Abstract
-
Objectives
- This study evaluated the validity and reliability of the Health-Related Quality of Life Instrument with 8 Items (HINT-8) in postoperative breast cancer patients in South Korea.
-
Methods
- The study included 300 breast cancer patients visiting a tertiary hospital. We measured health-related quality of life (HRQoL) using the HINT-8, the 5-level EQ-5D version (EQ-5D-5L), and the Functional Assessment of Cancer Therapy-Breast (FACT-B). Discriminatory ability, known-group validity, and convergent validity were assessed. Reliability was evaluated with the Cohen kappa, weighted kappa, and intraclass correlation coefficient (ICC).
-
Results
- The EQ-5D-5L indexes (p<0.001) and EQ visual analogue scale (VAS) scores (p<0.001) were significantly higher in subjects with no problems in each item of the HINT-8 than in those with problems. The FACT-B total scores were also higher in subjects without problems on the HINT-8. Older age, lower education level, and comorbidities were associated with a lower HINT-8 index. The HINT-8 index was correlated with the EQ-5D-5L index and the EQ VAS, with correlation coefficients of 0.671 (p<0.001) and 0.577 (p<0.001), respectively. The correlation coefficients between the HINT-8 and the FACT-B ranged from 0.390 to 0.714. The ICC was 0.690 (95% confidence interval, 0.580–0.780).
-
Conclusion
- The HINT-8 showed appropriate validity for capturing HRQoL in postoperative breast cancer patients.
-
Keywords: Breast neoplasms; Quality of life; Reproducibility of results
Introduction
- Breast cancer has high incidence and mortality rates, ranking first and fifth in incidence and mortality in world cancer statistics in 2020 [1]. In Korea, breast cancer was the type of cancer with the highest incidence in women in 2016, followed by thyroid cancer [2]. While the age-standardized incidence rate increased from 24.5 (per 100,000 people) in 1999 to 62.5 in 2016, the 5-year observed survival also showed an increasing tendency between 2012 and 2016 [2,3]. Accordingly, assessing health-related quality of life (HRQoL) is critical for capturing patients’ experiences, in addition to traditional epidemiological measures such as mortality and survival rates.
- There are 2 types of HRQoL measures: generic and disease-specific. Disease-specific instruments, such as the European Organization for Research and Treatment of Cancer quality of life questionnaire (EORTC QLQ-C30), focus on issues related to a specific illness, whereas generic instruments assess overall health status in a wide range of populations, including healthy individuals [4]. Generic preference-based measures, such as the EQ-5D or the Short Form 6D, are widely used as a trial end-point and to generate utility estimates for economic evaluations [5,6]. However, the broad application of these generic instruments has been criticized due to cultural differences [7]. In light of this criticism, the Health-Related Quality of Life Instrument with 8 Items (HINT-8) was developed to fit the Korean context [8,9].
- The psychometric properties of the HINT-8, a generic preference-based instrument, have been studied in the Korean general population [9]. In addition, its value set (a set of preference weights) was developed for use in the Korean population [10]. The HINT-8 can be used to estimate utility weights using this value set in economic evaluations. The Korea National Health and Nutrition Examination Survey (KNHANES), a national surveillance program assessing participants’ health and nutritional status, has adopted the HINT-8 to evaluate quality of life since 2019. However, no study has yet investigated the validity and reliability of the HINT-8 in disease-specific populations, such as individuals with cancer. The psychometric properties of the HINT-8 in disease-specific populations should be studied to expand its use for decision-making in the healthcare sector. Therefore, we evaluated the validity and reliability of the HINT-8 in postoperative breast cancer patients in Korea.
Materials and Methods
- Subjects and Study Setting
- We recruited a consecutive series of 300 breast cancer patients in the ambulatory or inpatient care setting of a tertiary hospital in Seoul, South Korea between April and June in 2018. The target population was women (aged ≥30 y) who underwent surgery as a primary treatment for breast cancer. We only included female patients due to the substantial differences between male and female breast cancer, including the rare incidence of this condition in men [3]. Considering differences in patients’ characteristics according to the postoperative duration, we categorized the population into 3 groups: group 1 (2–4 days after surgery, n=50), group 2 (within 5 years after surgery, n=150), and group 3 (more than 5 years after surgery, n=100). After obtaining written informed consent from each patient, a paper-based survey was conducted by a trained interviewer in the survey. After 1 to 4 weeks, 100 consecutive participants from the first survey were followed up through a telephone-based survey administered by the same interviewer. Considering fluctuations in HRQoL status during the immediate perioperative period [11], subjects in group 1 (2–4 days after surgery) were excluded from the retest for reliability assessment. The institutional review board of Asan Medical Center approved the study (No. 2018-0026).
- Data Collection and HRQoL Assessment
- Primary background information about demographics (age, education level, marital status, monthly household income, outpatient visit, hospitalization, and self-rated health) and clinical characteristics (duration of disease, surgery type, current treatment, and comorbidities) was collected from all participating subjects. The HINT-8, as the generic HRQoL instrument of interest, and other widely used instruments including the 5-level EQ-5D version (EQ-5D-5L) and the Functional Assessment of Cancer Therapy-Breast (FACT-B) were used in the initial and follow-up surveys [12,13].
- The HINT-8 consists of 8 items (climbing stairs, pain, vitality, working, depression, memory, sleep, and happiness) and 4 levels (no problems, mild, moderate, and severe problems) representing 65,536 health states [8,9], which is a far higher number of states than the 3,125 states gathered by the EQ-5D-5L [14]. The HINT-8 scores range from 0.132 (worst possible health state, 44444444) to 1.000 (best possible health state, 11111111), and the index can be derived from the previously developed value set [10]. The EQ-5D-5L comprises 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and 5 levels (no problems, slight problems, moderate problems, severe problems, and extreme problems) [14]. To derive a utility index from the descriptive system of the EQ-5D-5L, we used the tariff developed in Korea [15,16]. The EQ-5D-5L utility scores using the Korean tariff range from −0.066 (worst possible health state, 55555) to 1 (best possible health state, 11111), with a higher score indicating better health status. In addition to the EQ-5D-5L descriptive system, participants’ overall current health status was assessed with the EQ visual analogue scale (EQ VAS) [14]. The EQ VAS ranges from 0 (worst imaginable health state) to 100 (best imaginable health state). The Korean version 4 of FACT-B, a disease-specific instrument, was also used to confirm the validity of the HINT-8 in the population of Korean breast cancer patients [13,17]. The FACT-B consists of 5 subscales: physical well-being (PWB; score range, 0–28), social/family well-being (SWB; score range, 0–28), emotional well-being (EWB; score range, 0–24), functional well-being (FWB; score range, 0–28), and the breast cancer subscale (BCS; score range, 0–40). The FACT-B trial outcome index (TOI; score range, 0–96), FACT-General (FACT-G) total score (score range, 0–108), and FACT-B total score (score range, 0–148) are derived as follows: (1) FACT-B TOI=PWB score+FWB score+BCS score; (2) FACT-G total score=PWB score+SWB score+EWB score+FWB score; and (3) FACT-B total score=PWB score+SWB score+EWB score+FWB score+BCS score. In the FACT-B, a higher score represents better quality of life.
- Statistical Analyses
- The distribution of responses in each level of the different instruments was calculated, and the ceiling effect of the HINT-8 was examined in comparison with the EQ-5D-5L. To determine the discriminatory ability of the HINT-8, the mean scores of the different measures (EQ-5D-5L index, EQ VAS, and FACT-B total) were compared according to the presence of problems (without problems vs. with problems). The group with problems included participants with mild, moderate, or severe problems, whereas those who reported no problems were included in the group without problems. Regarding discriminative validity, it was assumed that the group reporting problems in the HINT-8 had a poor health state in other HRQoL instruments. To demonstrate the known-group validity of the HINT-8, the HINT-8 index score was evaluated according to sociodemographic and clinical features. We hypothesized that the HINT-8 index would be lower in older and less educated groups [18]. We also evaluated the EQ-5D-5L index scores between relevant groups, and then calculated the relative efficiency (RE) to compare the efficiency of 2 generic instruments to capture relevant differences in breast cancer patients [19]. The RE was defined as the ratio of the squared t statistics (t2HINT-8/t2EQ-5D-5L) or the ratio of ANOVA F statistics (FHINT-8/FEQ-5D-5L).
- To evaluate convergent validity, the associations of the HINT-8 with the EQ-5D-5L and FACT-B were examined. It was assumed that a specific item of the HINT-8 would correlate more strongly with conceptually relevant categories of the other instruments (i.e., EQ-5D-5L dimensions and FACT-B subscales) than with unrelated ones. The Cohen kappa, weighted kappa coefficient, and intraclass correlation coefficient (ICC) were calculated to identify the reliability of the HINT-8, including individual items and the utility index [20]. A p-value less than 0.05 was considered to indicate statistical significance. Statistical analyses were performed using SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
- Subject Characteristics
- The ages of subjects in the baseline and follow-up tests were 54.4±9.1 and 54.4±8.6 years, respectively (Table 1). Regarding the education level, the largest proportion (46.0%) of participants in the first survey had a university degree or higher, whereas the largest group in the follow-up survey (45.0%) had a secondary education level. The proportion of married participants was 79.7% and 79.0%, respectively. The average monthly household income (Korean won, KRW) was slightly higher in the baseline population than in the retest population (5,080,000±5,160,000 vs. 4,920,000±5,570,000 KRW). The duration of disease after diagnosis was 4.2±4.0 years in the first paper-based survey and 4.8±3.7 years in the second telephone-based survey. Patients who underwent partial mastectomy accounted for the largest proportion of participants in the baseline and follow-up groups (69.7% and 72.0%, respectively). In both rounds of tests, the proportion of patients undergoing current treatment was similar (46.3% vs. 49.0%). The proportions of participants with any comorbidities were 36.7% and 41.0% in the baseline and follow-up tests, respectively.
- Distribution of Responses to HRQoL Instruments
- The response distribution of individual HINT-8 items is shown in Figure 1A. In the HINT-8, more than 90% of the responses to the items of climbing stairs, pain, working, depression, and memory corresponded to levels 1 and 2 in the first survey, whereas the proportion of responses of levels 1 to 3 was over 90% for the vitality, sleep, and happiness items. The HINT-8 indexes were similar in the first and second surveys (0.801±0.095 vs. 0.813±0.091). The average EQ-5D-5L index was slightly higher than the HINT-8 indexes in both the test and retest results (0.850±0.117 vs. 0.881±0.115). In terms of descriptive responses to the EQ-5D-5L, 89.2% to 94.4% of participants responded with levels 1 and 2, except in the domain of self-care in the first round, and 88.0% to 95.0% in the second round of tests (Figure 1B); 92.0% and 91.0% of respondents reported no problems (level=1) for the item of self-care. The mean±standard deviation (SD) of the total score of the FACT-B was 104.76±20.73 and the TOI was 68.16±13.66 in the baseline test (Figure 1C).
- In the EQ-5D-5L, 21.0% of respondents reported the best possible health state (11111), whereas only 2.3% reported the best health state (11111111) in the HINT-8 (Table S1). The EQ VAS score of subjects who reported the best possible health state in the HINT-8 was 4.63 points higher than that of subjects with the corresponding state in the EQ-5D-5L. The respondents reporting the best possible health state in the HINT-8 showed higher FACT-B scores than those with a perfect health state in the EQ-5D-5L. The FACT-B total scores differed by 6.03 between subjects who reported a perfect health status in the 2 HRQoL instruments (i.e., HINT-8 and EQ-5D-5L).
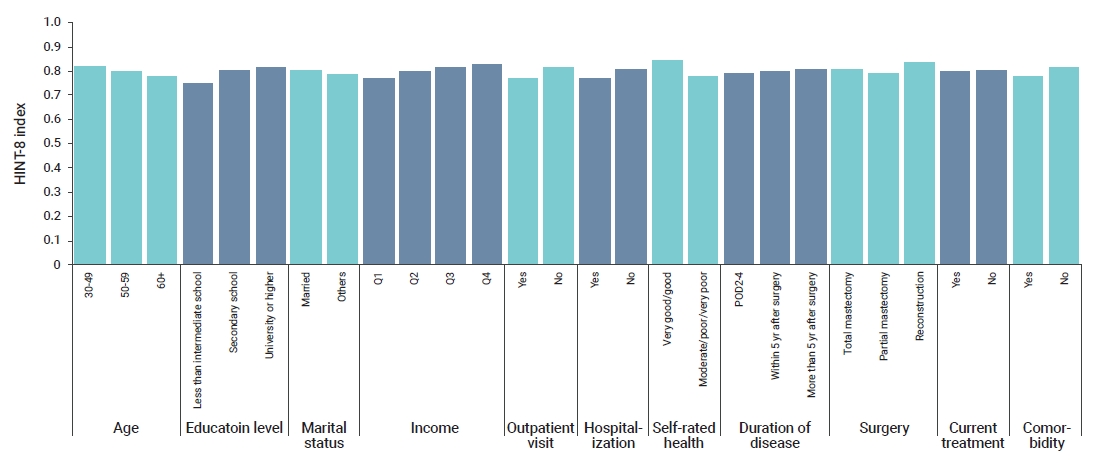
- Validity and Reliability
- The results of discriminatory ability testing showed that subjects who reported no problems on the HINT-8 had higher scores in the EQ-5D-5L and EQ VAS than those with problems, and the differences were significant (p<0.001) (Table 2). The discriminatory ability of the HINT-8 was also demonstrated in the FACT-B measures, and the differences were mostly significant, except in the memory and sleep items of the HINT-8 (Figure S1). The results of the test for determining the differences between groups to evaluate known-group validity are presented in Figure 2 (HINT-8) and Figure S2 (EQ-5D-5L). The results were consistent with the hypotheses for the HINT-8: older patients and less educated patients had significantly lower HINT-8 indexes than those in other groups. The current treatment group had a slightly lower HINT-8 index than the others (0.794 vs. 0.804), although the difference was not statistically significant (p=0.755). There was a trend toward lower HINT-8 index scores in subjects with comorbidities than in subjects without any comorbidity, but this trend did not reach statistical significance (0.779 vs. 0.811, p=0.059). In terms of EQ-5D-5L, while the results were consistent with our hypotheses for age groups (age 30–49 y, 0.848; age 50–59 y, 0.842; age ≥60 y, 0.827; p=0.493) and comorbidities (yes, 0.813; no, 0.855; p<0.001), there were no significant differences according to education level and marital status, income, and current treatment. The HINT-8 showed better known-group validity than the EQ-5D-5L. The RE statistic was more than 1, denoting better efficiency, for the following characteristics: age groups (RE=4.63), level of education (RE=7.20), monthly household income (RE=2.47), self-rated health (RE=1.59), and current treatment (RE=8.09). However, the RE values were lower for marital status (RE=0.69), hospitalization (RE=0.94), duration of disease (RE=0.11), and comorbidities (RE=0.96), implying poor efficiency of the HINT-8 compared to the EQ-5D-5L. The RE measures of several characteristics indicated similar efficiency (outpatient visit, RE=1.21; surgery, RE=1.05). The results of the correlation analysis between the HINT-8 and the other instruments are presented in Tables 3 and 4. The climbing stairs item showed an almost strong correlation with the mobility domain of the EQ-5D-5L (r=0.493, p<0.001). The working item of the HINT-8 showed moderate to strong correlations with the dimensions of mobility, usual activities, and pain/discomfort. There was a strong correlation between the depression item of the HINT-8 and the anxiety/depression domain of the EQ-5D-5L indexes (r=0.727, p<0.001). The happiness item in the HINT-8 was strongly correlated with the anxiety/depression domain of the EQ-5D-5L (r=0.511, p<0.001). The HINT-8 index was moderately correlated with individual domains of the EQ-5D-5L (from –0.581 to –0.435) except the self-care domain (r=–0.158). The correlation coefficients of the HINT-8 index with EQ-5D-5L and EQ VAS were 0.671 and 0.577, respectively. The pain and working items in the HINT-8 had a strong relationship with the PWB subscale of the FACT-B (–0.582 and –0.566, respectively). The depression item of the HINT-8 had a strong correlation with the EWB subscale, as well as the FACT-G, FACT-B total score, and TOI. The happiness item of the HINT-8 was strongly correlated with the FWB subscale, in addition to the FACT-G, FACT-B total score, and TOI. In general, there were strong correlations between the HINT-8 indexes and FACT-B subscales and other aggregated scores (i.e., TOI, FACT-G total, and FACT-B total), whereas there was a relatively moderate correlation (r=0.390) between the HINT-8 index and SWB.
- Agreement between surveys ranged from 43.0% to 70.0% (Table 5). The Cohen kappa coefficients of individual items in the HINT-8 ranged from 0.134 to 0.436 and the weighted kappa ranged from 0.249 to 0.513, indicating fair agreement except for the vitality item. The ICC of the HINT-8 index was 0.690 (95% confidence interval [CI], 0.580–0.780).
Discussion
- This study compared the psychometric properties of the HINT-8, a newly developed general HRQoL instrument targeting the Korean population, with widely used generic and disease-specific HRQoL instruments. The comparative analysis between subjects with no problems and those with problems on the HINT-8 showed significant differences in the EQ-5D-5L index, EQ VAS, and FACT-B total score; groups reporting no problems had higher scores than the others. The results are interpreted as showing that the response levels of the HINT-8 meaningfully distinguish between the levels of specific health states. The results of known-group validity were consistent with those of a previous validity study of the EQ-5D-3L with respect to age and education level [5,21]. The hypotheses related to the known-group validity of the HINT-8 were mostly verified; younger, more highly educated subjects and patients with a longer disease duration showed a better HRQoL status. However, the differences between patients according to the duration of disease were not significant (p=0.471). This non-significant difference was also observed in clinical features such as current treatment and comorbidities. The lack of statistical significance may be related to the small sample sizes of individual subgroups, which occurred because of resource restrictions and efforts to recruit a wide spectrum of patients with different HRQoL statuses based on previous studies [22–26]. Considering the RE statistics between the HINT-8 and the EQ-5D-5L, the HINT-8 showed better or similar known-group validity for most characteristics (RE statistics, range: 0.69–8.09), with the only exception being the duration of disease (RE=0.11).
- The comparison between the HINT-8 and the EQ-5D-5L showed strong correlations between the 2 relevant areas such as pain and depression (r=0.600 and r=0.727, respectively). Moreover, the correlation between the utility indexes of the 2 generic instruments (i.e., HINT-8 and EQ-5D-5L) was also strong (r=0.671). The correlation coefficients between the HINT-8 index and the FACT-B (FACT-B subscales and total score) were 0.390–0.731 in current study. In previous studies, the correlations between the EQ-5D-3L index and FACT-B were strongest in SWB and weakest in FACT-B total scores, with ranges of 0.11–0.56 reported by Lee et al. [27] and 0.199–0.557 by Kim et al. [5], respectively. The HINT-8 showed a good correlation with the EQ-5D-5L in general. In addition, correlations of the HINT-8 with the FACT-B were better than the EQ-5D-3L. The results support the feasibility of using the HINT-8 instead of the EQ-5D-5L, a currently widely used tool in decision-making such as economic evaluations in patients with breast cancer.
- The reliability of the categorical variables of the HINT-8 was acceptable, with weighted kappa coefficients of 0.249–0.513; using the cutoff points proposed by Landis and Koch [28], these values are interpreted as indicating fair or moderate agreement [29,30]. The overall Cohen kappa values derived from this study were lower than those of a previous study in the general population (0.565–0.799) [10]. The ICC of the HINT-8 index between the test and the retest (0.690; 95% CI, 0.580–0.780) was also to some extent lower than the outcomes derived from the HINT-20 and the HINT-8 (0.813 and 0.853, respectively) [10,20]. These inconclusive results regarding reliability may be attributed to differences in the survey administration methods between the baseline and the follow-up survey. A similar pattern was reported in the prior study of the EQ-5D-5L that used different survey administration methods; the kappa values of individual domains of the EQ-5D-5L ranged from 0.206 to 0.446 and the ICC was 0.626 [30]. Although the telephone interview method has been reported as equivalent to patient-completed surveys, variations in the agreement between individual domain scores were reported by Chatterji et al. [31].
- A strength of the HINT-8 is the inclusion of a greater number of health states (65,536 health states) than those included in commonly used generic tools such as EQ-5D-3L and EQ-5D-5L [9,10]. Compared with the EQ-5D-5L, the HINT-8 showed good properties related to the ceiling effect. Only 2.3% of participants reported a perfect health state in the HINT-8, whereas the corresponding proportion was 21.0% in the EQ-5D-5L. In addition, the EQ VAS score of the group with the full health state measured by the HINT-8 was higher than in the EQ-5D-5L (EQ VAS 93.00 vs. 88.37, respectively). These results indicate that the HINT-8 may be a more elaborate tool representing diverse health states that is superior for capturing changes in HRQoL among relatively healthy individuals. Considering the proper level of validity and better results in certain aspects including more informative health states, the HINT-8 is a usable tool to evaluate HRQoL in patients with breast cancer.
- Despite the overall good psychometric properties of the HINT-8, this study has several limitations. First, the results should be generalized with caution because all subjects were recruited consecutively in either the ambulatory or inpatient units of a single tertiary hospital. Second, patients were enrolled into 3 subgroups according to the duration of disease (group 1, 2–4 days after surgery; group 2, within 5 years after surgery; group 3, more than 5 years after surgery) with predesignated numbers of samples in each subgroup. Resource restrictions and the variety of patients with clinical conditions affecting HRQoL resulted in small sizes in the different groups. Lastly, the use of different survey methods in the baseline and the follow-up tests may have affected the reliability of the results. The first test consisted of a paper-based survey administered in the hospital setting, including outpatient clinics and inpatient wards, whereas the follow-up survey was conducted through personal mobile devices. The use of mobile devices implies that participants were in a variety of locations at the time of the second survey, which might have affected the reliability of the test. The use of the same survey mode may improve the reliability of the instruments in future studies. Furthermore, future studies are needed both to assess the impact of different survey methods and to investigate tactics for minimizing the effects resulting from the use of different survey methods.
- In conclusion, our study showed the HINT-8 is applicable to Korean women recovering from breast cancer surgery as a measurement of HRQoL. In particular, the HINT-8 showed better properties than the EQ-5D-5L in certain aspects such as known-group validity. Considering the inconclusive findings regarding reliability, its reliability should be more investigated in further research.
Supplementary Material
Table S1: Analysis of ceiling effects; Figure S1: Difference of FACT-B score between groups reporting with problems and without problems for each HINT-8 item; Figure S2: Mean scores of EQ-5D indexes according to general and clinical characteristics. Supplementary data are available at https://doi.org/10.24171/j.phrp.2021.0005.
Figure S1.
Difference of FACT-B score between groups reporting with problems and without problems for each HINT-8 item. PWB, physical well-being; SWB, social/family well-being; EWB, emotional well-being; FWB, functional well-being; BCS, breast cancer subscale; FACT-B, Functional Assessment of Cancer Therapy-Breast; TOI, trial outcome index; FACT-G, Functional Assessment of Cancer Therapy-General; HINT-8, Health-Related Quality of Life Instrument with 8 Items.
j-phrp-2021-0005-suppl2.pdf
Figure S2.
Mean scores of EQ-5D indexes according to general and clinical characteristics. POD, postoperative day. *p<0.05.
j-phrp-2021-0005-suppl3.pdf
Article information
-
Ethics Approval
The institutional review board of Asan Medical Center approved the study (No. 2018-0026). The written informed consent was obtained from all subjects prior to participating in the study.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2015R1D1A1A01059426).
-
Availability of Data
All data generated or analyzed during this study are included in this published article and its supplementary information files. For other data, these may be requested through the corresponding author.
-
Authors’ Contributions
Conceptualization: MWJ, HJL, JWL; Data curation: JK, SHA, BHS, JWL, SBL; Formal Analysis: JK; Funding acquisition: MWJ; Investigation: all authors; Methodology: MWJ, HJL, JWL; Project administration: JK, HJL; Supervision: MWJ; Writing–original draft: JK; Writing–review & editing: all authors.
Figure 1.Response distribution of the HINT-8, EQ-5D-5L, and FACT-B. (A) HINT-8, (B) EQ-5D-5L, (C) FACT-B. HINT-8, Health-Related Quality of Life Instrument with 8 Items; EQ-5D-5L, 5-level EQ-5D; FACT-B, Functional Assessment of Cancer Therapy-Breast; PWB, physical well-being; SWB, social/family well-being; EWB, emotional well-being; FWB, functional well-being; BCS, breast cancer subscale; TOI, trial outcome index; FACT-G, Functional Assessment of Cancer Therapy-General.
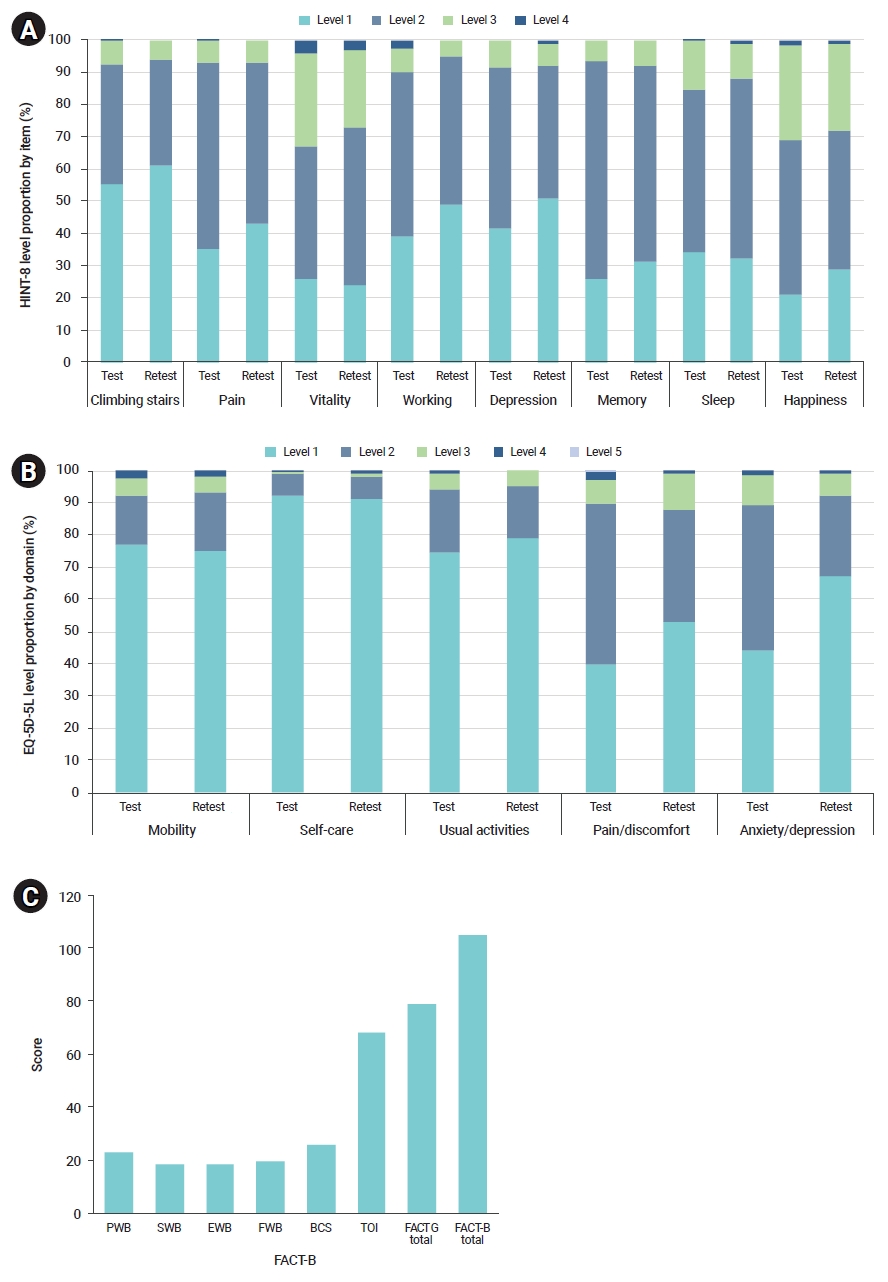
Figure 2.Mean scores of HINT-8 indexes according to general and clinical characteristics. All p-values less than 0.05 except marital status (p=0.760), duration of disease (p=0.471), current treatment (p=0.755), and comorbidities (p=0.059). HINT-8, Health-Related Quality of Life Instrument with 8 Items; Q, quartile; POD, postoperative day.
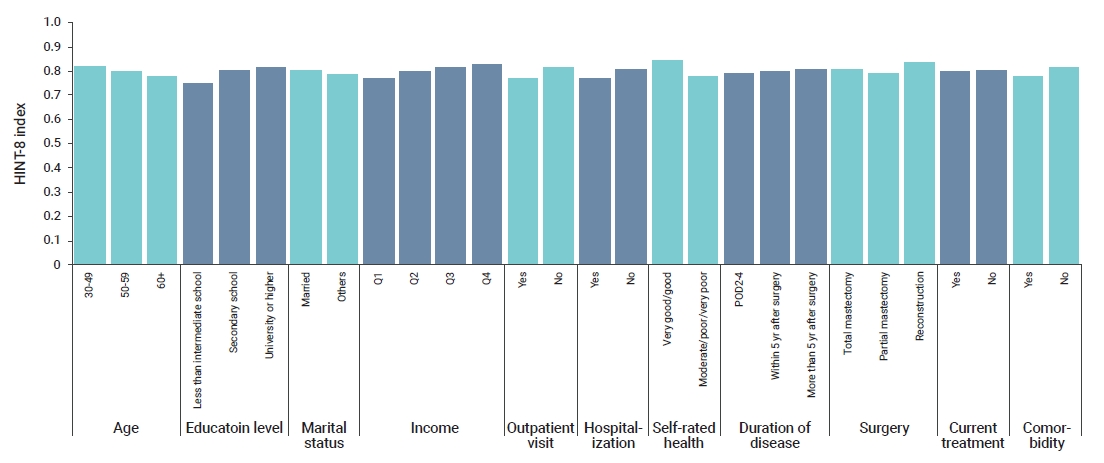
Table 1.General and clinical characteristics
|
Characteristic |
Baseline (n=300) |
Follow-up (n=100) |
|
Age (y) |
54.4±9.1 |
54.4±8.6 |
|
30–49 |
93 (31.0) |
28 (28.0) |
|
50–59 |
119 (39.7) |
42 (42.0) |
|
≥60 |
88 (29.3) |
30 (30.0) |
|
Level of education |
|
|
|
Less than intermediate school |
46 (15.3) |
19 (19.0) |
|
Secondary school |
116 (38.7) |
45 (45.0) |
|
University degree or higher |
138 (46.0) |
36 (36.0) |
|
Marital status |
|
|
|
Married |
239 (79.7) |
79 (79.0) |
|
Others |
61 (20.3) |
21 (21.0) |
|
Monthly household income (₩10,000) |
508±516 |
492±557 |
|
Q1 (n=85) |
124±64 |
115±66 |
|
Q2 (n=75) |
327±65 |
312±56 |
|
Q3 (n=72) |
555±60 |
519±65 |
|
Q4 (n=68) |
1,136±740 |
1,091±891 |
|
Outpatient visit in the past 2 weeks |
|
|
|
Yes |
92 (30.7) |
35 (35.0) |
|
No |
208 (69.3) |
65 (65.0) |
|
Hospitalization in the past 1 year |
|
|
|
Yes |
71 (23.7) |
22 (22.0) |
|
No |
229 (76.3) |
78 (78.0) |
|
Self-rated health |
|
|
|
Very good/good |
100 (33.3) |
33 (33.0) |
|
Moderate/poor/very poor |
200 (66.7) |
67 (67.0) |
|
Postoperative duration |
4.2±4.0 |
4.8±3.7 |
|
2–5 day (n=50) |
50 (16.7) |
0 |
|
<5 y (n=150) |
150 (50.0) |
60 (60.0) |
|
≥5 y (n=100) |
100 (33.3) |
40 (40.0) |
|
Surgery |
|
|
|
Total mastectomy |
60 (20.0) |
17 (17.0) |
|
Partial mastectomy |
209 (69.7) |
72 (72.0) |
|
Reconstruction |
31 (10.3) |
11 (11.0) |
|
Current treatment |
|
|
|
Yes |
139 (46.3) |
49 (49.0) |
|
No |
161 (53.7) |
51 (51.0) |
|
Comorbidity |
|
|
|
Yes |
110 (36.7) |
41 (41.0) |
|
No |
190 (63.3) |
59 (59.0) |
Table 2.Comparison of the EQ-5D-5L index, the EQ VAS, and the FACT-B total score according to the presence of problems in the HINT-8
|
HINT-8 item |
Levela)
|
n
|
EQ-5D-5L index |
EQ VAS |
FACT-B total |
|
Climbing stairs |
1 |
162 |
0.878±0.094**
|
82.29±12.74**
|
27.71±5.00**
|
|
2 or 3 or 4 |
138 |
0.794±0.130 |
74.86±17.49 |
23.30±6.29 |
|
Pain |
1 |
104 |
0.901±0.098**
|
84.01±11.04**
|
28.14±4.86**
|
|
2 or 3 or 4 |
196 |
0.807±0.117 |
76.14±16.86 |
24.38±6.20 |
|
Vitality |
1 |
78 |
0.891±0.114**
|
84.68±13.05**
|
27.36±5.54*
|
|
2 or 3 or 4 |
222 |
0.821±0.116 |
76.83±15.85 |
25.09±6.10 |
|
Working |
1 |
121 |
0.891±0.088**
|
83.84±11.59**
|
27.97±4.87**
|
|
2 or 3 or 4 |
179 |
0.805±0.125 |
75.51±16.93 |
24.14±6.26 |
|
Depression |
1 |
117 |
0.899±0.094**
|
85.12±11.08**
|
28.02±4.90**
|
|
2 or 3 or 4 |
183 |
0.802±0.119 |
74.87±16.65 |
24.19±6.23 |
|
Memory |
1 |
81 |
0.887±0.097**
|
83.28±12.60**
|
27.70±4.74**
|
|
2 or 3 or 4 |
219 |
0.822±0.122 |
77.24±16.21 |
24.94±6.30 |
|
Sleep |
1 |
101 |
0.877±0.098**
|
83.55±10.95**
|
26.94±5.36*
|
|
2 or 3 or 4 |
199 |
0.821±0.125 |
76.49±16.94 |
25.05±6.27 |
|
Happiness |
1 |
60 |
0.899±0.105**
|
88.18±9.10**
|
27.83±5.26*
|
|
2 or 3 or 4 |
240 |
0.825±0.118 |
76.54±15.95 |
25.15±6.11 |
Table 3.Correlation coefficients between the HINT-8 and the EQ-5D-5L
|
HINT-8 |
Mobility |
Self-care |
Usual activities |
Pain/discomfort |
Anxiety/depression |
EQ-5D-5L index |
EQ VAS |
|
Climbing stairs |
0.493**
|
0.165*
|
0.321**
|
0.365**
|
0.241**
|
–0.440**
|
–0.227**
|
|
Pain |
0.407**
|
0.135*
|
0.373**
|
0.600**
|
0.290**
|
–0.553**
|
–0.310**
|
|
Vitality |
0.311**
|
0.104 |
0.249**
|
0.290**
|
0.331**
|
–0.377**
|
–0.373**
|
|
Working |
0.454**
|
0.108 |
0.419**
|
0.429**
|
0.338**
|
–0.505**
|
–0.338**
|
|
Depression |
0.264**
|
0.162*
|
0.255**
|
0.224**
|
0.727**
|
–0.453**
|
–0.378**
|
|
Memory |
0.206**
|
0.035 |
0.166*
|
0.318**
|
0.198**
|
–0.303**
|
–0.191**
|
|
Sleep |
0.182*
|
0.175*
|
0.257**
|
0.263**
|
0.301**
|
–0.307**
|
–0.283**
|
|
Happiness |
0.246**
|
0.071 |
0.229**
|
0.243**
|
0.511**
|
–0.376**
|
–0.461**
|
|
HINT-8 index |
–0.473**
|
–0.158**
|
–0.435**
|
–0.581**
|
–0.561**
|
0.671**
|
0.577**
|
Table 4.Correlation coefficients between the HINT-8 and the FACT-B
|
HINT-8 |
PWB |
SWB |
EWB |
FWB |
BCS |
TOI |
FACT-G total |
FACT-B total |
|
Climbing stairs |
–0.367**
|
–0.148*
|
–0.207**
|
–0.287**
|
–0.374**
|
–0.402**
|
–0.303**
|
–0.347**
|
|
Pain |
–0.582**
|
–0.202**
|
–0.253**
|
–0.375**
|
–0.368**
|
–0.501**
|
–0.413**
|
–0.439**
|
|
Vitality |
–0.469**
|
–0.211**
|
–0.330**
|
–0.358**
|
–0.230**
|
–0.407**
|
–0.406**
|
–0.397**
|
|
Working |
–0.566**
|
–0.219**
|
–0.272**
|
–0.414**
|
–0.357**
|
–0.519**
|
–0.431**
|
–0.456**
|
|
Depression |
–0.387**
|
–0.300**
|
–0.589**
|
–0.477**
|
–0.379**
|
–0.506**
|
–0.524**
|
–0.532**
|
|
Memory |
–0.301**
|
–0.213**
|
–0.143*
|
–0.240**
|
–0.237**
|
–0.295**
|
–0.271**
|
–0.290**
|
|
Sleep |
–0.351**
|
–0.114*
|
–0.211**
|
–0.439**
|
–0.244**
|
–0.424**
|
–0.322**
|
–0.336**
|
|
Happiness |
–0.357**
|
–0.445**
|
–0.474**
|
–0.545**
|
–0.350**
|
–0.512**
|
–0.570**
|
–0.566**
|
|
HINT-8 index |
0.714**
|
0.390**
|
0.535**
|
0.621**
|
0.568**
|
0.767**
|
0.698**
|
0.731**
|
Table 5.Test-retest reliability of the HINT-8
|
HINT-8 |
Kappa (95% CI) |
Weighted kappa (95% CI) |
Agreement rate (%) |
|
Climbing stairs |
0.396 (0.235–0.557) |
0.469 (0.316–0.622) |
66 |
|
Pain |
0.428 (0.273–0.584) |
0.467 (0.320–0.615) |
68 |
|
Vitality |
0.134 (–0.010–0.277) |
0.249 (0.112–0.386) |
43 |
|
Working |
0.428 (0.280–0.577) |
0.440 (0.304–0.575) |
67 |
|
Depression |
0.436 (0.281–0.591) |
0.513 (0.374–0.652) |
68 |
|
Memory |
0.416 (0.238–0.593) |
0.464 (0.293–0.635) |
70 |
|
Sleep |
0.418 (0.257–0.579) |
0.499 (0.355–0.644) |
66 |
|
Happiness |
0.390 (0.241–0.539) |
0.444 (0.294–0.593) |
60 |
|
HINT-8 index |
0.690 (0.580–0.780)a)
|
- |
- |
References
- 1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209−49.ArticlePubMed
- 2. Jung KW, Won YJ, Kong HJ, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2016. Cancer Res Treat 2019;51:417−30.ArticlePubMedPMC
- 3. Park SK. Epidemiological characteristics of breast cancer in Koreans. J Korean Med Assoc 2019;62:424−36.Article
- 4. Wells GA, Russell AS, Haraoui B, et al. Validity of quality of life measurement tools: from generic to disease-specific. J Rheumatol Suppl 2011;88:2−6.ArticlePubMed
- 5. Kim SH, Jo MW, Lee JW, et al. Validity and reliability of EQ-5D-3L for breast cancer patients in Korea. Health Qual Life Outcomes 2015;13:203. ArticlePubMedPMC
- 6. Jensen R, Moinpour C, Fairclough D. Assessing health-related quality of life in cancer trials. Clin Investig 2012;2:563−77.Article
- 7. Ock M, Jo MW, Lee S. Measuring health related quality of life using EQ-5D in South Korea. J Health Tech Assess 2013;1:103−11.
- 8. Jo MW. Development of measurement tool for health related quality of life in the Korean National Health and Nutrition Examiniation Survey. Cheongju: Korea Centers for Disease Control and Prevention; 2014.
- 9. Lee HJ, Jo MW, Choi SH, et al. Development and psychometric evaluation of measurement instrument for Korean health-related quality of life. Public Health Wkly Rep 2016;9:447−54.
- 10. Jo MW. Valuation of Korean Health-Related Quality of Life Instrument with 8 Items (HINT-8). Cheongju: Korea Centers for Disease Control and Prevention; 2017. Korean.
- 11. Zhang J, Miller CJ, O'Malley V, et al. Patient quality of life fluctuates before and after Mohs micrographic surgery: a longitudinal assessment of the patient experience. J Am Acad Dermatol 2018;78:1060−7.ArticlePubMed
- 12. Park KY, Kim M, Yang YO. Factors relating to quality of life in Korean breast cancer patients: systematic review and meta-analysis. J Korean Acad Fundam Nurs 2017;24:95−105.Article
- 13. Yoo HJ, Ahn SH, Eremenco S, et al. Korean translation and validation of the functional assessment of cancer therapy-breast (FACT-B) scale version 4. Qual Life Res 2005;14:1627−32.ArticlePubMed
- 14. EuroQol Research Foundation. EQ-5D-5L user guide, 2019 [Internet]. Rotterdam: EuroQol Research Foundation; 2019 [cited 2020 Jun 12]. Available from: https://euroqol.org/publications/user-guides.
- 15. Kim SH, Ahn J, Ock M, et al. The EQ-5D-5L valuation study in Korea. Qual Life Res 2016;25:1845−52.ArticlePubMed
- 16. Kim SH, Jo MW, Ahn J, et al. The valuation of EQ-5D-5L health states in Korea. Seoul: National Evidence-based Healthcare Collaborating Agency; 2014.
- 17. FACIT.org. Questionnaires 2020 [Internet]. FACIT.org; 2020 [cited 2021 July 30]. Available from: https://wizard.facit.org/index.php?option=com_facit&view=search&layout=measure&id=5.
- 18. Jo MW, Lee HJ, Kim SY, et al. Development and validation of a novel generic Health-related Quality of Life Instrument with 20 Items (HINT-20). J Prev Med Public Health 2017;50:38−59.ArticlePubMedPMC
- 19. Fayers PM, Machin D. Quality of life: the assessment, analysis and reporting of patient-reported outcomes. 3rd ed. Wiley Blackwell; 2015.
- 20. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 2016;15:155−63.ArticlePubMedPMC
- 21. Chae YR, Seo K. Health-related quality of life in women with breast cancer in Korea: do sociodemographic characteristics and time since diagnosis make a difference? Oncol Nurs Forum 2010;37:E295−303.ArticlePubMed
- 22. Yan B, Yang LM, Hao LP, et al. Determinants of quality of life for breast cancer patients in Shanghai, China. PLoS One 2016;11:e0153714.ArticlePubMedPMC
- 23. Lu W, Cui Y, Chen X, et al. Changes in quality of life among breast cancer patients three years post-diagnosis. Breast Cancer Res Treat 2009;114:357−69.ArticlePubMed
- 24. Chen Q, Li S, Wang M, et al. Health-related quality of life among women breast cancer patients in eastern China. Biomed Res Int 2018;2018:1452635. ArticlePubMedPMC
- 25. Kang M. Quality of life of breast cancer patients measured by EQ-5D-5L [dissertation] Seoul, Seoul National University. 2017.
- 26. Jo HC, Kim ET, Min JW. Distress and quality of life for breast cancer survivors during follow-up periods in Korea. J Breast Dis 2016;4:58−63.Article
- 27. Lee CF, Ng R, Luo N, et al. The English and Chinese versions of the five-level EuroQoL Group's five-dimension questionnaire (EQ-5D) were valid and reliable and provided comparable scores in Asian breast cancer patients. Support Care Cancer 2013;21:201−9.ArticlePubMed
- 28. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;33:159−74.ArticlePubMed
- 29. Sim J, Wright CC. The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Phys Ther 2005;85:257−68.ArticlePubMed
- 30. Koh D, Abdullah AM, Wang P, et al. Validation of Brunei's Malay EQ-5D questionnaire in patients with type 2 diabetes. PLoS One 2016;11:e0165555.ArticlePubMedPMC
- 31. Chatterji R, Naylor JM, Harris IA, et al. An equivalence study: are patient-completed and telephone interview equivalent modes of administration for the EuroQol survey? Health Qual Life Outcomes 2017;15:18. ArticlePubMedPMC
Citations
Citations to this article as recorded by

- Health-related quality of life of premenopausal young breast cancer survivors undergoing endocrine therapy
Kyungmi Lee, Hye Suk Jun
European Journal of Oncology Nursing.2024; 68: 102496. CrossRef - Smartphone application-based rehabilitation in patients with chronic respiratory and cardiovascular diseases
Chiwook Chung, Ah-Ram Kim, Dongbum Kim, Hee Kwon, Seong Ho Lee, Il-Young Jang, Min-Woo Jo, Do-Yoon Kang, Sei Won Lee
Scientific Reports.2024;[Epub] CrossRef - Willingness to pay for integrative healthcare services to treat sleep disturbances: Evidence from a nationwide survey
Min Kyung Hyun
European Journal of Integrative Medicine.2023; 58: 102223. CrossRef - Internal Structure of the Health-Related Quality of Life Instrument with 8-Items in a Nationally Representative Population
Eun-Hyun Lee
Journal of Korean Academy of Nursing.2023; 53(3): 359. CrossRef - Factors influencing health-related quality of life for young single-person households: the mediating effect of resilience
Soo Jin Lee, Sujin Lee, Xianglan Jin
Journal of Korean Biological Nursing Science.2023; 25(3): 160. CrossRef - Smartphone application-based rehabilitation in patients with chronic respiratory and cardiovascular diseases: a randomised controlled trial study protocol
Chiwook Chung, Ah-Ram Kim, Il-Young Jang, Min-Woo Jo, Seongho Lee, Dongbum Kim, Hee Kwon, Do-Yoon Kang, Sei Won Lee
BMJ Open.2023; 13(9): e072698. CrossRef - Health-related quality of life among cancer patients and survivors and its relationship with current employment status
Woorim Kim, Kyu-Tae Han, Seungju Kim
Supportive Care in Cancer.2022; 30(5): 4547. CrossRef - Associations between Food Groups and Health-Related Quality of Life in Korean Adults
Shamirah Nabbosa, Sunghee Lee
Nutrients.2022; 14(17): 3643. CrossRef - Validity of the Health-Related Quality of Life Instrument with 8 Items (HINT-8) in the Korean Elderly: A Cross-Sectional Study
Seon-Ha Kim, Miok Kim
Journal of Korean Gerontological Nursing.2022; 24(3): 248. CrossRef

 , Min-Woo Jo1,2
, Min-Woo Jo1,2
 PubReader
PubReader ePub Link
ePub Link Cite
Cite