Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 14(1); 2023 > Article
-
Special Article
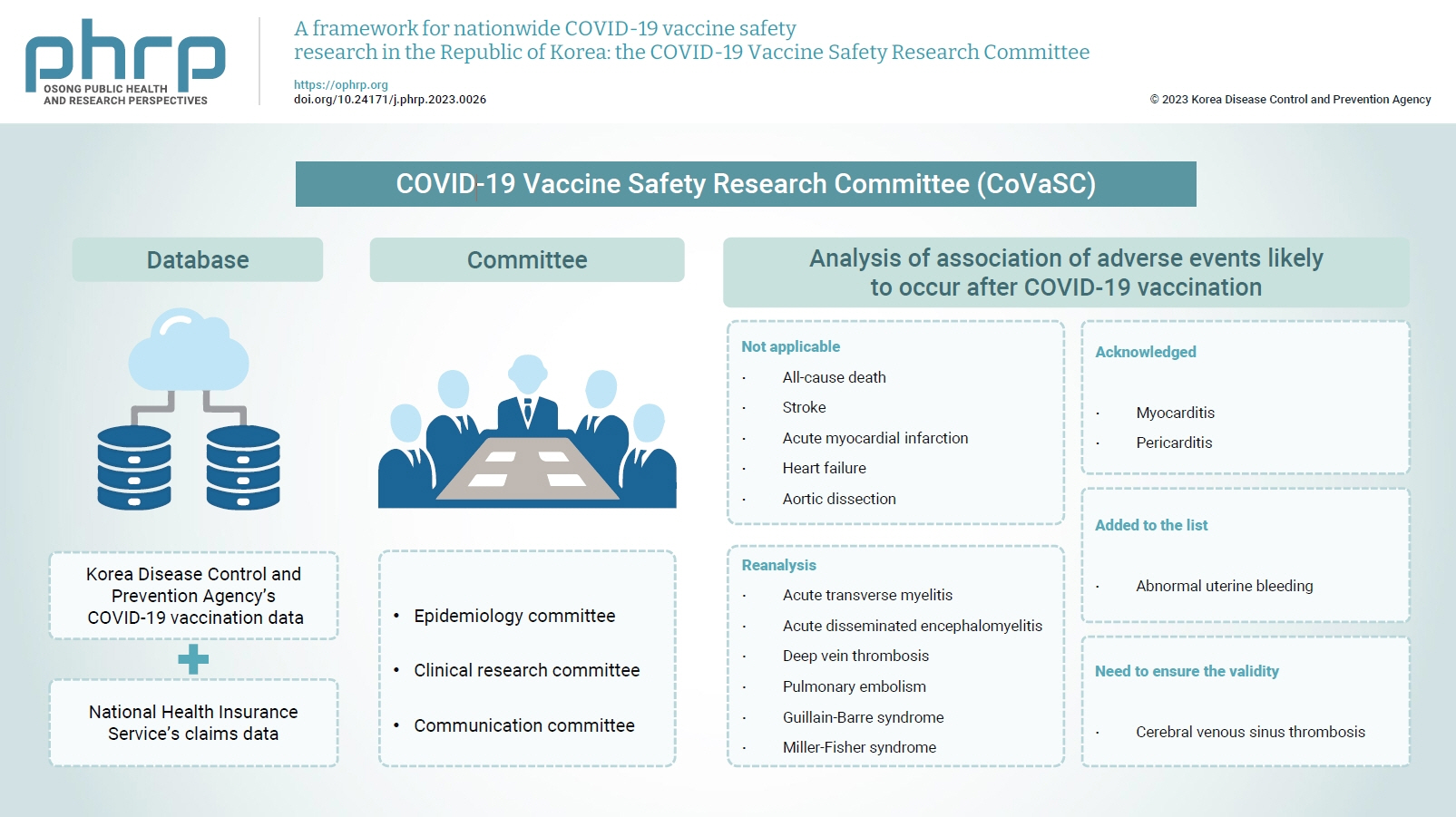
A framework for nationwide COVID-19 vaccine safety research in the Republic of Korea: the COVID-19 Vaccine Safety Research Committee -
Na-Young Jeong1,2
 , Hyesook Park1,3,4, Sanghoon Oh1,5, Seung Eun Jung1,4,6, Dong-Hyun Kim1,7, Hyoung-Shik Shin1,8, Hee Chul Han1,4,9, Jong-Koo Lee1,4, Jun Hee Woo1,4, Byung-Joo Park1,4, Nam-Kyong Choi1,2
, Hyesook Park1,3,4, Sanghoon Oh1,5, Seung Eun Jung1,4,6, Dong-Hyun Kim1,7, Hyoung-Shik Shin1,8, Hee Chul Han1,4,9, Jong-Koo Lee1,4, Jun Hee Woo1,4, Byung-Joo Park1,4, Nam-Kyong Choi1,2 -
Osong Public Health and Research Perspectives 2023;14(1):5-14.
DOI: https://doi.org/10.24171/j.phrp.2023.0026
Published online: February 28, 2023
1COVID-19 Vaccine Safety Research Center, Seoul, Korea
2Department of Health Convergence, College of Science & Industry Convergence, Ewha Womans University, Seoul, Korea
3Department of Preventive Medicine, College of Medicine, Graduate Program in System Health Science & Engineering, Ewha Womans University, Seoul, Korea
4National Academy of Medicine of Korea, Seoul, Korea
5Department of Psychiatry, Uijeongbu Eulji Medical Center, Eulji University School of Medicine, Uijeongbu, Korea
6Department of Radiology, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
7Department of Social and Preventive Medicine, Hallym University College of Medicine, Chuncheon, Korea
8Department of Infectious Diseases, Daejeon Eulji Medical Center, Eulji University School of Medicine, Daejeon, Korea
9Department of Physiology, Korea University College of Medicine, Seoul, Korea
- Co-Corresponding author: Byung-Joo ParkNational Academy of Medicine of Korea, 51 Seochojungang-ro, Seocho-gu, Seoul 06654, Korea E-mail: bjpark@snu.ac.kr
- Corresponding author: Nam-Kyong Choi Department of Health Convergence, College of Science & Industry Convergence, Ewha Womans University, Seoul, Korea E-mail: nchoi@ewha.ac.kr
© 2023 Korea Disease Control and Prevention Agency.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
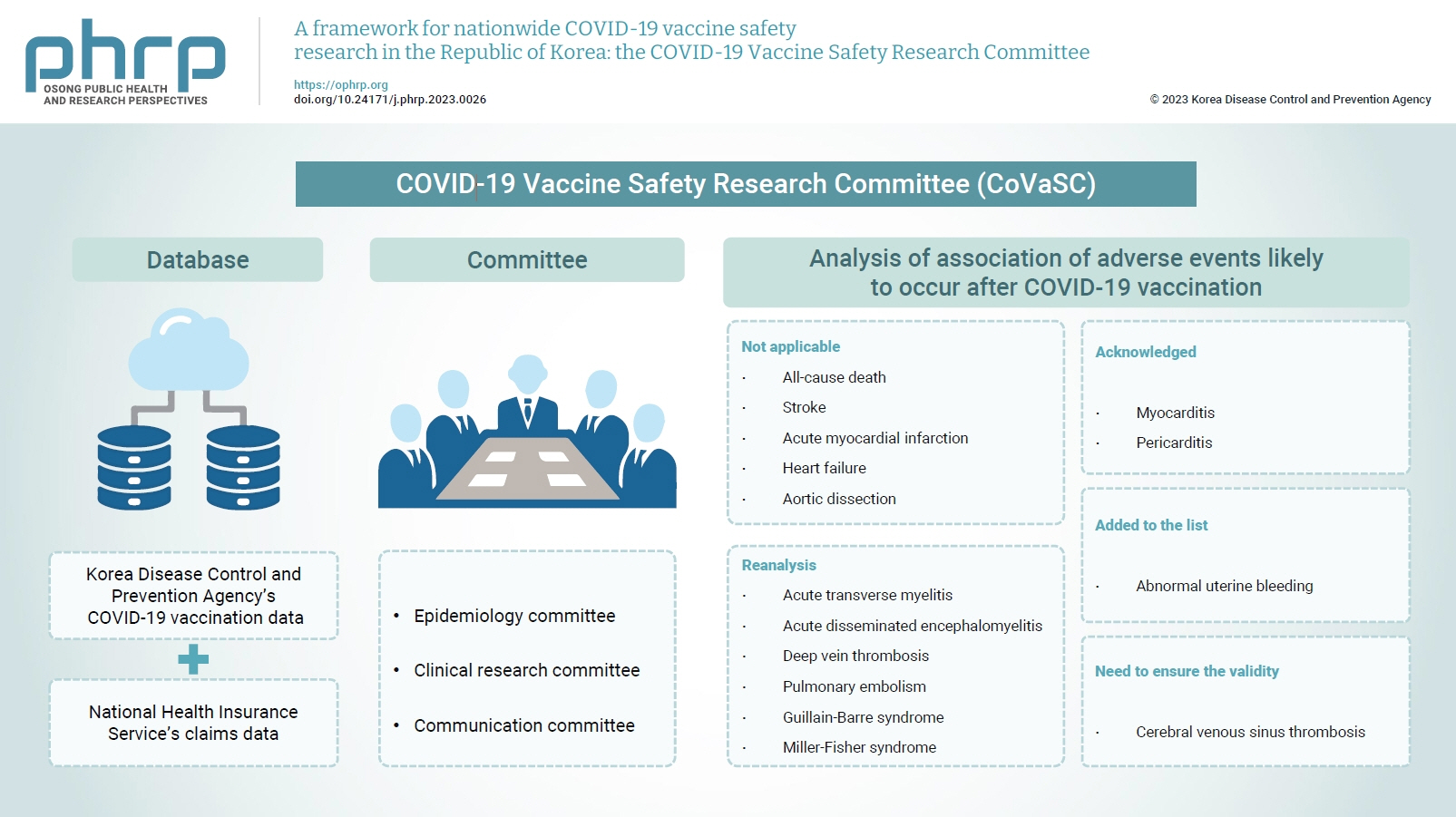
Figure & Data
References
Citations
- Risk of encephalitis and meningitis after COVID-19 vaccination in South Korea: a self-controlled case series analysis
Ju Hwan Kim, Dongwon Yoon, Hwa Yeon Ko, Kyungyeon Jung, Jun-Sang Sunwoo, Won Chul Shin, Jung-Ick Byun, Ju-Young Shin
BMC Medicine.2024;[Epub] CrossRef - To become a more stronger and safer country
Jong-Koo Lee
Osong Public Health and Research Perspectives.2023; 14(2): 67. CrossRef - Risk of lymphadenopathy from SARS-CoV-2 vaccination in Korea: a self-controlled case series analysis
Mi-Sook Kim, Bongyoung Kim, Jeong Pil Choi, Nam-Kyong Choi, Jung Yeon Heo, Jun Yong Choi, Joongyub Lee, Sang Il Kim
Epidemiology and Health.2023; 45: e2023090. CrossRef
 Cite
Cite