
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 8(3); 2017 > Article
-
Original Article
Long-term Treatment with Anti-platelet Agents for Collagen-induced Arthritis Improves Radiological Findings - Chan Kima, Toyou Kimb, Jihyung Yooc, Dong-Hyuk Sheenc, Sang Kwang Leed, Eun-Hye Choid, Tong Jin Chune, Seong-wook Kangf, Seung-Cheol Shimf, Mi-Kyoung Limc
-
Osong Public Health and Research Perspectives 2017;8(3):179-184.
DOI: https://doi.org/10.24171/j.phrp.2017.8.3.04
Published online: June 30, 2017
aDepartment of Physiology, Eulji University School of Medicine, Daejeon, Korea
bDepartment of Mechanical Engineering, the Cooper Union, New York, NY, USA
cDivision of Rheumatology, Department of Medicine, Eulji University School of Medicine, Daejeon, Korea
dEulji Medi-Bio Research Institute, Eulji University School of Medicine, Daejeon, Korea
eDepartment of Radiology, Eulji University School of Medicine, Daejeon, Korea
fDivision of Rheumatology, Daejeon Rheumatoid & Degenerative Arthritis Center, Chungnam National University Hospital, Daejeon, Korea
- Corresponding author: Mi-Kyoung Lim, E-mail: mklim@eulji.ac.kr
- *Chan Kim and Toyou Kim contributed equally to this work.
• Received: March 21, 2017 • Revised: May 9, 2017 • Accepted: May 15, 2017
Copyright ©2017, Korea Centers for Disease Control and Prevention
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
- 3,500 Views
- 19 Download
- 1 Scopus
Abstract
-
Objectives
- The objectives of this study were to evaluate the long-term effect of anti-platelet treatment on the radiological progression of collagen-induced arthritis in rats.
-
Methods
- Female Lewis rats with collagen-induced arthritis were divided into three experimental groups: saline, aspirin monotherapy (n = 12), and aspirin–clopidogrel dual therapy (n = 12). Drugs were administered daily and continued up to 70 days after the induction of arthritis. The clinical arthritis index (weight, morphology score, and paw thickness) and radiological scores were evaluated.
-
Results
- The clinical arthritis index peaked on day 20, while the radiological scores peaked on day 35. No intergroup difference was observed in the clinical arthritis index throughout the experiment. The aspirin–clopidogrel dual therapy group had a significantly higher mean radiological score than the other groups (p = 0.045) on day 35. Further treatments resulted in significantly improved radiological findings in the aspirin monotherapy and aspirin–clopidogrel dual therapy groups on day 70 but no significant improvement in the saline group.
-
Conclusion
- Anti-platelet agent treatment improved radiological findings on day 70. These observations emphasize the importance of a future long-term study of the effects of anti-platelet agent treatment on arthritis.
- An increased risk of cardiovascular disease (CVD) associated with rheumatoid arthritis (RA) has been observed over the past few decades. RA has been identified as an independent risk factor of premature ischemic heart disease [1]. As observed in patients with type 2 diabetes mellitus, CVD occurs 10 years earlier in patients with RA than in healthy individuals [2]. In one survey of 9,093 patients with RA and 2,479 patients with OA, RA patients reported a significantly higher prevalence of current myocardial infarction (odds ratio [OR], 2.14; 95% confidence interval [CI], 1.48–3.09) and congestive heart failure (OR, 1.43; 95% CI, 1.28–1.59) [3].
- The increased comorbidity of CVD in patients with RA and the chronic use of anti-platelet agents by patients with CVD motivated us to investigate the effect of anti-platelet agent use on RA. Recent studies have also revealed that platelets play an important role in inflammatory disease, especially in the pathogenesis of RA. Reducing the number of platelets by 95% via the use of a platelet-depleting antibody causes significant improvement in the clinical condition and histological score of patients with RA [4]. Heterotypic platelet–monocyte and platelet–neutrophil complexes have been observed in blood samples of patients with RA [5].
- Although the relationship between anti-platelet agents and RA is being steadily explored, studies published to date cannot verify the long-term effects of anti-platelet agents on RA. Recent studies assessing the relationships between platelets and arthritis lasted less than 3 weeks [4,6], a duration that is insufficient for verifying long-term relationships. A study with a longer duration is needed to fully investigate the effects of anti-platelet agents on RA since CVD and RA are chronic diseases. In addition, clopidogrel and ticlopidine showed conflicting effects on RA symptoms despite belonging to the same class of anti-platelet agents, adenosine diphosphate receptor inhibitors [4,6,7].
- This study aimed to verify the long-term effect of aspirin monotherapy and aspirin–clopidogrel dual therapy, two commonly used anti-platelet treatments for CVD, on the radiological progression of collagen-induced arthritis, and compare the effectiveness of these treatments.
INTRODUCTION
- 1. Animals
- Thirty-six 7-week-old female specific pathogen-free Lewis rats (Samtaco Inc., Osan, Korea) were used in the experiments after a 1-week adaptation period. The animals were raised in a temperature-controlled room (21°C ± 1°C) under normal 12 h:12 h light-dark cycles (200–300 lux) with food and water provided ad libitum. The experiment was conducted according to the University’s institutional guidelines, which are based on the National Institutes of Health Guide for the Care and Use of Laboratory Animals (NIH Publications No.80-23, 1996), and the study was approved by the Animal Research Committee of Eulji University.
- 2. Experimental groups and treatments
- The animals received a primary immunization at the tail base consisting of bovine type II collagen (CII; 4 mg/mL in 0.05 M acetic acid) emulsified 1:1 in complete Freund’s adjuvant (Difco, 4 mg/mL Mycobacterium tuberculosis H37Ra) in a total volume of 200 μL. After 1 week, the animals were boosted with CII in incomplete Freund’s adjuvant in a total volume of 100 μL.
- At 8 weeks of age, the 36 rats were randomly divided into the saline group (n = 12), aspirin monotherapy group (5 mg/kg of aspirin, n = 12), and aspirin–clopidogrel dual therapy group (5 mg/kg of aspirin and 10 mg/kg of clopidogrel, n = 12). The rats received orally administered corresponding 3 days prior to the primary immunization, followed by daily oral administration for 70 days. Four animals from each group were sacrificed on days 20, 35, and 70 for histological and radiological analyses.
- 3. Clinical observation
- Body weight, paw thickness, and morphology scores of the animals were evaluated to assess arthritis development every 2 or 3 days after primary immunization. Paw thickness was measured with a constant-tension caliper (Dyer, Lancaster, PA, USA) by two observers and the mean value was used. The morphology score of arthritis in each affected joint was graded according to an established scoring system on a scale of 0 to 4 for a maximum score of 16 [8].
- 4. Radiology
- The radiographic analysis was performed with a 40-kW X-ray exposure for 0.01 seconds (Philips X12 mammography; Philips, Munich, Germany). Both hind limbs were radiographically taken (exposure at 38 kV, 500 mA, 232.38 msec using Kodak M film; Kodak, Rochester, NY, USA) for the analysis. Two experts who were blinded to the treatment regimen scored the radiographic findings in the knee and ankle joints of each hind limb using a scale of 0 to 3 as follows: 0 = normal, 1 = tissue swelling and edema, 2 = joint erosion, and 3 = bone erosion and osteophyte formation.
- 5. Statistical analysis
- Differences among treatment groups were analyzed by one-way analysis of variance (ANOVA) followed by Scheffé’s post-hoc test. The Kruskal-Wallis test was used to verify the differences when the data failed the tests for homogeneity of variances. Values of p < 0.05 were considered statistically significant. The statistical analysis was performed using the IBM SPSS Statistics program for Windows, standard version (version 19.0; IBM Co., Armonk, NY, USA).
- The intra-class correlation coefficient (ICC) was evaluated to determine the degree of agreement for the radiological scores recorded by the two experts. ICC was interpreted according to the scale suggested by Landis and Koch [9]: slight agreement (0–0.20), fair agreement (0.21–0.40), moderate agreement (0.41–0.60), substantial agreement (0.61–0.80), and almost perfect agreement (0.81–1). Spearman’s test was used to determine the correlation between the radiological scores provided by the two experts.
MATERIALS AND METHODS
- 1. Anti-platelet agents did not affect the clinical development of RA
- During the 70-day period, there was no significant effect of treatment on the clinical parameters examined in this study, and most animals developed arthritis 2 weeks after the primary immunization. Clinical arthritis index parameters, i.e., body weight, paw thickness, and morphology score, peaked on day 20. The rats gradually recovered afterwards, the parameters became invariant at approximately day 35, and there were no significant differences among the three groups (Figure 1).
- 2. Anti-platelet agent use improved radiological scores during the chronic phase
- The ICC for the radiological scores recorded by the two experts was 0.727 (p < 0.01; 95% CI, 0.526–0.851), which indicated substantial agreement according to the scale suggested by Landis and Koch [9]. The Spearman’s ρ value was 0.667 (p < 0.01, R = 0.735), which showed a strong correlation between the two radiological scores.
- In all groups, radiological scores of all groups significantly changed over time (Table 1, Figure 2). On day 35, group comparisons revealed that the aspirin–clopidogrel dual therapy group had a significantly higher mean score than the saline and aspirin monotherapy groups (F = 3.668, p = 0.045), and there was no difference between the saline and aspirin monotherapy groups. On day 70, the aspirin monotherapy group and the aspirin–clopidogrel dual therapy group had significantly lower mean scores than the saline group (F = 6.338, p = 0.008), and no difference was observed between the aspirin monotherapy and aspirin–clopidogrel dual therapy groups (Table 2, Figure 2).
RESULTS
- An increasing number of studies have assessed the relationship between platelets and RA. However, studies published to date were not long enough to fully investigate this relationship since their durations were too short to cover the entire RA disease process. It is necessary to observe the relationship on a long-term basis; therefore, here we observed the anti-arthritic effects of long-term anti-platelet agent treatment.
- The clinical arthritis index showed a similar tendency regardless of treatment type throughout the entire experimental period, and there was no significant difference among the three groups (Figure 1). Our result reveals that aspirin monotherapy and aspirin–clopidogrel dual therapy did not improve RA. It is well known that aspirin exerts dose-dependent effects and that the dose required to achieve an anti-inflammatory effect is higher than the anti-platelet effect dose, i.e., low-dose aspirin. We used low-dose aspirin in the treatment groups to simulate its usage in patients with CVD, and we believe that the aspirin treatment groups failed to show improvements in clinical manifestations due to the dosage, which was insufficient to have an anti-inflammatory effect. Previous reports on K/BxN serum– and peptidoglycan polysaccharide-induced arthritis (PG-PS)–induced arthritis showed that clopidogrel monotherapy worsens arthritis [4,6]. In a study on PG-PS–induced arthritis [6], clopidogrel worsened the pathological parameters and histological score on day 21. Garcia et al. [6] showed a significant decrease in anti-inflammatory interleukin-10 (IL-10) plasma levels in the PG-PS–induced arthritis animals treated with clopidogrel. The proinflammatory effect of clopidogrel is thought to act as an antagonist to the P2Y12 receptor, whose stimulation increases IL-10 release. Moreover, there are clinical reports on clopidogrel-associated arthritis in which clopidogrel therapy was followed by the occurrence of abrupt arthritis and hyperthermia [10,11].
- Although significant changes in clinical manifestations occurred during the acute phase (day 20), the radiological findings assessed as scores were not significant. This is due to the nature of the radiological scoring system since the main manifestation in the acute phase, i.e. soft tissue swelling, corresponds to the lowest score. In the sub-acute and chronic phases, changes in the joints and bones led to higher radiological scores. On day 35, radiological scores in all treatment groups were significantly increased, and specifically, the mean score of the aspirin–clopidogrel dual therapy group was significantly higher than those of the other groups. On day 70, most of the scores in the aspirin mono-therapy and aspirin–clopidogrel dual therapy groups mostly had recovered, but radiological findings persisted in the saline group. Our results show that a duration of 35 days, which is longer than the duration in the other arthritis studies, is insufficient to observe the radiological improvements induced by anti-platelet agents. Therefore, we emphasize the need for a long-term duration of an arthritis study, which is further accentuated during the assessment of radiological progress.
- Weicht et al. [12] showed that platelet increases osteoclastogenesis through tumor growth factor β and p38 signaling during the process of osteoclast differentiation. Therefore, platelet suppression may play a positive role in bone changes via affecting osteoclastogenesis. A recent study reported that clopidogrel inhibits osteoclast formation, viability, and resorptive activity by acting as a P2Y12 receptor antagonist [13], which explains the positive effect of clopidogrel on bone changes in our study. Our study revealed that long-term treatment with aspirin has a positive effect on bone changes. We think that this is related to the inhibitory effect of aspirin on tumor necrosis factor-α– and IL-1–induced NF-kappa B activation, as NF-kappa B plays a significant role in bone erosion in RA [14,15].
- There are some conflicting results in the currently existing studies with respect to the effect of clopidogrel. Grimaldi [7] reported that low dose treatment with ticlopidine in RA for 18 months, which has the same mechanism as clopidogrel, improved the counts of the involved joints and other inflammatory markers. However, in recent studies, clopidogrel significantly increased ankle thickness in K/BxN serum-transfer arthritis [4] and aggravated the clinical and pathological manifestations of PG-PS–induced arthritis [6].
- Despite the conflicting results obtained studies, many studies have provided evidence of a close association between platelets and inflammatory arthritis. We observed the beneficial effect of long-term aspirin monotherapy and aspirin–clopidogrel dual therapy in rats with collagen-induced arthritis and noted improvements in bone changes. While the verification was successful, the results of our study are limited by the small number of animals and absence of a clopidogrel monotherapy group that would be needed for comparison with existing studies. In further studies, it will be necessary to study the drug interaction between the anti-platelet agents and anti-rheumatic drugs via co-administration in an animal arthritis model. Moreover, our area of study could be expanded by investigations of other anti-platelet agents and the use of more accurate imaging techniques such as magnetic resonance imaging and computed tomography. Lastly, a large-scale prospective and retrospective cohort study is required to evaluate how the long-term administration of anti-platelet agents affects patients with RA.
DISCUSSION
-
Acknowledgements
- This work was supported by EMBRI Grants 2012-EMBRI DJ 0004 from the Eulji University and the Bio & Medical Technology Development Program of the NRF funded by the Korean government, MSIP (No. 2016M3A9B694241).
ACKNOWLEDGMENTS
- 1. del Rincón ID, Williams K, Stern MP, et al. High incidence of cardiovascular events in a rheumatoid arthritis cohort not explained by traditional cardiac risk factors. Arthritis Rheum 2001;44:2737−45. https://doi.org/10.1002/1529-0131(200112)44:12<2737::AID-ART460>3.0.CO;2-#. PMID: 10.1002/1529-0131(200112)44:12<2737::AID-ART460>3.0.CO;2-#. PMID: 11762933.ArticlePubMed
- 2. Bacon PA, Stevens RJ, Carruthers DM, et al. Accelerated atherogenesis in autoimmune rheumatic diseases. Autoimmun Rev 2002;1:338−47. https://doi.org/10.1016/S1568-9972(02)00100-3. PMID: 10.1016/S1568-9972(02)00100-3. PMID: 12848989.ArticlePubMed
- 3. Wolfe F, Freundlich B, Straus WL. Increase in cardiovascular and cerebrovascular disease prevalence in rheumatoid arthritis. J Rheumatol 2003;30:36−40. PMID: 12508387.PubMed
- 4. Boilard E, Nigrovic PA, Larabee K, et al. Platelets amplify inflammation in arthritis via collagen-dependent microparticle production. Science 2010;327:580−3. https://doi.org/10.1126/science.1181928. PMID: 10.1126/science.1181928. PMID: 20110505.ArticlePubMedPMC
- 5. Pamuk GE, Vural O, Turgut B, et al. Increased platelet activation markers in rheumatoid arthritis: are they related with subclinical atherosclerosis? Platelets 2008;19:146−54. https://doi.org/10.1080/09537100701210057. PMID: 10.1080/09537100701210057. PMID: 17852775.ArticlePubMed
- 6. Garcia AE, Mada SR, Rico MC, et al. Clopidogrel, a P2Y12 receptor antagonist, potentiates the inflammatory response in a rat model of peptidoglycan polysaccharide-induced arthritis. PloS One 2011;6:e26035https://doi.org/10.1371/journal.pone.0026035. PMID: 10.1371/journal.pone.0026035. PMID: 22028806.ArticlePubMedPMC
- 7. Grimaldi MG. Long-term low dose ticlopidine treatment in rheumatoid arthritis: effects on serum sulphydryl levels, technetium index, erythrocyte sedimentation rate, and clinical disease activity. Eur J Clin Pharmacol 1985;29:165−8. https://doi.org/10.1007/BF00547416. PMID: 10.1007/BF00547416. PMID: 3000794.ArticlePubMed
- 8. Bakharevski O, Stein-Oakley AN, Thomson NM, et al. Collagen induced arthritis in rats. Contrasting effect of subcutaneous versus intradermal inoculation of type II collagen. J Rheumatol 1998;25:1945−52. PMID: 9779848.PubMed
- 9. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;33:159−74. https://doi.org/10.2307/2529310. PMID: 10.2307/2529310. PMID: 843571.ArticlePubMed
- 10. Kawashiri SY, Taguchi M, Kawakami A, et al. Clopidogrel-associated acute arthritis. Rheumatol Int 2012;32:449−50. https://doi.org/10.1007/s00296-009-1267-y. PMID: 10.1007/s00296-009-1267-y. PMID: 20024558.ArticlePubMed
- 11. Swennen EL, Bast A, Dagnelie PC. Immunoregulatory effects of adenosine 5′-triphosphate on cytokine release from stimulated whole blood. Eur J Immunol 2005;35:852−8. https://doi.org/10.1002/eji.200425423. PMID: 10.1002/eji.200425423. PMID: 15719372.ArticlePubMed
- 12. Weicht B, Maitz P, Kandler B, et al. Activated platelets positively regulate RANKL-mediated osteoclast differentiation. J Cell Biochem 2007;102:1300−7. https://doi.org/10.1002/jcb.21360. PMID: 10.1002/jcb.21360. PMID: 17957725.ArticlePubMed
- 13. Syberg S, Brandao-Burch A, Patel JJ, et al. Clopidogrel (Plavix), a P2Y12 receptor antagonist, inhibits bone cell function in vitro and decreases trabecular bone in vivo. J Bone Miner Res 2012;27:2373−86. https://doi.org/10.1002/jbmr.1690. PMID: 10.1002/jbmr.1690. PMID: 22714653.ArticlePubMed
- 14. Zhu G, Cai J, Zhang J, et al. Abnormal nuclear factor (NF)-kappaB signal pathway and aspirin inhibits tumor necrosis factor alpha-induced NF-kappaB activation in keloid fibroblasts. Dermatol Surg 2007;33:697−708. https://doi.org/10.1111/j.1524-4725.2007.33146.x. PMID: 17550447.ArticlePubMed
- 15. Cuesta E, Boada J, Perales JC, et al. Aspirin inhibits NF-kappaB activation in a glycolysis-depleted lung epithelial cell line. Eur J Pharmacol 2005;517:158−64. https://doi.org/10.1016/j.ejphar.2005.05.024. PMID: 10.1016/j.ejphar.2005.05.024. PMID: 15987633.ArticlePubMed
REFERENCES
Figure 1
Time course of clinical arthritis index. (A) Body weight, (B) paw thickness, and (C) morphology score. Evaluations were made every 2 or 3 days. Morphology score was recorded using a 0 to 4 scale; for a maximum score of 16. Values are presented as mean ± standard error of mean.
ASA, aspirin; Clop, clopidogrel.
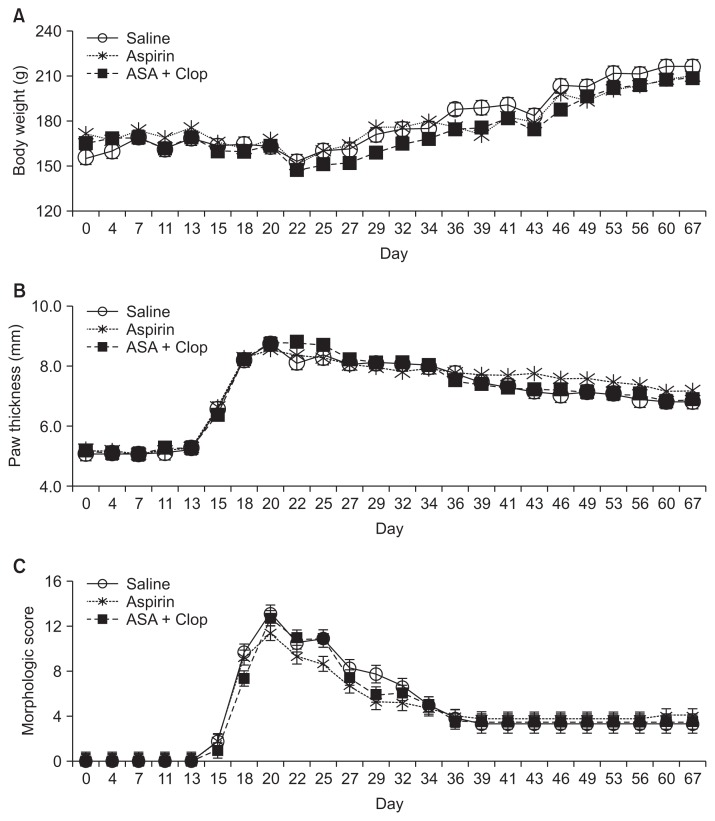
Figure 2Radiological score and X-ray image of Lewis rats with collagen-induced arthritis. (A) Radiological scores were assessed using a 0 to 3 scale in both hindlimbs: saline monotherapy group, aspirin monotherapy group, aspirin–clopidogrel dual therapy group. The scores were analyzed using analysis of variance to verify group differences on day 20, day 35, and day 70, respectively (*p < 0.05, **p < 0.01). (B) X-ray images on day 70: a) saline monotherapy group, b) aspirin monotherapy group, c) aspirin–clopidogrel dual therapy group. The hind paws and knee of the saline group showed more bone erosions (arrowheads) and osteophytes (arrows) than the aspirin monotherapy and aspirin–clopidogrel dual therapy groups.
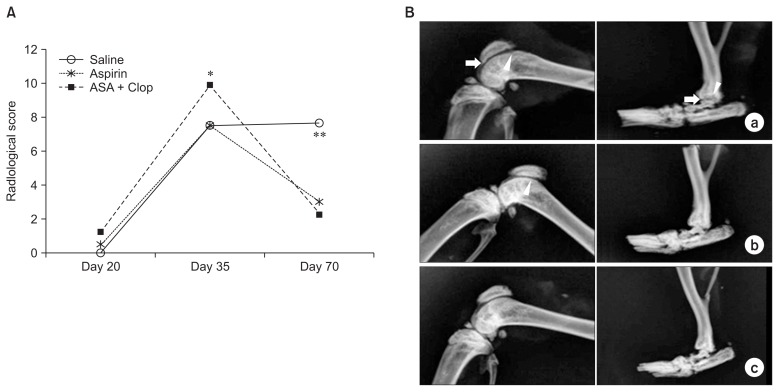
Table 1Changes in radiological scores of experimental groups over time
| Day 20 | Day 35 | Day 70 | p-value | F or χ2 | |
|---|---|---|---|---|---|
| Saline | 0 ± 0 | 7.50 ± 0.96 | 7.67 ± 1.69 | 0.002 | 12.871 |
| Aspirin | 0.50a ± 0.33 | 7.50b ± 0.82 | 3.00a ± 0.93 | 0.000 | 22.978 |
| Aspirin–clopidogrel | 1.25a ± 0.65 | 9.88b ± 0.40 | 2.25a ± 0.80 | 0.000 | 55.085 |
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader Cite
Cite

