Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 15(1); 2024 > Article
-
Original Article
Epidemiological analysis and prevention strategies in response to a shigellosis cluster outbreak: a retrospective case series in an alternative school in the Republic of Korea, 2023 -
Yeongseo Ahn1
 , Sunmi Jin2, Gemma Park1, Hye Young Lee1, Hyungyong Lee1, Eunkyung Shin3, Junyoung Kim3, Jaeil Yoo3, Yuna Kim1
, Sunmi Jin2, Gemma Park1, Hye Young Lee1, Hyungyong Lee1, Eunkyung Shin3, Junyoung Kim3, Jaeil Yoo3, Yuna Kim1 -
Osong Public Health and Research Perspectives 2024;15(1):68-76.
DOI: https://doi.org/10.24171/j.phrp.2023.0298
Published online: February 7, 2024
1Division of Infectious Disease Response, Chungcheong Reginal Center for Disease Control and Prevention, Daejeon, Republic of Korea
2Yuseong-gu Health Center, Daejeon, Republic of Korea
3Division of Bacterial Diseases, Bureau of Infectious Disease Diagnosis Control, Korea Disease Control and Prevention Agency, Cheongju, Republic of Korea
- Corresponding author: Yuna Kim Division of Infectious Disease Response, Chungcheong Reginal Center for Disease Control and Prevention, Union building 2nd floor, 48 Daedeok-daero 242beon-gil, Seo-gu, Daejeon 35233, Republic of Korea E-mail: yunaghim@korea.kr
- #Current affiliation: Nowon-gu Health Center, Seoul, Republic of Korea
© 2024 Korea Disease Control and Prevention Agency.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
- 982 Views
- 51 Download
Abstract
-
Objectives
- In March 2023, an alternative school in the Republic of Korea reported 12 cases of shigellosis. This study aims to analyze the epidemiological characteristics in order to determine the cause of the cluster outbreak of shigellosis and to develop prevention strategies.
-
Methods
- This study focused on 12 patients with confirmed Shigella infection and investigated their demographics, clinical features, epidemiology, diagnostics, and antimicrobial susceptibility. Following the identification of Shigella, we conducted follow-up rectal smear cultures to manage patients, implementing isolation and control measures.
-
Results
- This study investigated the emergence of multidrug-resistant Shigella following missionary activities in Cambodia, documenting a cluster infection within an alternative school in Daejeon, the Republic of Korea. The outbreak affected 56 participants, resulting in the confirmation of 12 cases. The incidence rates varied by gender and occupation, with higher rates among males and teachers. All 12 cases demonstrated multidrug resistance. Challenges included delayed pathogen confirmation and suboptimal adherence to isolation criteria. The incident prompted revisions in the criteria for isolation release, focusing on symptom resolution. The study underscores the necessity for strengthened surveillance, educational initiatives focusing on prevention in endemic areas, and improved oversight of unlicensed educational establishments.
-
Conclusion
- Successful response strategies included swift situation assessment, collaborative efforts, effective infection control measures, and modified criteria for isolation release. Continued surveillance of multidrug-resistant strains is recommended, especially in regions with a high prevalence.
- Shigella species are important pathogens that cause diarrhea and intestinal infections in developing and developed countries [1,2]. The World Health Organization (WHO) estimates that Shigella is responsible for at least 80 million cases of bloody diarrhea and contributes to approximately 7 million deaths worldwide each year [3]. In 2016, despite significant reductions in mortality over the past 3 decades, shigellosis was associated with roughly 212,438 deaths across all age groups, including about 60,000 fatalities among children under 5 years of age [4]. In the United States, 52 state and regional public health laboratories reported 12,597 cases of culture-confirmed Shigella spp. to the Laboratory-based Enteric Disease Surveillance system in 2016 [5]. In the Republic of Korea, the number of reported cases was 151 in 2019, decreased to 29 in 2020, then to 18 in 2021, increased to 31 in 2022, and stood at 17 by April 2023 [6]. Shigellosis is diagnosed through the isolation and identification of Shigella bacteria from stool or rectal swab samples. The primary symptoms of shigellosis vary and can include high fever, nausea, vomiting, crampy abdominal pain, and diarrhea, which may contain blood or mucus. In some cases, the infection may be asymptomatic. The typical incubation period for shigellosis is up to 14 days [1]. It is important to note that the cornerstone of shigellosis treatment is the maintenance of hydration and electrolyte balance [7]. Furthermore, the infection remains contagious until the bacteria are no longer present in the stool, which usually occurs within a few days to 4 weeks after symptoms begin. In rare instances, individuals can carry the bacteria for several months [1]. Among the various Shigella spp., Shigella sonnei is the most commonly isolated species in shigellosis cases in industrialized countries [8]. Over recent decades, it has also become increasingly prevalent throughout Southeast Asia [9].
- The rise of multidrug-resistant (MDR) strains within Enterobacteriaceae, notably Shigella, presents a significant threat to public health. This resistance compromises the efficacy of treatments, leading to longer durations of illness, increased healthcare costs, and higher mortality rates. Recent studies have highlighted the link between drug resistance and the lack of clustered regularly interspaced short palindromic repeats (CRISPRs) and CRISPR-associated (Cas) systems in Enterobacteriaceae, especially in the context of clinical infections [10,11]. In a tertiary hospital in the Republic of Korea, research focused on carbapenem-resistant Enterobacteriaceae and Acinetobacter baumannii (CRE/CRAB) [12]. Although community-acquired cases were relatively rare (6%), the study found that 20% of CRE/CRAB isolates were already present. The detection of carbapenem-resistant bacteria in domestic pets and their environments highlights the need to include these animals in One Health surveillance efforts to more effectively combat antimicrobial resistance [13]. Data on the response to overseas-imported shigellosis in alternative schools are limited. Therefore, the purpose of this study is to provide an epidemiological analysis of patients with overseas-imported shigellosis in an alternative school and to document their response status. The goal is to lay the groundwork for developing strategies to prevent the spread of shigellosis in future incidents.
Introduction
- Study Background and Settings
- On March 28, 2023, at 16:00, a medical institution in Daejeon, the Republic of Korea, reported a case of shigellosis, which was then recorded in the integrated disease control and prevention management system. Upon verification of the report, the public health office identified a student who had begun showing symptoms, including fever and diarrhea, on March 25, 2023. The student was subsequently subjected to a rectal swab test. Results from the test, conducted on March 28, 2023, detected the Shigella-specific gene (ipaH), confirming the diagnosis of Shigella infection in this individual.
- An epidemiological study was initiated by a local public health office. The investigation revealed that a student had engaged in mission work in Cambodia for 6 days, from March 20 to March 25, 2023. The student reported that several friends who also participated in the missionary activities exhibited symptoms such as fever and diarrhea. Notably, a friend who shared a room with the student had earlier experienced diarrhea and a high fever. In response to this cluster of symptomatic individuals suggestive of shigellosis, the local health department reported the situation to Daejeon and conducted an on-site epidemiological investigation on March 29, in collaboration with epidemiological investigation personnel from Daejeon City.
- The epidemiological investigation was coordinated by the Daejeon Metropolitan City Epidemiological Investigation Team and supported by the Chungcheong Reginal Center for Disease Control and Prevention. This collaboration also involved the local public health offices (4 in total), which were selected based on the patient's area of residence.
- The school under investigation was unlicensed and affiliated with an alternative religion, serving approximately 600 students and 100 staff members. It offered educational programs for elementary, middle, and high school levels. The middle school curriculum incorporated overseas missionary work. In March 2023, a group of 51 third-grade middle school students and 5 teachers from the school participated in a mission trip to Siem Reap, Cambodia, from March 20 to March 25. Following this trip, 12 individuals—10 students from the 3rd grade of middle school and 2 teachers—contracted Shigella.
- Epidemiological Investigation
- Individuals who engaged in missionary activities in Cambodia from March 20 to March 25, 2023, and subsequently displayed clinical symptoms indicative of shigellosis, with the presence of Shigella bacteria confirmed through the isolation and identification from their stool or rectal swab samples, were defined as cases.
- We attempted to estimate the source of infection through a cohort or case-control study. However, we faced limitations related to assessing food consumption during missionary activities in Cambodia due to the lack of dietary records, such as those for hotel breakfasts and group meals. Consequently, we opted to conduct a case series study of individuals who met the case definition.
- Patient information was collected through face-to-face interviews or telephone conversations using a shigellosis Epidemiological Investigation Form. The collected information included general characteristics, such as sex, age, place of residence, and occupation, and diagnostic and reporting-related data, such as the reporting classification and type of pathogen. The clinical symptom information collected included the date and time of initial symptom onset, symptoms and signs, medical facility visits, duration of illness, antibiotic treatment, and underlying diseases. Epidemiological data were obtained by investigating food consumption, international travel histories, and participation in group meals.
- Rectal swab culture tests were conducted for 16 types of bacteria, 5 types of viruses, and 4 types of parasites at the National Institute of Health and Environment. Students and school staff underwent rectal swab tests at public health centers near the school. Family members living in the same household were instructed to visit their local public health centers for the same tests. The samples were then sent to the local National Institute of Health and Environment for analysis. Additionally, Shigella isolates underwent confirmation, genotyping, and antimicrobial susceptibility testing at the Korea Disease Control and Prevention Agency (KDCA) to determine genetic relatedness among the pathogens. The identification of Shigella spp. isolates was performed using the VITEK 2 system (BioMerieux), and serotyping was carried out with commercial antisera kits (Denka Seiken) designed for all Shigella spp. serovars. Antimicrobial susceptibility testing for these isolates was conducted using the broth microdilution method with the Sensititre KRCDC2F custom panel (TREK Diagnostic Systems), following the Clinical and Laboratory Standards Institute guidelines. All isolates were analyzed by pulsed-field gel electrophoresis (PFGE) after XbaI digestion, in compliance with the PulseNet International protocol (https://pulsenetinternational.org/). The genetic relatedness among the PFGE patterns was assessed using BioNumerics ver. 7.6 (Applied Maths).
- Twelve patients diagnosed with shigellosis underwent both inpatient and outpatient treatments. Upon completion of their treatment, they were subjected to follow-up tests using rectal swab cultures at 24-hour intervals to confirm the absence of the bacteria. Furthermore, individuals in close contact with the patients, particularly family members residing in the same household, were identified as close contacts and also underwent rectal swab testing.
- Data Analysis
- Descriptive statistics, including frequency and percentage, were used to analyze the demographic and clinical characteristics of the cases gathered during the epidemiological investigation. All analyses were conducted using Microsoft Excel ver. 2013 (Microsoft Corp.)
- Ethics Approval
- The study protocol was approved by the Institutional Review Board of the KDCA (No: KDCA-2023-09-04-PE-01).
Materials and Methods
Case definition
Study design
Case Investigation
Laboratory Testing
Follow-Up Investigation
- On March 28, 2023, a healthcare facility reported a suspected case of shigellosis to the local health department. The following day, officials from the local health department and regional authorities carried out an epidemiological investigation at the site. This investigation uncovered that a group of 56 individuals, comprising 51 students and 5 teachers, had participated in missionary activities in Cambodia from March 20 to March 25, 2023. Beyond the initial reported case, multiple individuals exhibiting symptoms were also identified.
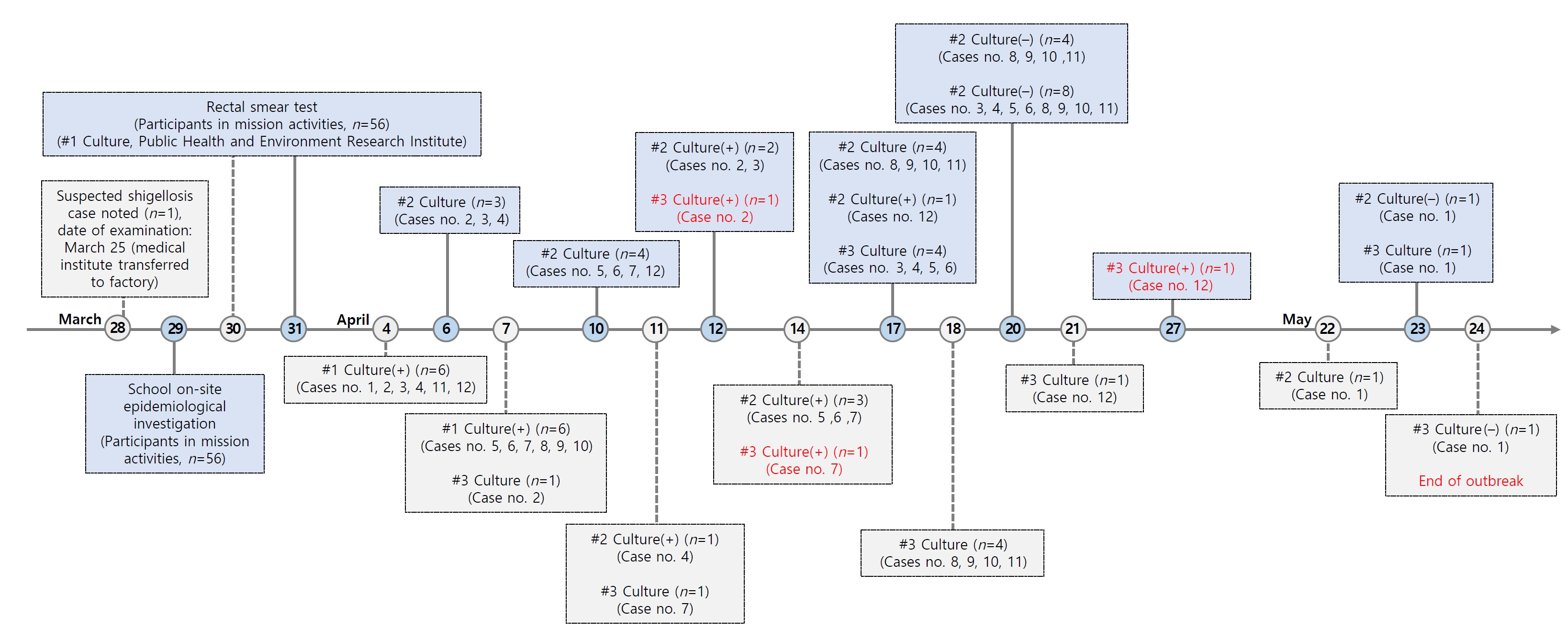
- In response to these findings, stool culture tests were administered on March 30 and 31, 2023, to 55 individuals who had participated in the missionary activities on both days, with the exception of the first case who had already tested positive via polymerase chain reaction (PCR). These individuals were also subjected to workplace swab tests. The National Institute of Environmental Research later reported that, of the 55 individuals tested, 11 were found to be positive for Shigella on March 31, 2023. On the same day, the local health department recommended that those who tested positive via PCR should self-isolate and highlighted the critical importance of maintaining personal hygiene. In addition, Shigella culture tests were performed on the close family members of the PCR-positive individuals, but only for those who had given verbal consent.
- Of the 12 PCR-positive individuals reported on March 31, 2023, the National Institute of Environmental Research confirmed that S. sonnei was cultured from 6 of them on April 4, 2023, and another 6 on April 7, 2023. These 12 individuals fell under the jurisdiction of 4 local health departments. Each department was notified of the positive S. sonnei culture results to effectively manage the cases. They were provided with guidance on patient management, which included isolating confirmed cases and conducting additional testing before releasing them from isolation. Of the 27 family members of patients with Shigella, 12 consented to participate in Shigella testing, all of whom tested negative. The remaining 15 individuals chose not to undergo testing; however, they were informed about the importance of personal hygiene.
- Of the 56 individuals in the study, who comprised 51 students and 5 teachers from an alternative school who participated in missionary activities in Cambodia over a period of 6 days from March 20 to March 25, 2023, 12 tested positive for Shigella on culture examinations. When examining demographic characteristics, the incidence rate was higher in males (25.8%; 8 out of 31) than in females (16.0%; 4 out of 25). Furthermore, the incidence rate among teachers was significantly higher (40.0%; 2 out of 5) than among students (19.6%; 10 out of 51) (Table 1).
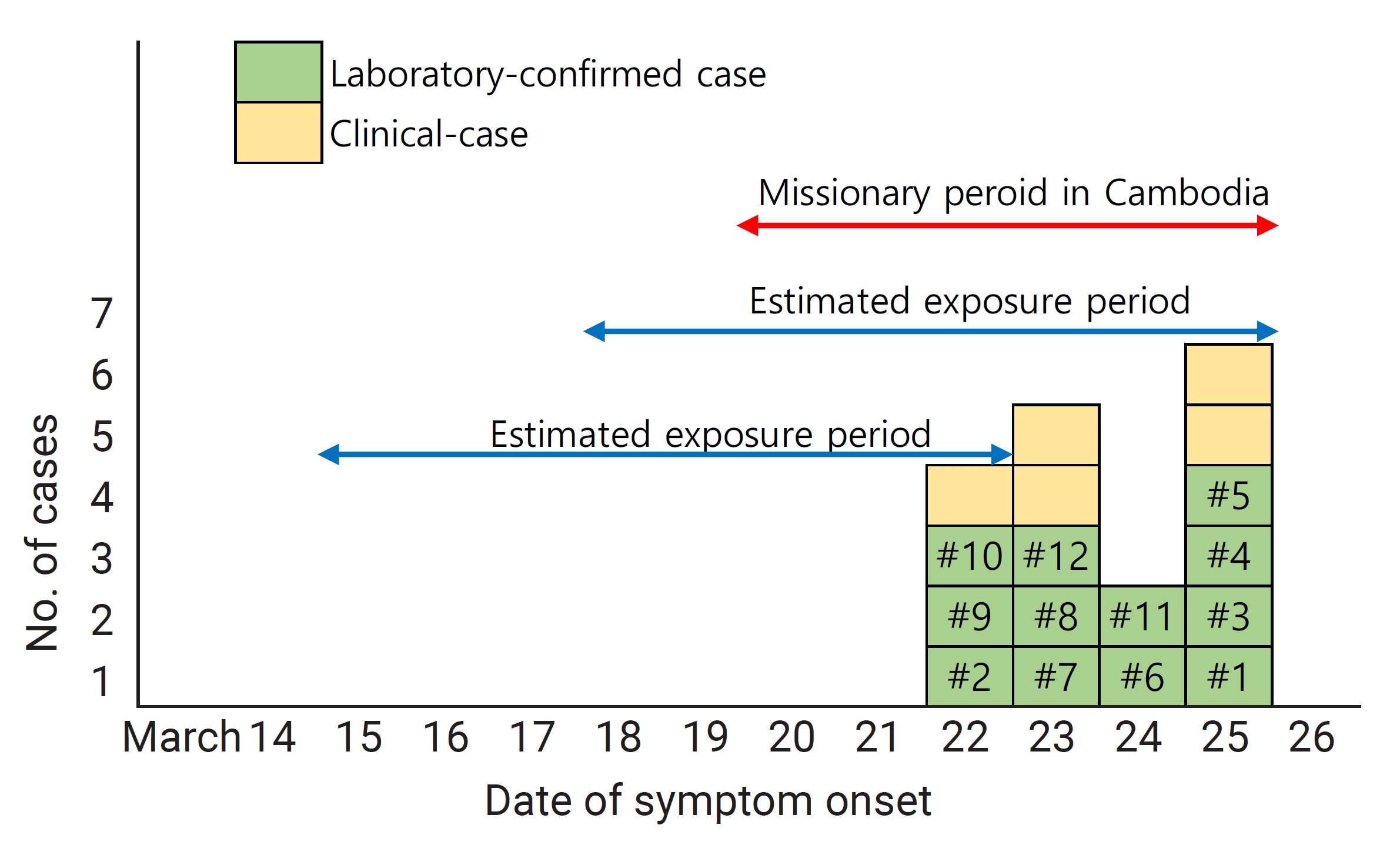
- The epidemiological analysis of shigellosis cases indicated that the onset of symptoms occurred on March 22, 23, 24, and 25, 2023, affecting 3, 3, 2, and 4 individuals, respectively. Taking into account the known incubation period for Shigella, which ranges from 12 hours to 7 days, we determined that the likely exposure period corresponded with missionary activities in Cambodia, as shown in Figure 1. Students and teachers participated in missionary activities in Siem Reap, Cambodia, from March 20 to 25, 2023. Individual bottled containers were provided for drinking water. The hotel’s menus, as reported by school officials, included kimchi stew, braised ribs, pork, beef, miso, army stew, morning glory stir-fry, and a variety of tropical fruits such as mango, longan, watermelon, papaya, and pineapple. However, the accuracy of an individual’s dietary information is dependent on memory and cannot be precisely determined. All 12 individuals who tested positive for Shigella in the culture examination experienced symptoms of diarrhea, with the number of episodes ranging from 3 to 10. The most common accompanying symptoms were abdominal pain, reported in 9 cases, fever in 6, and headaches in 5 (Table 2).
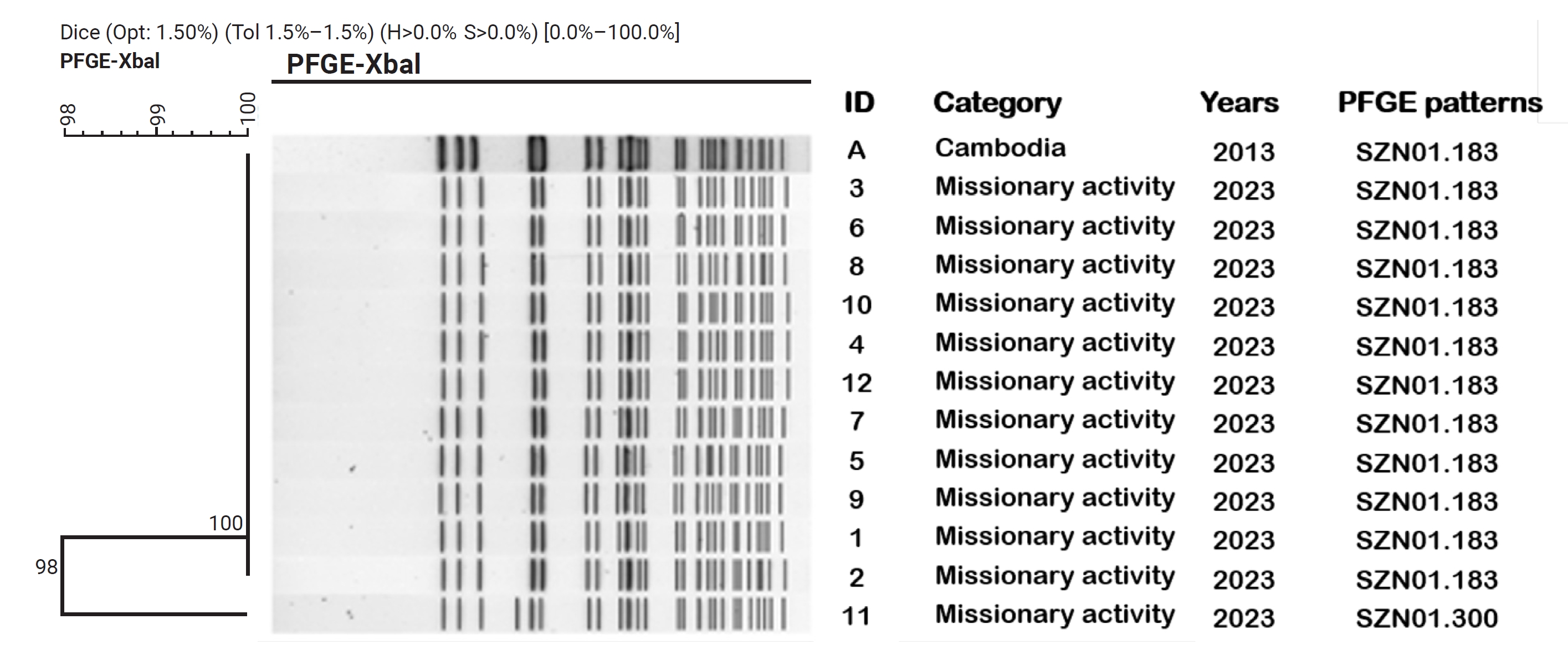
- In the patient isolate analysis, 2 PFGE patterns were detected using the XbaI restriction enzyme. These patterns were identified as SZNX01.183, which displayed 11 bands, and SZNX01.300, which consisted of a single band. The genetic relatedness between these 2 patterns was found to be 97.98%. Antibiotic susceptibility testing indicated that the Shigella strains were resistant to multiple antibiotics, including ampicillin, and exhibited a MDR phenotype, showing resistance to 7 or 8 different antibiotics (Table 2). According to the PulseNet database for domestic S. sonnei, the SZNX01.183 pattern with 11 bands has been previously identified in Shigella strains that were introduced from foreign countries, including India, Cambodia, and Vietnam, between the years 2012 and 2014 (Figure 2).
- The epidemiological investigation conducted in this study successfully isolated Shigella from the stool samples of 12 individuals. Serogroup D of S. sonnei was identified and confirmed as the causative pathogen. Although the duration of the individuals’ stay in Cambodia coincided with the incubation period of Shigella (Figure 1), the lack of sufficient evidence from food consumption and environmental investigations precluded the determination of the precise source of infection.
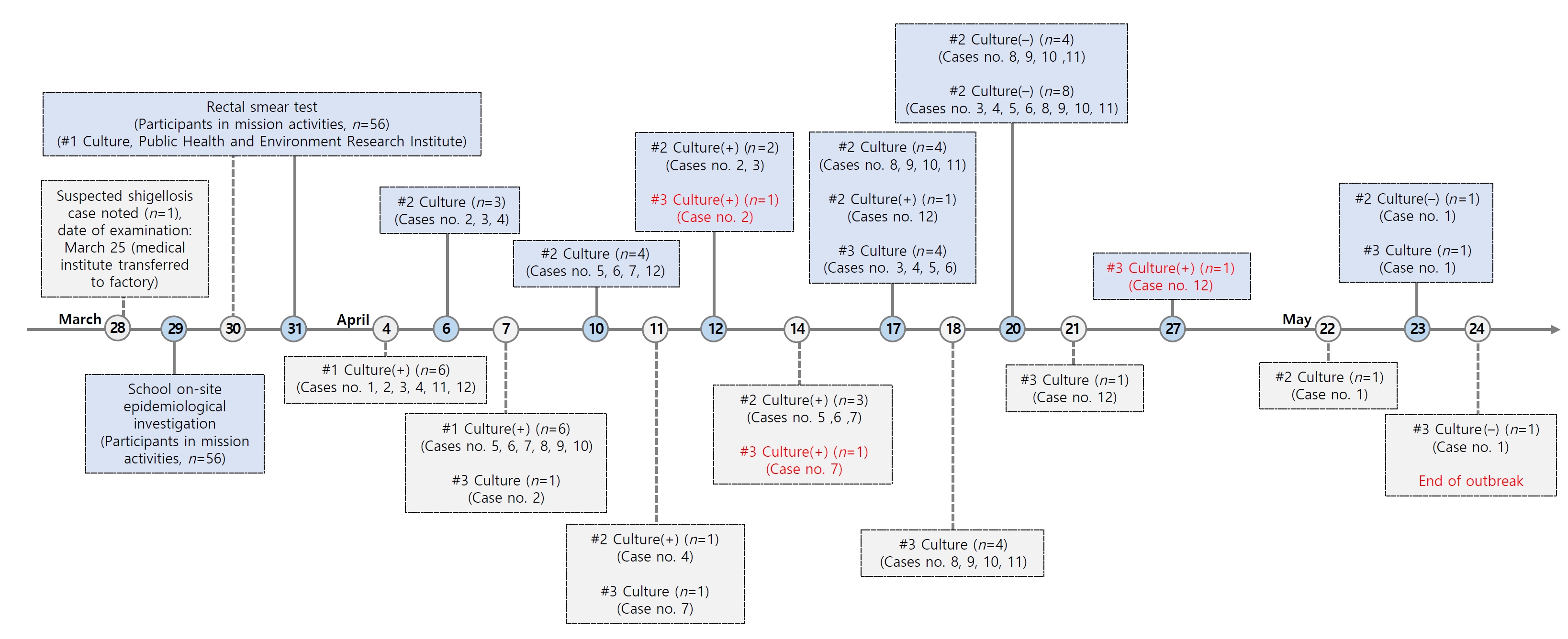
- Shigella-positive individuals were monitored, and subsequent second and third culture tests were conducted to determine when they could be released from isolation. Following the confirmation of negative results, there were no further cases of shigellosis reported as of May 24, 2023, marking the end of the outbreak (Figure 3).
Results
- Shigellosis, also known as bacillary dysentery, is officially recognized as a notifiable infectious disease under the Communicable Disease Prevention Act enforced by the KDCA. It falls under the management framework of Class 2 infectious diseases according to legal regulations. The KDCA reports that the incidence of shigellosis in the Republic of Korea has decreased since the 1950s, following the introduction of antibiotics and advancements in environmental hygiene. During the global coronavirus disease 2019 (COVID-19) pandemic, from 2020 to 2022, there was a notable decline in cases of shigellosis acquired overseas in the Republic of Korea. The recorded cases for these years were 29 in 2020, 18 in 2021, and 31 in 2022 [14]. This trend aligns with the observed decrease in gastrointestinal infections during the COVID-19 pandemic in the United Kingdom [15].
- Shigellosis can cause a wide range of clinical symptoms, ranging from asymptomatic cases to mild or severe illness, which may include dehydration and bloody diarrhea [1]. In the outbreak described, all patients exhibited the typical symptom of watery diarrhea, while other symptoms such as fever, nausea, and vomiting differed among individuals. These observations align with the symptomatology reported in prior research on shigellosis [16].
- All 12 cases of S. sonnei identified in this study were found to be MDR strains, showing resistance to 7 or 8 different antibiotics based on antibiotic susceptibility analysis. S. sonnei is globally distributed and is the most common causative agent of shigellosis in industrialized regions, such as Europe, North America, and Australia. It is currently expanding to middle-income countries across Asia, Latin America, and the Middle East [17]. In acute pediatric diarrheal samples collected in Tehran, S. sonnei was detected in 40 out of 75 Shigella spp. cases [18].
- S. sonnei has demonstrated MDR to sulfonamides, ampicillin, streptomycin, and tetracycline since the 1960s, which suggests the presence of a variety of antimicrobial resistance genes [1,2]. As a result, the use of fluoroquinolones, especially ciprofloxacin, increased for treating drug-resistant shigellosis, and their use became the standard practice after the WHO endorsed them in 2005. However, the extensive use of fluoroquinolones, including ciprofloxacin, has led to the emergence of antibiotic resistance. By the late 1990s, ciprofloxacin-resistant S. sonnei had appeared and begun to spread across Asia [19–22]. For instance, between 2014 and 2019, 98% of Shigella isolates collected in Cambodia were found to be MDR [23].
- Based on results from the PulseNet database of the KDCA, the S. sonnei strain implicated in the recent outbreak, identified as SZNX01.183, was found to match the type associated with overseas shigellosis cases imported from India, Cambodia, and Vietnam between 2012 and 2014. Consequently, it can be inferred that the shigellosis outbreak in this instance was linked to exposure incurred during missionary activities in Cambodia.
- In this outbreak, it took some time to confirm that the gastrointestinal infection with symptoms of diarrhea was caused by MDR Shigella. Consequently, individuals who sought medical care before the test results were available received appropriate treatment. This could include antibiotics or symptomatic treatment, depending on the severity of their symptoms, in accordance with the travelers’ diarrhea treatment guidelines [24]. However, a significant amount of time was required for individuals to meet the isolation release criteria, which necessitated 2 negative culture test results without the use of antibiotics. Despite the resolution of symptoms, some teachers remained unable to return to work, and students were not able to fully participate in classes, leading to less than optimal adherence to infection management. This outbreak prompted a reassessment of the need to reconsider the shigellosis isolation release criteria in the Republic of Korea. As a result, the KDCA revised the isolation release criteria to consider both the presence or absence of symptoms and laboratory test results.
- The school involved in the recent shigellosis outbreak operated as an alternative educational institution. It was not subject to the School Health Act, functioning as an unlicensed educational facility outside the regulatory oversight of both the Ministry of Education and the provincial Office of Education. This situation has brought to light the problem of ambiguous authority over the management and supervision of such institutions. In a similar case from January 2021, an unlicensed residential educational facility run by a missionary group became the center of a COVID-19 cluster infection [25,26]. This incident further underscored the need for better regulation of unlicensed educational organizations. Previous research suggests that a practical approach might include the classification and mandatory reporting of various types of unlicensed educational facilities to protect students. Additionally, creating legal frameworks to govern and administer these reported institutions could be an effective solution [27].
- The implementation of immediate school restrictions, self-isolation, and infection control measures, such as hand hygiene, upon confirmation of test results during the shigellosis outbreak, was effective in preventing further spread. These measures are consistent with non-pharmaceutical interventions that have been previously employed in the management of patients with shigellosis [28].
- Prior research has demonstrated a widespread prevalence of MDR Shigella strains in Southeast Asia, underscoring the need for improved surveillance to control the spread of antibiotic resistance. This is particularly important given the potential for overseas travel to contribute to this issue [16,29].
- Recent updates have been made to the criteria for releasing shigellosis patients from isolation, which are now based on the resolution of symptoms. Further research is needed to evaluate the awareness and acceptance of these revised guidelines among infection control personnel.
Discussion
- The successful response to the outbreak of MDR Shigella imported from Cambodia was facilitated by a rapid assessment of the situation and cooperative efforts between local communities and pertinent agencies. It is crucial to maintain timely communication with these agencies to prevent the spread of infection domestically after it is introduced from abroad. Furthermore, it is important to focus on improving patient adherence to infection control practices in various environments, including schools, family households, and local communities.
- Additionally, individuals visiting regions where shigellosis is endemic should receive education on preventive strategies, including practicing proper hand hygiene, ensuring access to clean drinking water, and adopting safe food consumption practices.
Conclusion
- • In March 2023, a shigellosis outbreak affected 12 individuals at an alternative school in the Republic of Korea.
- • This study aimed to analyze and prevent cluster outbreaks.
- • Shigella cases were confirmed in 21.4% of individuals engaged in missionary activities in Cambodia, all of whom presented with diarrhea.
- • The strains exhibited multidrug resistance.
- • Rapid identification, on-site investigations, and strict hygiene measures halted the epidemic without further local transmission.
- • Swift situational awareness and responses are crucial for interrupting transmission and preventing the spread of Shigella.
- • Collective efforts from schools, families, and communities can improve patient compliance with infection control measures.
HIGHLIGHTS
-
Ethics Approval
The collection of data in accordance with Article 18 of the infectious Disease Control and Prevention Act was approved by the Institutional Review Board of the KDCA (KDCA: 2023-09-04-PE-01).
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Availability of Data
The datasets are not publicly available, but are available from the corresponding author upon reasonable request.
-
Authors’ Contributions
Conceptualization: all authors; Data curation: YA, JP; Formal analysis: SJ, ES, JK, JY; Investigation: SJ, YA, JP, HL, HL; Methodology: YA, JP, HL, HL; Project administration: YAG; Resources: SJ; Supervision: YAG; Visualization: YA; Writing–original draft: YA; Writing–review & editing: all authors. All authors read and approved the final manuscript.
-
Additional Contributions
We thank our colleagues in the related province and the public health center for their contribution to data and sample collection and also thank Editage (www.editage.co.kr) for English language editing.
Article information

| Variable | Total (n) | Shigella sonnei case (n) | Attack rate (%) |
|---|---|---|---|
| Total | 56 | 12 | 21.4 |
| Sex | |||
| Male | 31 | 8 | 25.8 |
| Female | 25 | 4 | 16.0 |
| Identity | |||
| Teacher | 5 | 2 | 40.0 |
| Student | 51 | 10 | 19.6 |
| Characteristic |
Case no. |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
| Sex | Female | Male | Female | Male | Male | Male | Female | Male | Female | Male | Male | Male |
| Occupation | Teacher | Teacher | Student | Student | Student | Student | Student | Student | Student | Student | Student | Student |
| Symptoms | ||||||||||||
| Fever | N | N | Y | Y | N | Y | N | N | Y | Y | Y | N |
| Nausea | Y | N | N | Y | N | N | N | N | N | N | Y | N |
| Vomiting | Y | N | N | Y | N | N | N | N | Y | N | Y | N |
| Watery diarrheaa) | Y6 | Y5 | Y10 | Y8 | Y4 | Y8 | Y5 | Y8 | Y6 | Y5 | Y4 | Y3 |
| Muscle pain | Y | N | Y | Y | N | N | N | N | N | N | N | N |
| Headache | Y | N | N | N | Y | N | Y | Y | N | N | N | N |
| Stomachache | Y | Y | Y | N | N | N | N | Y | Y | Y | Y | Y |
| Dehydration | Y | N | N | N | N | N | N | N | N | N | N | N |
| Types of bacteria | S. sonnei | S. sonnei | S. sonnei | S. sonnei | S. sonnei | S. sonnei | S. sonnei | S. sonnei | S. sonnei | S. sonnei | S. sonnei | S. sonnei |
| Serotype | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ | D, phase Ⅱ |
| PFGE type | SZNX01.183 | SZNX01.183 | SZNX01.183 | SZNX01.183 | SZNX01.183 | SZNX01.183 | SZNX01.183 | SZNX01.183 | SZNX01.183 | SZNX01.183 | SZNX01.300 | SZNX01.183 |
| Antimicrobial susceptibility | ||||||||||||
| Ampicillin | R | R | R | R | R | R | R | R | R | R | R | R |
| Azithromycin | R | R | R | R | R | R | R | R | R | R | R | R |
| Cefotaxime | R | R | R | R | R | R | R | R | R | R | R | R |
| Ceftriaxone | R | R | R | R | R | R | R | R | R | R | R | R |
| Ciprofloxacin | R | R | R | R | R | R | R | R | R | R | R | R |
| Nalidixic acid | R | R | R | R | R | R | R | R | R | R | R | R |
| Tetracycline | R | R | R | S | R | S | R | R | R | R | S | R |
| Trimethoprim/sulfamethoxazole | R | R | R | R | R | R | R | R | R | R | R | R |
- 1. Niyogi SK. Shigellosis. J Microbiol 2005;43:133−43.PubMed
- 2. Kotloff KL, Riddle MS, Platts-Mills JA, et al. Shigellosis. Lancet 2018;391:801−12.ArticlePubMed
- 3. World Health Organization (WHO). Guidelines for the control of shigellosis epidemics due to Shigella dysenteriae type I. WHO; 2005.
- 4. Khalil IA, Troeger C, Blacker BF, et al. Morbidity and mortality due to shigella and enterotoxigenic Escherichia coli diarrhoea: the Global Burden of Disease Study 1990-2016. Lancet Infect Dis 2018;18:1229−40.ArticlePubMedPMC
- 5. Center for Disease Control and Prevention (CDC). National enteric disease surveillance: shigella annual report, 2016 [Internet]. National Center for Emerging and Zoonotic Infectious Diseases, CDC; 2018 [cited 2023 May 12]. Available from: https://www.cdc.gov/nationalsurveillance/pdfs/LEDS-Shig-2016-REPORT-508.pdf.
- 6. Korea Disease Control and Prevention Agency (KDCA). Infectious disease portal [Internet]. KDCA; 2023 [cited 2023 Oct 11]. Available from: https://dportal.kdca.go.kr/pot/ii/sttyInftnsds/sttyInftnsds.do.
- 7. Victora CG, Bryce J, Fontaine O, et al. Reducing deaths from diarrhoea through oral rehydration therapy. Bull World Health Organ 2000;78:1246−55.PubMedPMC
- 8. Gupta A, Polyak CS, Bishop RD, et al. Laboratory-confirmed shigellosis in the United States, 1989-2002: epidemiologic trends and patterns. Clin Infect Dis 2004;38:1372−7.ArticlePubMed
- 9. Vinh H, Nhu NT, Nga TV, et al. A changing picture of shigellosis in southern Vietnam: shifting species dominance, antimicrobial susceptibility and clinical presentation. BMC Infect Dis 2009;9:204. ArticlePubMedPMCPDF
- 10. Alduhaidhawi AH, AlHuchaimi SN, Al-Mayah TA, et al. Prevalence of CRISPR-Cas systems and their possible association with antibiotic resistance in Enterococcus faecalis and Enterococcus faecium collected from hospital wastewater. Infect Drug Resist 2022;15:1143−54.ArticlePubMedPMCPDF
- 11. Jwair NA, Al-Ouqaili MT, Al-Marzooq F. Inverse association between the existence of CRISPR/Cas systems with antibiotic resistance, extended spectrum β-lactamase and carbapenemase production in multidrug, extensive drug and pandrug-resistant Klebsiella pneumoniae. Antibiotics (Basel) 2023;12:980. ArticlePubMedPMC
- 12. Kang S, Jeong IS. Epidemiological characteristics of carbapenem-resistant Enterobacteriaceae and carbapenem-resistant Acinetobacter baumannii in a tertiary referral hospital in Korea. Osong Public Health Res Perspect 2022;13:221−9.ArticlePubMedPMCPDF
- 13. Rincon-Real AA, Suarez-Alfonso MC. Carbapenem resistance in critically important human pathogens isolated from companion animals: a systematic literature review. Osong Public Health Res Perspect 2022;13:407−23.ArticlePubMedPMCPDF
- 14. Korea Disease Control and Prevention Agency (KDCA). Infectious diseases surveillance yearbook, 2022. KDCA; 2023. Korean.
- 15. Love NK, Elliot AJ, Chalmers RM, et al. Impact of the COVID-19 pandemic on gastrointestinal infection trends in England, February-July 2020. BMJ Open 2022;12:e050469.ArticlePubMed
- 16. Muzembo BA, Kitahara K, Mitra D, et al. Burden of Shigella in South Asia: a systematic review and meta-analysis. J Travel Med 2023;30:taac132. ArticlePubMedPDF
- 17. Torraca V, Holt K, Mostowy S. Shigella sonnei. Trends Microbiol 2020;28:696−7.ArticlePubMedPMC
- 18. Yaghoubi S, Ranjbar R, Dallal MM, et al. Profiling of virulence-associated factors in Shigella species isolated from acute pediatric diarrheal samples in Tehran, Iran. Osong Public Health Res Perspect 2017;8:220−6.ArticlePubMedPMC
- 19. Chung H, Baker S. Out of Asia: the independent rise and global spread of fluoroquinolone-resistant Shigella. Microb Genom 2018;4:e000171.PubMedPMC
- 20. Al-Qaysi AK, Al-Ouqaili MT, Al-Maeani SA. Effect of pyocyanin as secondary metabolite on pseudomonal biofilm and in increasing the resistance degree to antipseudomonal agents. Drug Invent Today 2020;14:864−9.
- 21. Al-Ouqaili MT. Identification of an OprD and blaIMP gene-mediated carbapenem resistance in Acinetobacter baumannii and Pseudomonas aeruginosa among patients with wound infections in Iraq. Asian J Pharm 2018;12.
- 22. Chinemerem Nwobodo D, Ugwu MC, Oliseloke Anie C, et al. Antibiotic resistance: the challenges and some emerging strategies for tackling a global menace. J Clin Lab Anal 2022;36:e24655.PubMedPMC
- 23. Poramathikul K, Wojnarski M, Sok S, et al. Update on Shigella and nontyphoidal salmonella antimicrobial drug resistance: implications on empirical treatment of acute infectious diarrhea in Cambodia. Antimicrob Agents Chemother 2021;65:e0067121.ArticlePubMedPDF
- 24. Riddle MS, Connor BA, Beeching NJ, et al. Guidelines for the prevention and treatment of travelers' diarrhea: a graded expert panel report. J Travel Med 2017;24(suppl 1). S63−80.Article
- 25. Kim DS. More than 30 unaccredited alternative schools in Gwangju... Corona epidemic “blind spot” [Internet]. Gwangju Daily Report; 2021 [cited 2023 Oct 11]. Available from: http://www.kwangju.co.kr/read.php3?aid=1611656400713460006. Korean.
- 26. Jeon HJ. Police seize and search IM Mission Church in Daejeon for COVID-19 outbreak [Internet]. Kookmin Daily Report. 2021 [cited 2023 Oct 11]. Available from: http://news.kmib.co.kr/article/view.asp?arcid=0015534276&code=61121111&cp=nv. Korean.
- 27. Shin KS. A study on the authority of managing the unapproved educational facilities: focused on the missionary schools and Confucian schools. Kangwon Law Rev 2021;64:107−40. Korean.Article
- 28. Park S, Michelow IC, Choe YJ. Trend of gastrointestinal infections following nonpharmaceutical interventions, South Korea, 2020. J Infect Dis 2021;224:368−71.ArticlePubMedPDF
- 29. Puzari M, Sharma M, Chetia P. Emergence of antibiotic resistant Shigella species: a matter of concern. J Infect Public Health 2018;11:451−4.ArticlePubMed
 Cite
Cite