
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 4(4); 2013 > Article
-
Original Article
Evaluation of the Effectiveness of Pandemic Influenza A(H1N1) 2009 Vaccine Based on an Outbreak Investigation During the 2010–2011 Season in Korean Military Camps - Kyo-Hyun Kima, Yoon Gu Choib, Hyun-Bae Yoonc, Jung-Woo Leed, Hyun-Wook Kimd, Chaeshin Chue, Young-Joon Parkf
-
Osong Public Health and Research Perspectives 2013;4(4):209-214.
DOI: https://doi.org/10.1016/j.phrp.2013.07.002
Published online: July 23, 2013
aThe Third Republic of Korea Army, Ministry of National Defense, Seoul, Korea
bThe 2nd Air Defense Artillery Brigade, Air Force, Ministry of National Defense, Seoul, Korea
cThe 26th Mechanized Infantry Division, Ministry of National Defense, Seoul, Korea
dThe 11th Regiment, 1st Infantry Division, Ministry of National Defense, Seoul, Korea
eDivision of Epidemic Intelligence Service, Korea Centers for Disease Control and Prevention, Osong, Korea
fDivision of Vaccine Preventable Disease Control and National Immunization Program, Korea Centers for Disease Control and Prevention, Osong, Korea
- ∗Corresponding author. pahmun@hanmail.net
© 2013 Published by Elsevier B.V. on behalf of Korea Centers for Disease Control and Prevention.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives
- In December 2010, there was an outbreak of acute febrile respiratory disease in many Korean military camps that were not geographically related. A laboratory analysis confirmed a number of these cases to be infected by the pandemic influenza A(H1N1) 2009 (H1N1pdm09) virus. Because mass vaccination against H1N1pdm09 was implemented at the infected military camps eleven months ago, the outbreak areas in which both vaccinated and nonvaccinated individuals were well mixed, gave us an opportunity to evaluate the effectiveness of H1N1pdm09 vaccine through a retrospective cohort study design.
-
Methods
- A self-administered questionnaire was distributed to the three military camps in which the outbreak occurred for case detection, determination of vaccination status, and characterization of other risk factors. The overall response rate was 86.8% (395/455). Case was defined as fever (≥38 °C) with cough or sore throat, influenza-like illness (ILI), and vaccination status verified by vaccination registry. Crude vaccine effectiveness (VE) was calculated as “1 − attack rate in vaccinated individuals/attack rate in nonvaccinated individuals”, and adjusted VE was calculated as “1 – odds ratio” using logistic regression adjusted for potential confounding factor. A number of ILI definitions were used to test the robustness of the result.
-
Results
- The attack rate of ILI was 12.8% in register-verified vaccinated individuals and 24.0% in nonvaccinated individuals. The crude VE was thus calculated to be 46.8% [95% confidence interval (CI): 14.5–66.9]. The adjusted VE rate was 46.8% (95% CI: –9.4 to 74.1). Various combinations of ILI symptoms also showed similar VE rates.
-
Conclusion
- We evaluated the effectiveness of H1N1pdm09 vaccine in the 2010–2011 season in an outbreak setting. Although the result was not sensitive to any analytical method used and ILI case definition, the magnitude of effectiveness was lower than estimated in the 2009–2010 season.
- In December 2010, there was an outbreak of acute febrile respiratory disease in several Korean military camps that were not geographically related. An initial outbreak assessment showed that in each camp there were more than 10 cases with fever over 38 °C and respiratory disease for a few days. A laboratory examination confirmed influenza A(H1N1)pdm09 infection in some cases, and therefore, the authorities declared the outbreak as sporadic.
- This outbreak provided an opportunity to evaluate the effectiveness of A(H1N1)pdm09 vaccine under the following conditions. First, the Korean military conducted a mass vaccination drive from January 2010 in order to protect its soldiers from H1N1pdm09 infection, and no seasonal influenza vaccination was administered except for new recruits and medical staff. Second, the medical history and vaccination history of the individuals was collected from medical records in the camps. Third, the cases lived in the same barrack, and therefore were considered to be exposed to the H1N1pdm09 virus, and were in a steady group with no huge external effect because they had restricted contacts with outside groups.
- This environment and the characteristics of military camps were enough to fulfill the basic condition required to evaluate the effect of vaccination during an outbreak [1,2]. Previous research evaluating the effectiveness of H1N1pdm09 vaccine were mainly laboratory studies [3–6] or large-scale cohort studies [7–11]. Although few studies have been reported based on outbreak cases, studies on evaluating the effectiveness of vaccine 1 year after vaccination for H1N1pdm09 are rare [12,13]. This study was conducted to complement previous studies on the vaccination effect of H1N1pdm09.
- Therefore, the authors aimed to evaluate the vaccination effect of H1N1pdm09 using a retrospective cohort study design on a sporadic outbreak case, based on the aforementioned conditions and potential implications.
Introduction
- 2.1 Situation
- The Korean military conducted a mass vaccination drive—Green Flu-S Plus vaccine that had antigen (3.25 μg) and MF-58 adjuvant—against H1N1pdm09 infection from January 2010 to March 2010. The immunogenicity of the vaccine was confirmed in a previous study [6]. Since then, with no additional vaccination of H1N1pdm09, half of the vaccinated soldiers were discharged at the end of their service term and an equal number of new recruits were placed at the camps with no history of vaccination against the virus. Each camp had recruited a number of susceptible individuals. The three camps were independent units with no geographical or administrative relation.
- 2.2 Patients
- The study patients were soldiers stationed at the three military camps as of December 1, 2010. The authors distributed self-administered questionnaires and reviewed the medical records of the soldiers to check their vaccination history. Informed consents were obtained from all the study participants. The questions included symptoms (fever, body temperature, cough, sore throat, running nose, chill, and muscle pain), vaccination history of seasonal influenza, vaccination history of H1N1pdm09, previous diagnosis of H1N1pdm09 infection, smoking, body mass index (BMI), frequency of hand washing, underlying diseases, and sociodemographic factors.
- 2.3 Definition of variables
- Case included those individuals who reported fever (≥38 °C) with cough or sore throat, or those who had been treated for the same symptoms in December 2010. This definition corresponded to influenza-like illness (ILI) defined by the Korea Centers for Disease Control and Prevention (KCDC). The H1N1pdm09 vaccination status was defined as follows: registry verified vaccination, self reported vaccination (non-verified), non vaccination.
- 2.4 Analysis
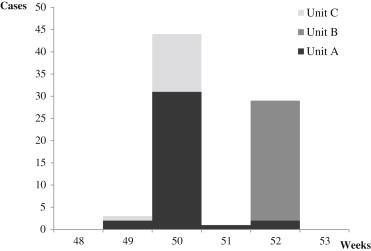
- The epidemic curve of each camp was recorded everyday (Figure 1), and the sociodemographic characteristics of each camp were tabulated (Table 1). Among the sociodemographic characteristics and influenza-associated factors, we identified the variables related to the vaccination history by Chi-square test. The associated variables were considered to be confounding factors in evaluating the effectiveness of vaccination. Vaccination effectiveness was evaluated by crude analysis, stratified analysis, and multivariate analysis. We evaluated the crude vaccine effectiveness (VE) by comparing the incidence based on the vaccination status with the following formula [1]:
- We then calculated the crude VE by stratifying the sociodemographic characteristics and influenza-associated factors. In the multivariate analysis, we included age, smoking status, BMI, seasonal influenza vaccinations status, and H1N1pdm09 vaccination status.
- Because we used the nonspecific clinical symptoms in the case definition, we estimated the vaccination effectiveness with various case definitions [e.g., cases with fever ≥37.8 °C or ≥38 °C in the medical record] and compared those with the VE of our case definition. This was conducted to evaluate the robustness of the results of this study, that is, a kind of sensitivity analysis.
- 2.5 Ethical considerations
- Although this study does not require an Institutional Review Board (IRB) consideration, as it was conducted as part of an epidemiological investigation of a respiratory outbreak in military camps, it contained a susceptible study group. Therefore, this study was reviewed by the Korean Military IRB. We distributed the study plan to all the study participants and received informed consents. To acknowledge their participation in the study, the participants were provided with a present.
Materials and Methods
- As of December 1, 2010, there were a total of 455 candidates in the three military camps, and among them, 395 participated in this study (participant rate: 86.8%). A total of 50 persons rejected participation and 10 were unable to attend the interview, because they were unavailable in their respective camps during the study.
- 3.1 Outbreak situation
- A total of 77 cases in three units were identified and the incidence rate was 19.5%. The incidence rate of Units A, B, and C was 14.6% (36/247), 29.0% (27/93), 25.5% (14/55), respectively. Each unit's incidence aspect is shown in Figure 1. Although the outbreak period was different, the progress of the outbreak was similar with a single peak.
- Approximately 85% of the study participants were ≤25 years, and all were men except one. The number of recruits admitted prior to January 1, 2010, who were supposed to have H1N1pdm09 vaccination in the camp, was 224 (56.7%). A total of 16 soldiers (4%) were treated for H1N1pdm09 infection prior to joining the military camp, and 27 (6.8%) had seasonal influenza vaccination in the past 1 year. The vaccination rate of H1N1pdm09 as verified by the registry was 37.7% (149/395). However, it will increase up to 69.3% (274/395) if the soldiers who checked the vaccination history in the questionnaires were also included (Table 1).
- 3.2 Effectiveness of influenza vaccine
- Crude VE was 45.9% [95% confidence interval (CI): 12.9–66.4], and the risk to get infected with ILI in the vaccinated group decreased by about half. If adjusted by age, smoking history, BMI, seasonal influenza vaccination history, H1N1pdm09 infection, the crude VE was 47.3% (95% CI: 4.1–71.0), and the risk to get ILI in the vaccinated group decreased similarly. A similar result (46.8%) was obtained if we exclude the unconfirmed H1N1pdm09 vaccination with no confirmation in the registry (Table 2). If various ILI definitions were applied, we had various incidence rates, but the values of vaccination effectiveness were relatively consistent. If loose case definition was applied (lowering the fever temperature or containing nonspecific symptoms only), the incidence rates were increasing, but the values of vaccination effectiveness were consistent. By contrast, if strict case definition was applied, the incidence rates decreased, but the vaccination effectiveness was not much different with that of the original setting (Table 3).
Results
- The H1N1pdm09 vaccine administered in January 2010 has about 50% effectiveness on the H1N1pdm09 outbreak that occurred in December 2010. The magnitude of vaccination effectiveness was robust with no huge difference, even when multivariate analysis was applied and various ILI definitions were adopted.
- The magnitude of VE in this study was lower than the 2009–2010 H1N1pdm09 season in the previous studies, which reported a 70% magnitude. However, the magnitude in this study was similar to that calculated for the next season (2010–2011) in the previous studies. Studies to evaluate the vaccination effectiveness 1 year after vaccination had suggested the hypothesis that the vaccination effectiveness was not persistent because no statistically significant results were available [12,13]. However, this study showed that statistically significant vaccination effectiveness does exist even 1 year after vaccination. The study result was immunologically consistent with a previous antigenicity study in which the vaccination effectiveness was noted even 1 year after seasonal influenza vaccination, but with decreased antibody titer [14].
- This study was designed and conducted to evaluate the vaccination effectiveness of H1N1pdm09 and methodologically makes up for the previous studies with case-control designs. In case-control study, exposure to a pathogen in the two groups is put artificially similar or is assumed to be similar. In this study, the study participants shared living space and contacted frequently, and therefore, we could assume that they were all similarly exposed to the pathogen regardless of vaccination status, which is the major explanatory variable. Using various combinations of case definition based on various body symptoms, respiratory symptoms, treatment status, and ILI confirmation status, the incidence rates of the vaccinated group were found to be lower than those of the nonvaccinated group. Although some CIs include the null value, no combination was statistically significant in the direction of effectiveness. This implied that the results of this study were not by chance, but were rather very robust. While interpreting the results of this study, the following should be considered. First, the case definition in this study was not that of a laboratory test but was a nonspecific one based on ILI symptoms, and so it could underestimate the vaccination effectiveness as in general studies with information misclassification [15,16]. However, the magnitude was considered minimum for the following reasons: First, a laboratory analysis confirmed all the cases to be H1N1pdm09 infected. Second, considering the aspect of outbreak, a single pathogen was suspected. Third, according to the KCDC influenza laboratory surveillance report, 95% of respiratory infection was due to H1N1pdm09 infection [17]. Fourth, the vaccination effectiveness under various case definitions was relatively consistent. Although the case definition was not based on the confirmative result of laboratory test, the aforementioned situations strongly suggested that the vaccination effectiveness in this study was not for ILI but for H1N1pdm09.
- Next, we needed to evaluate the intergroup heterogeneity (study participants, type of exposure, method to measure the result) in order to review the validity of pooled analysis. The study participants from the three groups were all men in their early 20s, shared camp lives, and were vaccinated with the same vaccine during the H1N1pdm09 mass vaccination drive. In addition, the aspect of outbreak was similar. The results were measured with the same questionnaire. Therefore, we thought that this study evaded any critical fault to suspect the results of pooled analysis.
- Finally, with regard to the external validity, the results of this study could not be applied to other age groups as well, especially to the elderly individuals who have low vaccination effectiveness. In this study, all the participants were young adult men. As for the internal validity, the study participants were homogeneous, a factor which enhanced the internal validity.
- Although there were some limitations, this study complemented the previous studies in study design and duration of effectiveness by evaluating the effectiveness of H1N1pdm09 vaccine 1 year after vaccination in military camps during an outbreak. The strength of this study was that the vaccination effectiveness was robust regardless of case definitions and analytical models, and that we considered other factors that could possibly affect influenza outbreak in our analysis.
- In conclusion, the effectiveness of H1N1pdm09 vaccine 1 year after vaccination was approximately 47%, and this study confirmed the results of previous studies, which showed that vaccination effectiveness decreased as time passed.
Discussion
-
Acknowledgements
- This study was supported by the funds of Korea Military Medicine Research Program (2011-KMMRP-OOO).
Acknowledgments
-
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article information
- 1. Orenstein W.A., Bernier R.H., Dondero T.J.. Field evaluation of vaccine efficacy. Bull World Health Organ 63(6). 1985;1055−1068. PMID: 3879673.PubMedPMC
- 2. Orenstein E.W., De Serres G., Haber M.J.. Methodologic issues regarding the use of three observational study designs to assess influenza vaccine effectiveness. Int J Epidemiol 36(3). 2007 Jun;623−631. PMID: 17403908.ArticlePubMed
- 3. Andrews N., Waight P., Yung C.F.. Age-specific effectiveness of an oil-in-water adjuvanted pandemic (H1N1) 2009 vaccine against confirmed infection in high risk groups in England. J Infect Dis 203(1). 2011 Jan;32−39. PMID: 21148494.ArticlePubMed
- 4. Song J.Y., Cheong H.J., Heo J.Y.. Effectiveness of the pandemic influenza A/H1N1 2009 monovalent vaccine in Korea. Vaccine 29(7). 2011 Feb;1395−1398. PMID: 21199701.ArticlePubMed
- 5. Cheong H.J., Song J.Y., Heo J.Y.. Immunogenicity and safety of influenza A (H1N1) 2009 monovalent inactivated split vaccine in Korea. Vaccine 29(3). 2011 Jan;523−527. PMID: 21055502.ArticlePubMed
- 6. Cheong H.J., Song J.Y., Heo J.Y.. Immunogenicity and safety of the influenza A/H1N1 2009 inactivated split-virus vaccine in young and older adults: MF59-adjuvanted vaccine versus nonadjuvanted vaccine. Clin Vaccine Immunol 18(8). 2011 Aug;1358−1364. PMID: 21715575.ArticlePubMed
- 7. Castilla J., Morán J., Martínez-Artola V.. Effectiveness of the monovalent influenza A(H1N1)2009 vaccine in Navarre, Spain, 2009–2010: cohort and case-control study. Vaccine 29(35). 2011 Aug;5919−5924. PMID: 21723358.ArticlePubMed
- 8. Cheng A.C., Kotsimbos T., Kelly H.A.. Effectiveness of H1N1/09 monovalent and trivalent influenza vaccines against hospitalization with laboratory-confirmed H1N1/09 influenza in Australia: a test-negative case control study. Vaccine 29(43). 2011 Oct;7320−7325. PMID: 21810450.ArticlePubMed
- 9. Wu J., Xu F., Lu L.. Safety and effectiveness of a 2009 H1N1 vaccine in Beijing. N Engl J Med 363(25). 2010 Dec;2416−2423. PMID: 21158658.ArticlePubMed
- 10. Mahmud S., Hammond G., Elliott L.. Effectiveness of the pandemic H1N1 influenza vaccines against laboratory-confirmed H1N1 infections: population-based case-control study. Vaccine 29(45). 2011 Oct;7975−7981. PMID: 21884747.ArticlePubMed
- 11. Pelat C., Falchi A., Carrat F.. Field effectiveness of pandemic and 2009–2010 seasonal vaccines against 2009–2010 A(H1N1) influenza: estimations from surveillance data in France. PLoS One 6(5). 2011 May;e19621PMID: 21573005.ArticlePubMed
- 12. Pebody R., Hardelid P., Fleming D.. Effectiveness of seasonal 2010/11 and pandemic influenza A(H1N1)2009 vaccines in preventing influenza infection in the United Kingdom: mid-season analysis 2010/11. Euro Surveill 16(6). 2011 Feb;pii: 19791.Article
- 13. Fielding J.E., Grant K.A., Garcia K., Kelly H.A.. Effectiveness of seasonal influenza vaccine against pandemic (H1N1) 2009 virus, Australia, 2010. Emerg Infect Dis 17(7). 2011 Jul;1181−1187. PMID: 21762570.ArticlePubMed
- 14. Song J.Y., Cheong H.J., Hwang I.S.. Long-term immunogenicity of influenza vaccine among the elderly: risk factors for poor immune response and persistence. Vaccine 28(23). 2010 May;3929−3935. PMID: 20394719.ArticlePubMed
- 15. Nichol K.L.. Heterogeneity of influenza case definitions and implications for interpreting and comparing study results. Vaccine 24(44–46). 2006 Nov10;6726−6728. PMID: 16879901.ArticlePubMed
- 16. Kasper M.R., Wierzba T.F., Sovann L.. Evaluation of an influenza-like illness case definition in the diagnosis of influenza among patients with acute febrile illness in Cambodia. BMC Infect Dis 10:2010 Nov;320PMID: 21054897.ArticlePubMed
- 17.
References
∗Case included patients who had influenza-like illness (≥38 °C and cough/sore throat), which is either self-reported or medically attended; †Adjusted for age group, smoking history, BMI, seasonal influenza vaccination history (past 1 year), past influenza A(H1N1)pdm09 diagnosis history. BMI = body mass index; CI = confidence interval; ILI = influenza-like illness; VE = vaccine effectiveness.
∗Comparing “no” or “self-reported” vaccination with “registry-verified” vaccination; †Comparing “no” vaccination with “registry-verified” vaccination. CI = confidence interval; ILI = all influenza-like illnesses (≥38 °C and cough/sore throat), which are self-reported cases or medically attended cases; ILI MA = influenza-like illness (≥38 °C and cough/sore throat), which is a medically attended case only; ILI SR = influenza-like illness (≥38 °C and cough/sore throat), which is a self-reported case only; VE = vaccine effectiveness.
Figure & Data
References
Citations
- Assessment of Intensive Vaccination and Antiviral Treatment in 2009 Influenza Pandemic in Korea
Chaeshin Chu, Sunmi Lee
Osong Public Health and Research Perspectives.2015; 6(1): 47. CrossRef - Was the Mass Vaccination Effective During the Influenza Pandemic 2009–2010 in Korea?
Hae-Wol Cho, Chaeshin Chu
Osong Public Health and Research Perspectives.2013; 4(4): 177. CrossRef
 PubReader
PubReader Cite
Cite
