
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 5(6); 2014 > Article
-
Original Article
Optimal Implementation of Intervention to Control the Self-harm Epidemic - Byul Nim Kim, M.A. Masud, Yongkuk Kim
-
Osong Public Health and Research Perspectives 2014;5(6):315-323.
DOI: https://doi.org/10.1016/j.phrp.2014.10.001
Published online: November 12, 2014
Department of Mathematics, Kyungpook National University, Daegu, Korea
- ∗Corresponding author. yongkuk@knu.ac.kr
• Received: August 3, 2014 • Revised: September 15, 2014 • Accepted: September 22, 2014
© 2014 Published by Elsevier B.V. on behalf of Korea Centers for Disease Control and Prevention.
This is an Open Access article distributed under the terms of the CC-BY-NC License (http://creativecommons.org/licenses/by-nc/3.0).
Abstract
-
Objectives
- Deliberate self-harm (DSH) of a young person has been a matter of growing concern to parents and policymakers. Prevention and early eradication are the main interventional techniques among which prevention through reducing peer pressure has a major role in reducing the DSH epidemic. Our aim is to develop an optimal control strategy for minimizing the DSH epidemic and to assess the efficacy of the controls.
-
Methods
- We considered a deterministic compartmental model of the DSH epidemic and two interventional techniques as the control measures. Pontryagin's Maximum Principle was used to mathematically derive the optimal controls. We also simulated the model using the forward-backward sweep method.
-
Results
- Simulation results showed that the controls needed to be used simultaneously to reduce DSH successfully. An optimal control strategy should be adopted, depending on implementation costs for the controls.
-
Conclusion
- The long-term success of the optimum control depends on the implementation cost. If the cost is very high, the control could be used for a short term, even though it fails in the long run. The control strategy, most importantly, should be implemented as early as possible to attack a comparatively fewer number of addicted individuals.
- Deliberate self-harm (DSH) is an activity of an individual in which the sole intention is to cause self-harm, although not to commit suicide; however, sometimes acute medical situations arise [1]. More scientific definitions of DSH are available in the literature [2–4]. It is associated with the physiology and psychology of the affected individual. In the past decade, it has become a pronounced health concern among adolescents and young adults all over the world [5]. You et al [6] and Whitlock [7] addressed it as a contagious social issue. Deliberate self-harm is associated with depression, anxiety, poor school performance, family conflict [8], sexual abuse [9], and other factors. Mathematical modeling of epidemics is a constructive tool to assess the evolution of contagious problems and to discover strategies to reduce or eradicate the epidemic of contagious problems.
- The techniques of mathematical modeling have recently been utilized in problems related to human behaviors and social interaction. For example, the theory for social behavior of individuals subjected to the social interaction was developed by Wirl and Feichtinger [10] to address the problem of obesity. Mathematical models have also been used to study the obesity epidemic [11–16]. Such ideas are also used to study smoking dynamics mathematically [17–22]. In addition, Li [23] used Bayesian proportional hazard analysis to deal with school drop-out. Porco et al [24] presented two models for antibiotic abuse. The techniques of mathematical modeling are likewise being exercised to understand contagious social and behavioral epidemics from diverse viewpoints.
- Do and Lee [25] proposed a mathematical model for the self-harm epidemic and analyzed it mathematically. By considering self-harm as a contagious disease, they formulated a deterministic compartmental model. In the present study, we introduced time-dependent controls into the Do and Lee model [25], and extend an optimal control problem to understand cost-effective strategies for reducing DSH.
Introduction
- 2.1 Basic model
- The Lee and Do model [25] without a demographic effect reduces to the following formula:
- In this paper, we note that the whole population N(t) = S(t)+A(t)+P(t)+R(t) is constant. The variable N(t) includes only adolescents and young adults between the ages 12 years and 23 years and is divided into four classes: susceptible, S(t); addicted, A(t); in treatment P(t); and recovered, R(t). Individuals of S(t) who try DSH move to A(t) with the per capita transition rate, α, which is peer pressure on susceptible individuals in A(t) and P(t). Individuals repeating DSH remain in A(t), but individuals who stop DSH move to R(t) at the rate η. This is the rate at which individuals in A(t) stop DSH without any treatment program or individuals who tried DSH only once and transferred to R(t). When individuals in A(t) seek treatment, they go to P(t) at the rate of β(P+R)/N+θ. In this equation, β is peer pressure due to individuals in P(t) and R(t) to the individuals in A(t), and θ is the intervention rate at which addicted individuals seek treatment. If the treatment fails, individuals may go back to A(t) from P(t) at the rate ω. Individuals in P(t) recover at rate ρ and move to R(t). The values of α and β may be different, but in this study they are considered the same for homogeneous mixing. Among all of these parameters, the system is most sensitive to α and η [19]. The values of η may also increase or decrease, depending on the positive or negative influence of the Internet [26]. Furthermore, the individual who performs DSH once, seeks more serious injury for the next DSH episode [27]. Therefore, a control strategy should be concerned with prevention through controlling peer pressure α and early intervention η.
- 2.2 Optimal control
- To shrink the DSH epidemic, we adopted two control strategies with the intent of increasing prevention [i.e., decreasing α and increasing early intervention (η)]. However, maintaining constant control over time is impractical. Therefore, our aim is to show that it is possible to implement time-dependent control techniques while minimizing the addicted population with minimum cost of implementation of the control measures.
- To develop an optimal control problem for the aforementioned purpose, two control terms were introduced into the basic model (1). The model reduces to the following formula:
- In this equation N = S(t)+A(t)+P(t)+R(t) is constant.
- The control variables, u1(t) and u2(t), represent the quantity of intervention associated with the parameters α and η, respectively at time t. The factor of 1−u1(t) reduces the per capita transition rate α from S(t) to A(t). The per capita transition rate η from P to R increases at a rate that is proportional to u2(t) in which μ > 0 is the proportionality constant.
- We define our control set as follows:
- An optimal control problem with the objective cost functional can be given bywhich is subject to the state equation (2). In the objective cost functional, the quantities Ac, B1 and B2 represent the weight constants. The costs associated with the controls of the transition rates are described by the terms
- Therefore,
- Let S∗(t), A∗(t), P∗(t), R∗(t) be optimal state solutions with associated optimal control variables
- Furthermore, the optimal controls
- (Please refer to Appendix 1 for the formulation in detail.)
Materials and methods
- To find the optimal control strategy for controlling the self-harm epidemic of adolescents and young adults in institutional settings, an optimal control problem has been established, based on the model proposed by Do and Lee [25]. The optimal control problem consists of eight ordinary differential equations describing states and adjoint variables with two control variables. The state variables are “susceptible”, S; “addicted”, A; “in treatment”, P; and “recovered”, R; the control u1 is associated with reducing peer pressure and the control u2 is associated with early intervention. As a general shortcoming, full efficiency of the controls is unfeasible. To choose an upper bound for the controls, we considered the study of Dunlop et al [29] in which they found that 79% of young people learned about suicide from the newspaper or from friends and family, and 59% of them learned from an online source. We assumed the upper bound of each of the controls was 0.6. The rate constant μ is chosen to be 0.01 in accordance with the value of η. Using the parameter values summarized in Table 1, the problem is solved numerically by the forward-backward sweep method [30], along with the fourth order Runge-Kutta algorithm, which is subject to a wide range of plausible values of weight factors Ac, B1 and B2 because the weights should vary from group to group. For an institutional setting, we considered that the total population is N(0) = 10000 with S(0) = 8700, A(0) = 900, P(0) = 100, R(0) = 300. Time span for the simulation is [0, T], in which T = 60 months (i.e., 5 years).
- Figure 1 depicts the dynamics of states with and without the controls when the weight factors are Ac = 1, B1 = 500, B2 = 500. The rightmost graphs in Figure 1 show the time-dependent control strategy in which we see that the controls u1 and u2 should be implemented at maximum for a long period and then gradually decreased to zero. The controls work fairly well for reducing the number of addicted population.
- Let t1 and t2 be the period of time for maximum implementation of the optimal controls u1 and u2, respectively. The time t1 and t2 may depend on the weights Ac, B1, B2 and the initial conditions as well. Figure 2 depicts the changes of t1 and t2 with B1 = 100–1000 and Ac = 1–100 while keeping B2 = 200 fixed. Figure 2A shows that for Ac > 60, the time t1 is the same for all B1; however, for smaller Ac; the effect of B1 to the change of t1 is more pronounced. A smaller B1 results in a higher t1 and vice versa. Figure 2B shows that t2 increases with Ac but it is not affected by B1. Figure 3 depicts the changes of t1 and t2 with B2 = 100–1000 and Ac = 1–100 while keeping B1 = 200 fixed. The change of weight B2 does not affect the change of t1 for all Ac and also does not affect the change of t2 for Ac > 40. Figure 4 depicts the changes of t1 and t2 with B1 = 100–1000 and B2 = 100–1000 while keeping Ac = 1 fixed. Figure 4A illustrates that changes in B1 and B2 negatively affect changes in t1 and t2, as we have already seen in Figures 2 and 3. In addition, for B1 > 100 t1 increases with B2. However, B1 has no noticeable effect in the change of t2. Figure 5 depicts the changes of t1 and t2 with B1 = 100–1000 and B2 = 100–1000 while keeping Ac = 10 fixed. In this case, B1, and B2 have no effect on changes in t2 and t1, respectively.
- The optimal control aims at reducing the number of addicted individuals while ensuring the least implementation cost of the two controls mentioned previously. Let
Results
- An optimal control problem has been established that takes into consideration self-harm as a contagious disease. We considered two control strategies: (1) reducing peer pressure and (2) accelerating early intervention with their associated costs (i.e., B1 and B2, respectively). The control problem is solved using Pontryagin's Maximum Principle. In this circumstance, the negative effect of an addicted individual is parameterized by Ac. The simultaneous use of both controls reduces the self-harm epidemic by increasing susceptible individuals and reducing the addicted individuals remarkably. But the costs associated with control strategies and the weight Ac may not be the same in all groups of young people. Depending on the groups, the costs and the weight may be varied so that different control strategies are needed. For a higher weight of addicted individuals, we used nearly the same control strategy for the groups, even with different control costs, which agrees with our intuition that a greater weight requires greater effort from the controls, irrespective of the control cost. However, if the weight is low, a great effort by the controls is no longer necessary. As a result, the strategy varies from group to group, depending on the control costs associated with the groups. Controls are implemented in smaller numbers in groups with a high control cost and vice versa.
- In the case of low weight, the strategy for early intervention is not affected by the cost associated with reducing peer pressure. However, if the cost of reducing peer pressure is high in some groups, it affects the reduction of peer pressure. As a result, the number of addicted individuals increase, which requires more effort for early intervention, even though it is expensive. Furthermore, the control strategies have no interdependency, resulting from the associated costs.
- The simulations presented above also shows that the control strategy is affected by the initial condition and the control costs. In groups with a high control cost, the control strategy is unsuitable for the long run. If the initial number of addicted people in a population is high, the control fails for lower costs of the controls. Therefore, even if the control costs are high, early implementation gives better results rather than waiting and allowing the number of addicted individuals to increase.
- Therefore, we conclude that the simultaneous use of the controls gives the desired outcome. In groups in which associated costs are high, the controls may fail after a long period. What is most important is that the control strategy should be implemented as early as possible to attack a comparatively fewer number of addicted individuals. To make the model more realistic, further efforts should be focused on including age-dependent peer pressure [31], which remains for our future work.
Discussion
- The authors declare no conflicts of interest.
Conflicts of interest
Theorem 1
Proof
-
Acknowledgements
- This work was supported by Kyungpook National University Research Fund, (Daegu, Korea), 2012.
Acknowledgements
-
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article information
- 1. NHS Centre for Reviews and Dissemination . no. 6. Effective health care bulletin: deliberate self-harm. vol. 4:1998. University of York; York, United Kingdom.
- 2. Favazza A.. Why patients mutilate themselves. Hosp Community Psychiatry 40(2). 1989 Feb;137−145. PMID: 2644160.ArticlePubMed
- 3. Madge N., Hewitt A., Hawton K.. Deliberate self-harm within an international community sample of young people: comparative findings from the Child and Adolescent Self-harm in Europe (CASE) Study. J Child Psychol Psychiatry 49(6). 2008 Jun;667−677. PMID: 18341543.ArticlePubMed
- 4. Mangnall J., Yurkovich E.. A literature review of deliberate self-harm. Perspect Psychiatr Care 44(3). 2008 Jul;175−184. PMID: 18577123.ArticlePubMed
- 5. Skegg K.. Self-harm. Lancet 366:2005 Oct;1471−1483. PMID: 16243093.ArticlePubMed
- 6. You J., Lin M.P., Fu K.. The best friend and friendship group influence on adolescent nonsuicidal self-injury. J Abnorm Child Psychol 41(6). 2013 Aug;993−1004. PMID: 23474798.ArticlePubMed
- 7. Whitlock J.. Self-Injurious behavior in adolescents. PLoS Medicine 7(5). 2010 May;e1000240PMID: 20520850.ArticlePubMed
- 8. Laukkanen E., Rissanen M.-L., Honkalampi K.. The prevalence of self-cutting and other self-harm among 13- to 18-year-old Finnish adolescents. Soc Psychiatry Psychiatr Epidemiol 44(1). 2009 Jan;23−28. PMID: 18604615.ArticlePubMed
- 9. Romans S.E., Martin J.L., Anderson J.C.. Sexual abuse in childhood and deliberate self-harm. Am J Psychiatry 152(9). 1995 Sep;1336−1342. PMID: 7653690.ArticlePubMed
- 10. Wirl F., Feichtinger G.. Modelling social dynamics (of obesity) and thresholds. Games 1(4). 2010 Jul;395−414.Article
- 11. González-Parra G., Acedo L., Villanueva Micó R.-J., Arenas A.J.. Modeling the social obesity epidemic with stochastic networks. Physica A 389(17). 2010 Sep;3692−3701.Article
- 12. Jódar L., Santonja F.J., González-Parra G.. Modeling dynamics of infant obesity in the region of Valencia, Spain. Comput Math Appl 56(3). 2008 Aug;679−689.Article
- 13. Kim M.S., Chu C., Kim Y.. A Note on obesity as epidemic in Korea. Osong Public Health Res Perspect 2(2). 2011 Sep;135−140. PMID: 24159463.ArticlePubMed
- 14. Santonja F.J., Villanueva R.J., Jódar L.. Mathematical modeling of social obesity epidemic in the region of Valencia, Spain. Mathematical and Computer Modeling of Dynamical Systems: Methods. Tools and Applications in Engineering and Related Sciences 16(1). 2010 Feb;23−34.
- 15. Santonja F.J., Shaikhet L.. Probabilistic stability analysis of social obesity epidemic by a delayed stochastic model. Nonlinear Analysis: Real World Applications 17:2014 Jun;114−125.Article
- 16. Aldila D., Rarasati N., Nuraini N.. Optimal control problem of treatment for obesity in a closed population. Int J Math Math Sci 2014:2014;Article ID 273037. http://dx.doi.org/10.1155/2014/273037.Article
- 17. Castillo-Garsow C., Jordan-Salivia G., Herrera A.R.. Mathematical models for the dynamics of tobacco use, recovery, and relapse. Technical Report Series BU-1505-M. 1997. Cornell University; Ithaca, NY.
- 18. Castillo G.C., Jordan S.G., Rodriguez A.H.. Mathematical models for the dynamics of tobacco use, recovery and relapse. Technical Report Series BU-1505-M. 2000. Cornell University Department of Biometrics; Ithaca, NY.
- 19. Sharomi O., Gumel A.B.. Curtailing smoking dynamics: a mathematical modeling approach. Appl Math Comput 195(2). 2008 Feb;475−499.Article
- 20. Lahrouz A., Omari L., Kiouach D.. Deterministic and stochastic stability of a mathematical model of smoking. Stat Probab Lett 81(8). 2011 Aug;1276−1284.Article
- 21. Alkhudhari Z., Al-Sheikh S., Al-Tuwairqi S.. Global dynamics of a mathematical model on smoking. ISRN Applied Mathematics 2014;Article ID 847075.Article
- 22. Timms K.P., Rivera D.E., Collins L.M.. Continuous-time system identification of a smoking cessation intervention. Int J Control 87(7). 2014 Feb;1423−1437. PMID: 25382865.ArticlePubMed
- 23. Li M.. Bayesian proportional hazard analysis of the timing of high school dropout decisions. Econom Rev 26(5). 2007 Aug;529−556.Article
- 24. Porco T.C., Gao D., Scott J.C.. When does overuse of antibiotics become a tragedy of the commons? PLoS One 7(12). 2012;e46505PMID: 23236344.ArticlePubMedPMC
- 25. Do T.S., Lee Y.S.. A modeling perspective of deliberate self-harm. Journal of KSIAM 14(4). 2010;275−284.
- 26. Daine K., Hawton K., Singaravelu V.. The power of the web: a systematic review of studies of the influence of the internet on self-harm and suicide in young people. PLoS One 8(10). 2013 Oct;e77555PMID: 24204868.ArticlePubMed
- 27. Evans J., Reeves B., Platt H.. Impulsiveness, serotonin genes and repetition of deliberate self-harm (DSH). Psychol Med 30(6). 2000 Nov;1327−1334. PMID: 11097073.ArticlePubMed
- 28. Agrachev A., Sachkov Y.. Control theory from the geometric viewpoint. 2004. Springer; Berlin, Germany.
- 29. Dunlop S.M., More E., Romer D.. Where do youth learn about suicides on the Internet, and what influence does this have on suicidal ideation? J Child Psychol Psychiatry 52(10). 2011 Oct;1073−1080. PMID: 21658185.ArticlePubMed
- 30. Lenhart S., Workman J.T.. Optimal control applied to biological models. 2007. United Kingdom: Chapman and Hall/CRC; London: 책.
- 31. Moran P., Coffey C., Romaniuk H.. The natural history of self-harm from adolescence to young adulthood: a population-based cohort study. Lancet 379(9812). 2012 Jan;236−243. PMID: 22100201.ArticlePubMed
References
Figure 1The dynamics of states with and without controls when the weight factors are Ac = 1, B1 = 500, B2 = 500.
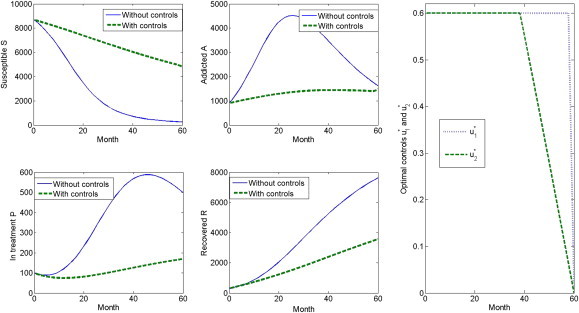
Figure 2(A) The duration of maximum implementation for the optimal control u_1. In this equation, Ac = 1–100, B1 = 100–1000, and B2 = 200. (B) The duration of maximum implementation for the optimal control u_2. In this equation, Ac = 1–100, B1 = 100–1000, and B2 = 200.
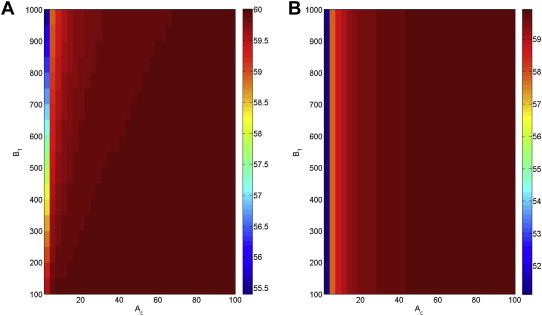
Figure 3(A). The duration of maximum implementation for the optimal control U1. In this equation, Ac = 1–100, B2 = 100–1000, and B1 = 200. (B). The duration of maximum implementation for the optimal control U2. In this equation, Ac = 1–100, B2 = 100–1000, and B1 = 200.
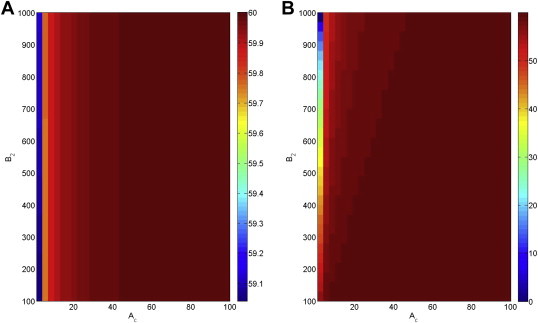
Figure 4(A). The duration of maximum implementation for the optimal control U1. In this equation, Ac = 1, B1 = 100–1000, and B2 = 100–1000. (B). The duration of maximum implementation for the optimal control U2. In this equation, Ac = 1, B1 = 100–1000, and B2 = 100–1000.
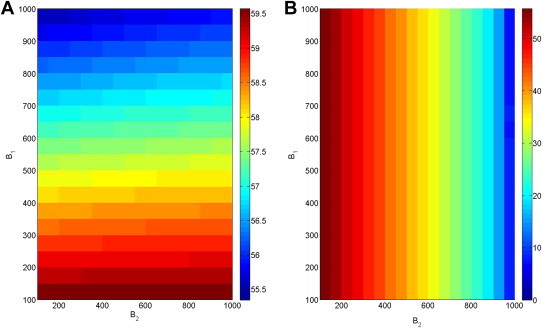
Figure 5(A). The duration of the maximum implementation for the optimal control u1. In this equation, Ac = 10, B1 = 100–1000, and B2 = 100–1000. (B). The duration of the maximum implementation for the optimal control u2. In this equation, Ac = 10, B1 = 100–1000, and B2 = 100–1000.
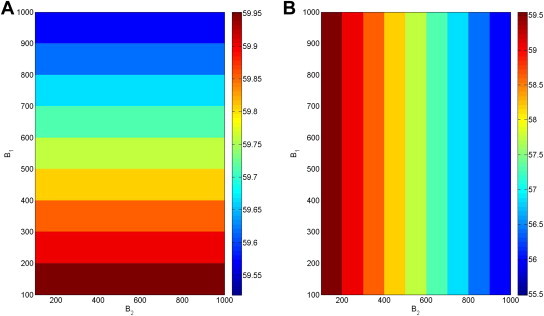
Figure 6(A) The contour plot of Δ A B 1 , B 2 T Δ A B 1 , B 2 T
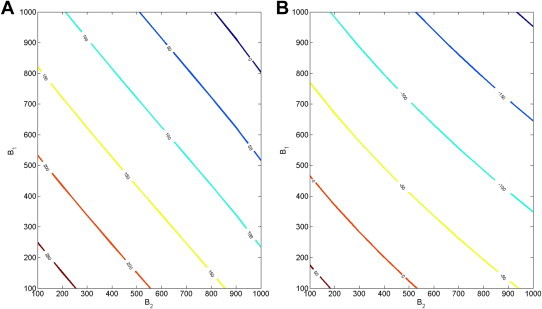
Table 1The parameter values for the model.
| Parameters | α | ω | β | θ | η | ρ | μ |
|---|---|---|---|---|---|---|---|
| Value (per mo.) | 0.17 | 0.018 | 0.024 | 0.0042 | 0.03 | 0.08 | 0.01 |
∗All values of the parameters are adopted from the results of parameter estimation in [25].
Figure & Data
References
Citations
Citations to this article as recorded by 
- A review of the use of optimal control in social models
D. M. G. Comissiong, J. Sooknanan
International Journal of Dynamics and Control.2018; 6(4): 1841. CrossRef - Adolescent self‐harm and risk factors
Jixiang Zhang, Jianwei Song, Jing Wang
Asia-Pacific Psychiatry.2016; 8(4): 287. CrossRef - Optimal Intervention Strategies for the Spread of Obesity
Chunyoung Oh, Masud M A
Journal of Applied Mathematics.2015; 2015: 1. CrossRef
 PubReader
PubReader Cite
Cite





