
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 3(3); 2012 > Article
-
Articles
Dynamics of Constructs in Successful Aging of Korean Elderly: Modified Rowe and Kahn’s Model - Sang-Nam Jeona, Hakgene Shinb, Hae-Jong Leec
-
Osong Public Health and Research Perspectives 2012;3(3):137-144.
DOI: https://doi.org/10.1016/j.phrp.2012.07.003
Published online: June 30, 2012
aHealth Policy Division, Ministry of National Defense, Seoul, Korea.
bDepartment of Welfare and Counselling, Jeonju Kijeon College, Jeonju, Korea.
cDepartment of Health Administration, Yonsei University, Wonju, Korea.
- Corresponding author. E-mail: shin@kijeon.ac.kr
• Received: April 26, 2012 • Revised: June 20, 2012 • Accepted: June 21, 2012
Copyright ©2012, Korea Centers for Disease Control and Prevention
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License () which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives
- This study examined components in Rowe and Kahn’s successful aging model to investigate their hierarchical order and led to a modification of the previous hierarchical order.
-
Methods
- To examine the hierarchical order of components, we constructed a structural equation model and verified those paths that have discrepancies in studies and/or potential inclusion or omission errors in the model. For this purpose, we analyzed 556 cases out of stratified and purposively sampled 600 elderly people living in the city of Jeonju during the study period (2011).
-
Results
- The paths with inclusion errors such as H3 [self-reported health → productive activity (SRH → PA)]: the effect of SRH on PA, and H6 [social network (SN) → PA]: the effect of SN on PA, were not directly but indirectly supported. The path with discrepancy, H4 [SN → physical–cognitive function (PCF)]: the effect of SN on PCFs, was statistically significant. The path with inclusion error and discrepancy, H8 (PCF → PA): the effect of PCF on PA, was not directly but indirectly supported. Also the path with the omission error, H2 [SRH → psychological trait (PT)]: the effect of SRH on PT, was statistically significant. The other paths in the hierarchical order of the model reported in previous studies were statistically significant.
-
Conclusion
- We verified new dynamics of constructs involved in successful aging, which would provide better understanding of Rowe and Kahn’s successful aging model for Korean elderly people living in a medium-sized city.
- Keywords: productive activity; physical–cognitive function; psychological trait; social network; self-reported health
- Ever since Rowe and Kahn proposed “successful aging” [1,2] to counteract the long-standing tendency of gerontology, that is, emphasizing only a distinction between older people with diseases or disabilities and those suffering from neither, “New Gerontology”, the study deviating from the negative perspective on aging and accepting the diversity of the elderly, has received much attention [3]. Similarly, Bowling and colleagues [4,5] reviewed 170 studies about successful aging and classified them into biomedical theories [1,6] and psycho-social approaches [7-9].
- Although Rowe and Kahn’s model was the most widely accepted approach, one of the limitations of the model was that it failed to address the implications of the fact that a disease-free older age was unrealistic for most people [5]. In addition, psycho-social viewpoints criticized the relatively low factors of social network (SN) and psychological trait (PT) in the model [10,11]. In this context, Kahn proposed a theoretical integration [12] of Rowe and Kahn’s model with studies of Riley [9] and Baltes [13], which has not been studied yet. In spite of the criticisms and shortcomings, we still believe in Rowe and Kahn’s model [1,2,6] and the later-added social and psychological aspects to the model were rather inclusive and more comprehensive than others [7-9,13].
- After all, Rowe and Kahn concluded that successful aging was achieved in the following hierarchical order: “minimize risk and disability”, “maximize physical and cognitive ability”, “engage in activities”. In addition, SN and PT had effects on physical and cognitive function (PCF), and productive activity (PA) respectively, thus supporting this hierarchical order [1,2,9,14-21].
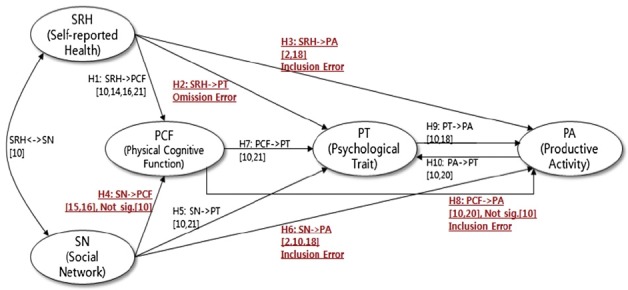
- So far we could find consensus that the model was truly multidimensional [1,4,5,10]. However, like the definition of successful aging still being contentious, there has been some debate about the appropriate hierarchical order of components in Rowe and Kahn’s successful aging as well [10,12,22,23]. Specifically, Rowe and Kahn clarified self-reported health (SRH) and SN were antecedents of PA (H3: SRH → PA and H6: SN → PA), which were potential inclusion errors in their modeling. Also, we speculated that there was a possible omission error in the path between SRH and PT (H2: SRH → PT). In addition, the path of H4: SN → PCF had discrepancies among various studies [10,14,19] and the path of H8: PCF → PA has suspected potential inclusion errors (Figure 1).
- To resolve these discrepancies and inclusion or omission errors, we investigated the effects among latent variables such as H2: SRH → PT, H3: SRH → PA, H4: SN → PCF, H6: SN → PA, H8: PCF → PA, and also analyzed the indirect effects at H2: SRH → PT and H4: SN → PCF. In addition, this study includes the path of H10: PA → PT reported by [10,20] (Figure 1). As a result, we propose a modified version of Rowe and Kahn’s successful aging model for older people residing in a medium-sized Korean city.
1. Introduction
- 2.1. Participants
- The survey was conducted on 600 seniors aged 65 and over, about 1% of the aging population living in the medium-sized city of Jeonju. Stratified sampling was used to allocate the number of samples into two administrative districts and purposively extracted samples of the male/female aging population ratio in the city. Trained surveyors visited the sampled elderly population at welfare centers, senior citizen centers, apartments, and houses in Jeonju from July 20 to August 31, 2011. Before the survey, the questionnaire was verified by five experts in health science, family medicine, and preventive medicine. Some items were added to/deleted from the basic model of Rowe and Kahn. Furthermore, a preliminary survey was carried out on 30 senior citizens in Seoul from May 16 to 20, 2011. The result of this study led to the modification of certain phrases in the previous questionnaire. Eventually, 600 questionnaires were distributed and 100% collection was achieved. Excluding the 44 incomplete or incorrectly answered questionnaires, 556 cases (92.6%) were included in the study.
- 2.2. SRH
- Rowe and Kahn (1998) did not operationalize their definition but later on Strawbridge and colleagues [23], and Bowling and Dieppe [4] did so, which was followed in most of the follow-up studies [3,10].
- This study measured SRH with three indicators: healthy habits, subjective health, and number of chronic diseases. First, for healthy habits, smoking and drinking were measured with the items used in the 2008 2nd Korean Longitudinal Study of Aging. Regular dietary habits and exercise were measured using a 5-point Likert scale based on the suggestions of a gerontology specialist. Second, for subjective health, the Health Rating Scale developed in Northern Illinois University and used by Lee and Park [24] was used. This 5-point scale was composed of two items: one item on current health status perceived by the participant, and one item comparing current health with the health status of the previous year. The Cronbach α value was reported as 0.87 in the previous study [24], whereas it was 0.721 in our study. Third, to measure the number of diseases, we selected a total of 12 chronic diseases including diabetes, cataract (glaucoma), systolic hypertension, stroke, asthma, cancer, heart disease, arthritis, disk (backache), depression, gastritis (peptic ulcers), and prostate disease (urinary incontinence) based on the 2001 Korean National Health and Nutrition Examination Survey of the Ministry of Health and Welfare, and on the study conducted by Andrews and colleagues [25].
- 2.3. SN
- Characteristics of SN have two dimensions: size of SN and social support [23]. However, this study did not include the size of SN based on the contact theory which asserts that quality and not frequency is important in social relationships [26]. In spite of the various forms, social support behavior could be largely classified into two categories: emotional support and instrumental support [10,16]. This study used eight items for emotional support and for instrumental support, respectively. Each item used a 5-point Likert scale. In the study conducted by Sung [10], the Cronbach α value of emotional support was 0.80, whereas the value of instrumental support was 0.83. In this study, the Cronbach α value of emotional support was 0.863, whereas the value of instrumental support was 0.878.
- 2.4. PCF
- Physical function may be defined as the ability to perform physical acts required in daily life. To measure the degree in which the elderly maintained physical function, this study used the following items: “Can you walk 400 m without stopping?”, “Can you climb 30 stairs without stopping?”, “Can you stand up without feeling dizzy?”. These items were used by Strawbridge and colleagues [23] to operationalize Rowe and Kahn’s model.
- Cognitive function could be defined as the ability to perform mental acts required in daily life. To measure cognitive function, this study used the following items adapted by Strawbridge and colleagues [23]: “Can you remember past incidents?”, “Can you remember where you placed an object?”, “Can you easily remember words when you speak?”. In addition, a total of six items, including home address, current date, and recollection of people, were used to find out the ability of the elderly to recognize a certain time, place, situation, or environment correctly [10]. Sung’s [10] Cronbach ga certain time, place, situation, or environmethe value of cognitive function was 0.70. In this study, the Cronbach value of physical function was 0.784, whereas the value of cognitive function was 0.874.
- 2.5. PT
- In MacArthur studies, PT was measured by factors such as self-efficacy, life satisfaction, and depression [15]. Because self-efficacy and life satisfaction embrace positive aspects of PT, and on the contrary, depression encompasses a negative aspect, these constructs were not interchangeable PTs; however, depression was already included as an item of chronic diseases in SRH. Thus, to avoid conflicts and measure a purer construct of positive PT, we excluded depression.
- Self-efficacy could be a belief that one could solve unique problems, confront unique challenges, and influence the affairs occurring in everyday life [11]. This study deployed a total of eight items [17], six items on self-efficacy and two items on interpersonal selfefficacy. Life satisfaction could refer to the subjective satisfaction level for one’s present life. This study measured a total of three items, which was the satisfaction with life scale [27].
- In the previous study [3], the Cronbach udyudy measured a total of tisfaction could the life satisfaction value was 0.789. In this study, the Cronbach . In this study, easured a total of tisfaction could refer to value was 0.873.
- 2.6. PA
- Most people would easily perceive PA, the final domain of the successful aging model, as a concept of paid labor. However, Rowe and Kahn included managing one’s household, taking care of family or friends, volunteering at a church or civic group, and looking after grandchildren in PA. In this study, we used five items—paid labor, volunteer work, group activity, household chores, and taking care of grandchildren—to measure PA according to the scale used by Herzog and colleagues [20], and other MacArthur studies. The participation number numerically expressed the participation in the five domains, whereas the participation time combined the hours participated in each activity variable.
- 2.7. Statistical analyses
- Initially, the cases which have multiple missing values in exogenous and endogenous variables were discarded. Each item in the case with only one missing value at random was replaced with a number computed
- Fitness indices for measurement model
- by a mean substitution method. Also, outliers were screened with Mahalanobis D2 at p < 0.001. Normality and multicollinearity were also assessed. Second, frequency analysis was performed to examine the general information of survey subjects. Third, exploratory factor analysis was deployed to assess construct validity and then internal consistence reliability (Cronbach α) was computed. Fourth, item parceling was applied to items composing a factor for computing index of each indicator. Fifth, confirmatory factor analysis was used to assess factor loadings of indicators and convergence validity as well as discretion validity. Finally, a structural equation model was constructed to estimate regression coefficients between latent variables and to estimate direct–indirect effects. The statistical significances of direct and indirect effects were confirmed by bootstrapping analysis. SPSS 18.0 and AMOS 18.0 were used for statistical analysis.
2. Materials and Methods
Table 1.
| x2 | DF | SRMR | AGFI | TLI (NNFI) | CFI | RMSEA (LO 90-HI 90) |
|---|---|---|---|---|---|---|
|
|
||||||
| 109.105* | 34 | 0.027 | 0.975 | 0.975 | 0.985 | 0.057 (0.044-0.071) |
- 3.1. Demographic characteristics
- Demographic characteristics included gender, age, subjective economic status, religion, and marital status.
- Among the 556 participants, 219 (39.4%) were men and 337 (60.6%) were women. This was approximately the same as the gender ratio of the aging population in the city studied. Age wise, 12.8% of participants were 65–69 years old, 27.3% were 70–74 years old, 32.0% were 75–79 years old, and 27.9% were >80 years old. Regarding educational levels, 38.5% did not have any level of education, 38.8% were elementary school
- Confirmatory factor analysis of measurement model
- graduates, 22.7% were middle school graduates. In this regard, over 75% of the survey participants were elementary school graduates or of lower educational background. About 61.2% selected “low” for subjective economic condition, whereas 35.4% answered “middle” and 3.4% selected “high”. Thus, over half of the participants answered that they were in “low” economic status. Regarding religion, 30.2% of participants were Christian, 18.3% were Buddhists, 15.6% were Catholics, 2.2% believed in other religions, whereas 33.6% reported they did not have any religion. About 21% of the participants answered that they had a spouse, whereas the remaining 79% answered that they did not have a spouse. Thus, nearly 80% of the participants had experienced the loss of a husband or wife.
- 3.2. Confirmatory factor analysis
- Model fitness for measurement was examined as shown in Table 1. First, as a generalized likelihood ratio, model x2 = 109.105 [degreesoffreedom (d.f.) = 34] and normalized x2 = 2.784 were appropriate. Second, as absolute fitness indices, standardized root mean residual (SRMR) = 0.027 which was less than 0.050 and root mean square error of approximation (RMSEA) = 0.057 (low: 0.044; high: 0.071), whose high value did not exceed 0.08 and the average value was close to 0.05, which is enough to be appropriate. Also, as adjusted goodness-of-fit index (AGFI) = 0.940, Tucker Lewis index (non-normalized fit index) [TLI (NNFI)] = 0.975, comparative fit index (CFI) = 0.985, the relative fitness indices implied that the measurement model was appropriate.
- Multicollinearity among latent variables
- As shown in Table 2, all factor loadings of indicators to latent variables presented statistical significance. Although SRH presented a little lower convergent validity (average variance extracted = 0.481) than threshold, it was close to 0.5, which is enough to be marginally accepted; however, other latent variables fulfilled the criterion of convergent validity.
- Before performing structural regression analysis, we used correlation analysis between latent variables to analyze multicollinearity. All relations presented statistical significance (Table 3), while the correlation coefficient between PCF and PT was 0.913, which was higher than threshold (0.900). These two variables were suspicious of multicollinearity. However, they theoretically and empirically were not the same constructs [10,23,28]. Thus, we differentiated them in the model. The discriminant validity between other latent variables was judged to be acceptable and so was the measurement model.
- 3.3. Structural regression analysis
- Structural regression analysis was performed to verify the hierarchical order of constructs in successful aging. Model fitness for structural regression analysis was confirmed (Table 4). First, as a generalized likelihood ratio, model x2 = 95.254 (d.f. = 36) and normalized x2 = 2.646, which were appropriate. Second, as absolute fitness indices, SRMR = 0.027, which was less than 0.050 and RMSEA = 0.055 (low: 0.042; high: 0.068), whose high value did not exceed 0.08 and the average value was close to 0.05, which is enough to be appropriate. Also, as AGFI = 0.944, TLI (NNFI) = 0.977, CFI = 0.985, the relative fitness
- Fitness indices for structural regression model
- indices implied that the structural regression model was appropriate.
- As shown in Figure 2 and Table 5, most of paths were statistically significant. In detail, H1: SRH/PCF, H2: SRH → PT, H4: SN → PCF, H5: SN → PT, H7: PCF → PT, H9: PT → PA, H10: PA → PT were statistically significant. Note that the path with discrepancies between studies (H4: SN → PCF) and the path with omission error (H2: SRH → PCF) were proven to be statistically significant. However, the paths suspected with inclusion error (H3: SRH → PA and H6: SN → PA) were not statistically significant. The path suspected with inclusion error and reported discrepancy among studies (H8: PCF → PA) was not statistically significant either.
- 3.4. Mediating effect
- The paths rejected because of inclusion error and/or discrepancy among studies could have had an indirect effect. Therefore, we analyzed the mediating effects. As presented in Table 6, the paths rejected because of inclusion errors and/or discrepancies among studies did not have a direct but had an indirect effect, which meant that there were mediating effects in those paths. Thus, PCF and PT positively and fully mediated the relationships between SRH and PA (H3) and between SN and PA (H6). Also, PT positively and fully mediated the relationship between PCF and PA (H8).
3. Results
Table 2.
Table 3.
Table 4.
| x2 | DF | SRMR | AGFI | TLI (ZNNFI) | CFI | RMSEA (LO 90-HI 90) |
|---|---|---|---|---|---|---|
|
|
||||||
| 95.254* | 36 | 0.027 | 0.944 | 0.977 | 0.985 | 0.055(0.042-0.068) |
- We observed the successful aging components of Rowe and Kahn’s model to re-examine the hierarchical
- order of the constructs in the model. The results confirmed that SRH and SN served the fundamental role in achieving successful aging. In the meantime, we resolved some discrepancies among studies and some omission or inclusion errors found from previous studies. Below were the selective contributions of this study.
- First, SRH had an effect on PCF. This corresponded with the precedent studies that perception of oneself to be subjectively healthy without diseases positively influenced PCF [3,10,14,16,21].
- Second, SRH, presumed to be an omission error and not covered in previous studies, had an influence on PT. Thus, we included the path from SRH to PT to a modified Rowe and Kahn’s successful aging model.
- Third, SRH did not directly affect PA, which confirmed an inclusion error. However, this did not correspond with the results of the previous studies [2,18]. This causality was supported by indirect effect that PCF and PT mediated between SRH and PA. Thus, those works [2,18] were partially supported.
- Fourth, SN had a positive effect on PCF. This corresponded with the reports that receiving high social support improved physical function and prevented decrease in cognitive function [22,29].
- Path coefficient and significance of structural regression model
- Fifth, SN had a significant influence on PT. This corresponded with the results of several studies that social support positively affected physical health, mental health, stress, depression, and subjective wellbeing [30,31].
- Sixth, SN did not show a direct effect on PA, which confirmed the inclusion error found in [2,10,18]. However, this causality was supported by the indirect effect that PCF and PT mediated between SN and PA. Thus, those works [2,10,18] were partially supported.
- Seventh, PCF significantly affected PT. This corresponded with the results of various studies that showed independently performing daily activities was not only significantly related to psychological well-being such as life satisfaction and self-efficacy, but also effective in achieving successful aging [32]. Physical function was also identified as a variable that has a positive effect on the quality of life [33]. Rowe and Kahn claimed PCF as the most important variable of successful aging because maintaining PCF through steady exercise enhanced the quality of life and helped the elderly to participate actively in social activities.
- Eighth, PT was presented to influence PA. This corresponded with the results of previous studies [2,18], which stated that the relationship between PCF and PA
- Indirect effects of paths with inclusion error and/or discrepancy among studies
- could be changed depending on PT. Furthermore, it also corresponded with the study reported in [10], which concluded that individuals with high level of life satisfaction and self-efficacy could actively participate in society.
- Ninth, PCF had an indirect effect on PA through PT without providing any direct effect. This corresponded with the results of a previous study [10]. It was also comprehended that PCF enhanced social participation only when connected with PT, such as life satisfaction and self-efficacy. This was supportive of the idea that emotional stability and peace were important values for successful aging [34].
- Tenth, PA had an influence on PT, which corresponded with the results of many studies [10,35,36]. This confirmation implied PT could be the final destination of successful aging instead of PA. Note that this interpretation may have the tendency of integrating Rowe and Kahn’s model with psycho-social approaches.
- Although this study resolved some potential modeling errors and discrepancies among studies, there were certain limitations in interpretation of the results. First, participants without spouses accounted for 79% of all survey participants. This was higher than other reports where they accounted for only 49.9% [37], 24% [10], 32.6% [3]. Therefore, cautious interpretation would be needed. Second, cross-sectional research focused only on establishing and verifying the hierarchical order between the five components that were used. In this regard, the model established did not sufficiently consider certain variables, such as disease factors that could change with time. Thus, successive studies could produce results on successful aging with greater accuracy by implementing a longitudinal research on the same subject. Third, the objectivity of measurement could limit the application of the result. Because the measurements are based on subjective perception of the elderly, there was the possibility that responses might have been given in a direction desired by the society. Fourth, the concept of successful aging used in this study was retained on the assumption that successful aging was achieved by actively participating in social activity formed from activity theory [1,2]. However, some studies would not agree with the premise [7-9,13].
- Finally, this study proposes the following for successive studies covering pertinent issues. First, as this study investigated the elderly of a medium city, successive study could explore an expanded sample. Such study would not only contribute to the generalization of research result, but would also construct a more accurate successful aging model. Second, the model of Rowe and Kahn might be slightly different from the real conditions in Korea. In this sense, various theoretical variables could be probed, which would lead to a model reflective of the extensional conditions in Korea.
4. Discussion

Table 5.
Table 6.
| Relevant factors | Standardized weights | ||
|---|---|---|---|
|
|
|||
| Total effects | Direct effect | Indirect effect | |
|
|
|||
| H3: SRH -> PA | 0.411* | 0.000 | 0.411* |
| H6: SN -> PA | 0.235* | 0.000 | 0.235* |
| H8: PCF -> PA | 0.255* | 0.000 | 0.255* |
- 1. Rowe JW Kahn RL. . Successful aging. Gerontologist 8;1997;37(4). 433−40. PMID: 9279031.ArticlePubMed
- 2. Rowe JW Kahn RL. . Successful aging.. Random House; New York: 1998.
- 3. Lee GO. . A structural analysis of successful aging factors of rural elders (dissertation).. Seoul National University; 2007. [in Korean].
- 4. Bowling A Dieppe P. . What is successful ageing and who should define it? BMJ 12;2005;331(7531). 1548−51. PMID: 16373748.ArticlePubMedPMC
- 5. Bowling A Iliffe S. . Which model of successful ageing should be used? Baseline findings from a British longitudinal survey of ageing. Age Ageing 11;2006;35:607−14. PMID: 16951427.ArticlePubMed
- 6. Phelan EA Anderson LA LaCroix AZ Larson EB. . Old adults’ views of “successful aging” –how do they compare with researchers’ definitions?”. JAm Geriatr Soc 2;2004;52(2). 211−6. PMID: 14728629.Article
- 7. Havighurst RL Neugarten B Tobin SS. . Middle age and aging: a reader in social psychology. In: Neugarten BL, editor. Disengagement and patterns of aging.. University of Chicago Press; Chicago: 1968. pp 161−72. chapter 16.
- 8. Ryff CD. . Beyond Ponce de Leon and life satisfaction: new directions in quest of successful aging. Int J Behav Dev 3;1989;12:35−55.Article
- 9. Riley MW Riley JW. . Age and structural lag. In: Riley MW, Kahn RL, Foner A, editors. Structural lag: past and future.. Wiley; New York: 1990. pp 15−36. [chapter 1].
- 10. Sung HY Cho HS. . A study of successful aging model: using the components of Rowe and Kahn. J Korean Gerontol Soc 3;2005;26(1). 105−23. [in Korean].
- 11. Lee SL Cho SH. . Aging and wisdom: an integrated conceptualization of successful aging. Korean J Psychol Soc Issues 9;2007;13(3). 65−87. [in Korean]..
- 12. Kahn RL. . On Successful aging and well-being: self-rated compared with Rowe and Kahn”. Gerontologist 12;2002;42(6). 727−33. PMID: 12451153.ArticlePubMed
- 13. Baltes PB. . On the incomplete architecture of human ontogeny. Selection, optimization, and compensation as foundation of developmental theory. Am Psychol 4;1997;52(4). 366−80. PMID: 9109347.ArticlePubMed
- 14. Seeman TE Berkman LF Charpentier PA Blazer DG Albert MS Tinetti ME. . Behavioral and psychosocial predictors of physical performance: MacArthur studies of successful aging. J Gerontol A Biol Sci Med Sci 7;1995;50(4). M177−83. PMID: 7614238.ArticlePubMed
- 15. Seeman TE Bruce ML McAvay GJ. . Social network characteristics and onset of ADL disability: MacArthur studies of successful aging. J Gerontol B Psychol Sci Soc Sci 7;1996;51(4). S191−200. PMID: 8673648.ArticlePubMed
- 16. Seeman T Chen X. . Risk and protective factors for physical functioning in older adults with and without chronic conditions: MacArthur studies of successful aging. J Gerontol B Psychol Sci Soc Sci 5;2002;57(3). S135−44. PMID: 11983740.ArticlePubMed
- 17. Seeman TE Rodin J Albert M. . Self-efficacy and cognitive performance in high-functioning older individuals: MacArthur studies of successful aging. J Aging Health 11;1993;5(4). 455−74.Article
- 18. Glass TA Seeman TE Herzog AR Kahn R Berkman LF. . Change in productive activity in late adulthood:MacArthur studies of successful aging. J Gerontol B Psychol Sci Soc Sci 3;1995;50(2). S65−76. PMID: 7757842.ArticlePubMed
- 19. Unger JB McAvay G Bruce ML Berkman L Seeman T. . Variation in the impact of social network characteristics on physical functioning in elderly persons: MacArthur studies of successful aging. J Gerontol B Psychol Sci Soc Sci 9;1999;54(5). S245−51. PMID: 10542826.ArticlePubMed
- 20. Herzog AR Kahn RL Morgan JN Jackson JS Antonucci TC. . Age differences in productive activities. J Gerontol 7;1989;44(4). S129−38. PMID: 2738316.ArticlePubMed
- 21. Tabbarah M Crimmins EM Seeman TE. . The relationship between cognitive and physical performance: MacArthur studies of successful aging. J Gerontol A Biol Sci Med Sci 4;2002;57(4). M228−35. PMID: 11909888.ArticlePubMed
- 22. Everard KM Lach HW Fisher EB Baum MC. . Relationship of activity and social support to the functional health of older adults. J Gerontol B Psychol Sci Soc Sci 7;2000;55(4). 208−12.Article
- 23. Strawbridge WJ Wallhagen MI Cohen RD. . Successful aging and well-being: self-rated compared with Rowe and Kahn. Gerontologist 12;2002;42(6). 727−33. PMID: 12451153.ArticlePubMed
- 24. Lee KJ Park HS. . A study on the perceived health status, depression, and activities of daily living for the elderly in urban areas. Korean J Women Health Nurs 9;2006;12(3). 221−30. [in Korean]..Article
- 25. Andrews G Michael C Mary L. . Successful aging in the Australian longitudinal study of aging: applying the MacArthur model cross-nationally. J Soc Issues 2;2003;58(4). 749−65.Article
- 26. Bousfield C Hutchison P. . Contact, anxiety and young people’s attitudes and behavioral intentions towards the elderly. Educ Gerontol 4;2010;36(6). 451−66.Article
- 27. Diener E Emmons RA Larsen RJ Griffin S. . The life satisfaction with life scale. J Pers Assess 2;1985;49:71−5. PMID: 16367493.ArticlePubMed
- 28. Kubzansky LD Berkman LF Seeman TE. . Social conditions and distress in elderly persons: findings from the MacArthur studies of successful aging. J Gerontol B Psychol Sci Soc Sci 7;2000;55(4). 238−46.Article
- 29. Kaplan GA Strawbridge WJ Camacho T Cohen RD. . Factors associated with change in physical functioning in the elderly: a six-year prospective study. J Aging Health 2;1993;5(1). 140−53.Article
- 30. Cutrona CE. . Stress and social support in search of optimal matching. J Soc Clin Psychol 9;1990;9:3−14.Article
- 31. Fernandez-Ballesteros R. . Social support and quality of life among older people in Spain. J Soc Issues Winter;2002;58(4). 645−59.Article
- 32. Chou KL Chi I Chow NW. . Sources of income and depression in elderly Hong Kong Chinese: mediating and moderating effects of social support and financial strain. Aging Ment Health 5;2004;8(3). 212−21. PMID: 15203402.ArticlePubMed
- 33. Jeon SN Shin HG. . The effects of perceived health and ageism experience on successful aging. J Korean Gerontol Soc 12;2009;29(4). 1383−96. [in Korean].
- 34. Choi HK. . The concept of successful aging as perceived by Korean elderly: constructing concepts and intervention strategies in Korean cultural context. J Fam Relat 9;2008;13(3). 145−68. [in Korean].
- 35. Van Willigen M. . Differential benefits of volunteering across the life course. J Gerontol B Psychol Sci Soc Sci 9;2000;55(5). S308−18. PMID: 10985302.ArticlePubMed
- 36. Morrow-Howell N Hinterlong J Rozario PA Tang F. . Effects of volunteering on the well-being of older adults. J Gerontol B Psychol Sci Soc Sci 5;2003;8B:137−45.Article
- 37. Statistics Korea. Korean Statistical Information Service. Available at: http://kosis.kr/index/index.jsp. [accessed 23.5.2011]..
Figure & Data
References
Citations
Citations to this article as recorded by 
- The Concept of Successful Aging: A Review Article
Fatemeh Estebsari, Maryam Dastoorpoor, Zahra Rahimi Khalifehkandi, Azadeh Nouri, Davoud Mostafaei, Meimanat Hosseini, Roghayeh Esmaeili, Hamidreza Aghababaeian
Current Aging Science.2020; 13(1): 4. CrossRef - Perceptions of Successful Ageing Among Iranian Elders
Nasibeh Zanjari, Maryam Sharifian Sani, Meimanat Hosseini Chavoshi, Hassan Rafiey, Farahnaz Mohammadi Shahboulaghi
The International Journal of Aging and Human Devel.2016; 83(4): 381. CrossRef - An Educational Program Based on the Successful Aging Approach on Health-Promoting Behaviors in the Elderly: A Clinical Trial Study
Fatemeh Estebsari, Mohammad Hossein Taghdisi, Abbas Rahimi Foroushani, Hasan Eftekhar Ardebili, Davoud Shojaeizadeh
Iranian Red Crescent Medical Journal.2014;[Epub] CrossRef
 PubReader
PubReader Cite
Cite

