le Grange JM, et al. Coinfection of SARS-CoV-2 and other respiratory pathogens. Infect Drug Resist 2020;13:3045−53.PubMedPMC
- 37. Hazra A, Collison M, Pisano J, et al. Coinfections with SARS-CoV-2 and other respiratory pathogens. Infect Control Hosp Epidemiol 2020;41:1228−9.ArticlePubMed
- 38. Peci A, Tran V, Guthrie JL, et al. Prevalence of co-infections with respiratory viruses in individuals investigated for SARS-CoV-2 in Ontario, Canada. Viruses 2021;13:130. ArticlePubMedPMC
- 39. Clementi N, Ghosh S, De Santis M, et al. Viral respiratory pathogens and lung injury. Clin Microbiol Rev 2021;34:e00103. −20.ArticlePubMedPMC
- 40. Huang I, Pranata R, Lim MA, et al. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: a meta-analysis. Ther Adv Respir Dis 2020;14:1753466620937175. ArticlePubMedPMC
- 41. Ponti G, Maccaferri M, Ruini C, et al. Biomarkers associated with COVID-19 disease progression. Crit Rev Clin Lab Sci 2020;57:389−99.ArticlePubMed
- 42. Ludvigsson JF. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr 2020;109:1088−95.ArticlePubMedPMC
- 43. Mantovani A, Rinaldi E, Zusi C, et al. Coronavirus disease 2019 (COVID-19) in children and/or adolescents: a meta-analysis. Pediatr Res 2021;89:733−7.ArticlePubMed
- 44. Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med 2020;172:577−82.ArticlePubMed
- 45. Consiglio CR, Cotugno N, Sardh F, et al. The immunology of multisystem inflammatory syndrome in children with COVID-19. Cell 2020;183:968−81.ArticlePubMedPMC
- 46. Hennon TR, Penque MD, Abdul-Aziz R, et al. COVID-19 associated Multisystem Inflammatory Syndrome in Children (MIS-C) guidelines; a Western New York approach. Prog Pediatr Cardiol 2020;57:101232. Article
- 47. Diorio C, Henrickson SE, Vella LA, et al. Multisystem inflammatory syndrome in children and COVID-19 are distinct presentations of SARS-CoV-2. J Clin Invest 2020;130:5967−75.ArticlePubMedPMC
- 48. Feldstein LR, Tenforde MW, Friedman KG, et al. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA 2021;325:1074−87.ArticlePubMed
- 49. Simpson JM, Newburger JW. Multisystem inflammatory syndrome in children in association with COVID-19. Circulation 2020;142:437−40.ArticlePubMed
- 50. Piedimonte G, Perez MK. Respiratory syncytial virus infection and bronchiolitis. Pediatr Rev 2014;35:519−30.ArticlePubMedPMC
- 51. Cheng MP, Papenburg J, Desjardins M, et al. Diagnostic testing for severe acute respiratory syndrome-related coronavirus 2: a narrative review. Ann Intern Med 2020;172:726−34.PubMed
- 52. Kubankova M, Hohberger B, Hoffmanns J, et al. Physical phenotype of blood cells is altered in COVID-19. Biophysical Journal 2021;120:2838−47.Article
- 53. Carotti M, Salaffi F, Sarzi-Puttini P, et al. Chest CT features of coronavirus disease 2019 (COVID-19) pneumonia: key points for radiologists. Radiol Med 2020;125:636−46.ArticlePubMedPMC
- 54. Chen H, Ai L, Lu H, et al. Clinical and imaging features of COVID-19. Radiol Infect Dis 2020;7:43−50.ArticlePubMedPMC
- 55. Siordia JA Jr. Epidemiology and clinical features of COVID-19: a review of current literature. J Clin Virol 2020;127:104357. ArticlePubMedPMC
- 56. Ghahramani S, Tabrizi R, Lankarani KB, et al. Laboratory features of severe vs. non-severe COVID-19 patients in Asian populations: a systematic review and meta-analysis. Eur J Med Res 2020;25:30. ArticlePubMedPMC
- 57. Kubina R, Dziedzic A. Molecular and serological tests for COVID-19: a comparative review of SARS-CoV-2 coronavirus laboratory and point-of-care diagnostics. Diagnostics (Basel) 2020;10:434. ArticlePubMedPMC
- 58. Shelmerdine SC, Lovrenski J, Caro-Dominguez P, et al. Coronavirus disease 2019 (COVID-19) in children: a systematic review of imaging findings. Pediatr Radiol 2020;50:1217−30.ArticlePubMedPMC
- 59. Dawson-Caswell M, Muncie HL Jr. Respiratory syncytial virus infection in children. Am Fam Physician 2011;83:141−6.PubMed
- 60. Karimi A, Rafiei Tabatabaei S, et al. An algorithmic approach to diagnosis and treatment of coronavirus disease 2019 (COVID-19) in children: Iranian Expert’s Consensus Statement. Arch Pediatr Infect Dis 2020;8:e102400.Article
- 61. Eiland LS. Respiratory syncytial virus: diagnosis, treatment and prevention. J Pediatr Pharmacol Ther 2009;14:75−85.ArticlePubMedPMC
- 62. American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics 2006;118:1774−93.ArticlePubMedPDF
- 63. Roque i Figuls M, Gine-Garriga M, Granados Rugeles C, et al. Chest physiotherapy for acute bronchiolitis in paediatric patients between 0 and 24 months old. Cochrane Database Syst Rev 2016;2:CD004873. PubMed
References
Figure & Data
References
Citations
- Results from the second WHO external quality assessment for the molecular detection of respiratory syncytial virus, 2019–2020
Thomas Williams, Sandra Jackson, Ian Barr, Shabana Bi, Jinal Bhiman, Joanna Ellis, Anne von Gottberg, Stephen Lindstrom, Teresa Peret, Sanjiv Rughooputh, Mariana Viegas, Siddhivinayak Hirve, Maria Zambon, Wenqing Zhang
Influenza and Other Respiratory Viruses.2023;[Epub] CrossRef - The Impact of Coronavirus Disease 2019 on Viral, Bacterial, and Fungal Respiratory Infections
Ashley Losier, Gayatri Gupta, Mario Caldararo, Charles S. Dela Cruz
Clinics in Chest Medicine.2023; 44(2): 407. CrossRef - Viral Coinfection of Children Hospitalized with Severe Acute Respiratory Infections during COVID-19 Pandemic
Célia Regina Malveste Ito, André Luís Elias Moreira, Paulo Alex Neves da Silva, Mônica de Oliveira Santos, Adailton Pereira dos Santos, Geovana Sôffa Rézio, Pollyanna Neta de Brito, Alana Parreira Costa Rezende, Jakeline Godinho Fonseca, Fernanda Aparecid
Biomedicines.2023; 11(5): 1402. CrossRef - Clinical Relevance of RSV and SARS-CoV-2 Coinfections in Infants and Young Children
Rosa Rodriguez-Fernandez, Felipe González-Martínez, Jimena Perez-Moreno, María Isabel González-Sánchez, Blanca Toledo del Castillo, Irene Mingueza de la Paz, Laura Diaz Pozo, Asuncion Mejias, Octavio Ramilo
Pediatric Infectious Disease Journal.2023; 42(12): e473. CrossRef - Targeting host calcium channels and viroporins: a promising strategy for SARS-CoV-2 therapy
Mona Fani, Maryam Moossavi, Hasan Bakhshi, Abozar Nasiri Jahrodi, Mohammad Reza Khazdair, Amir Hossein Zardast, Shokouh Ghafari
Future Virology.2023; 18(12): 797. CrossRef - Respiratory syncytial virus, recurrent wheeze and asthma: A narrative review of pathophysiology, prevention and future directions
Elly Binns, Jane Tuckerman, Paul V Licciardi, Danielle Wurzel
Journal of Paediatrics and Child Health.2022; 58(10): 1741. CrossRef - Impact of genetic polymorphisms related to innate immune response on respiratory syncytial virus infection in children
Laura Elena Córdova-Dávalos, Alicia Hernández-Mercado, Claudia Berenice Barrón-García, Augusto Rojas-Martínez, Mariela Jiménez, Eva Salinas, Daniel Cervantes-García
Virus Genes.2022; 58(6): 501. CrossRef - Clinical and epidemiological characteristics of SARS-CoV-2 virus in ambulatory children under 2 years old
Carolina A. Perez, Ivana Ormazabal, Javier Pérez-Valenzuela, Andrea Araya, Rafael A. Medina, Cecilia Perret
Frontiers in Pediatrics.2022;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite