Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 14(4); 2023 > Article
-
Original Article
Effects of an arteriovenous fistula stenosis prevention program in patients receiving hemodialysis -
Haegyeong Lee1
 , Gyuli Baek1, Eunju Lee2
, Gyuli Baek1, Eunju Lee2 -
Osong Public Health and Research Perspectives 2023;14(4):279-290.
DOI: https://doi.org/10.24171/j.phrp.2023.0101
Published online: August 9, 2023
1Keimyung University Graduate School, Daegu, Republic of Korea
2College of Nursing, Keimyung University, Daegu, Republic of Korea
- Corresponding author: Eunju Lee College of Nursing, Keimyung University, 1095 Dalgubeol-daero, Dalseo-gu, Daegu 42601, Republic of Korea E-mail: vinuslee76@gmail.com
© 2023 Korea Disease Control and Prevention Agency.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
- 1,261 Views
- 143 Download
Abstract
-
Objectives
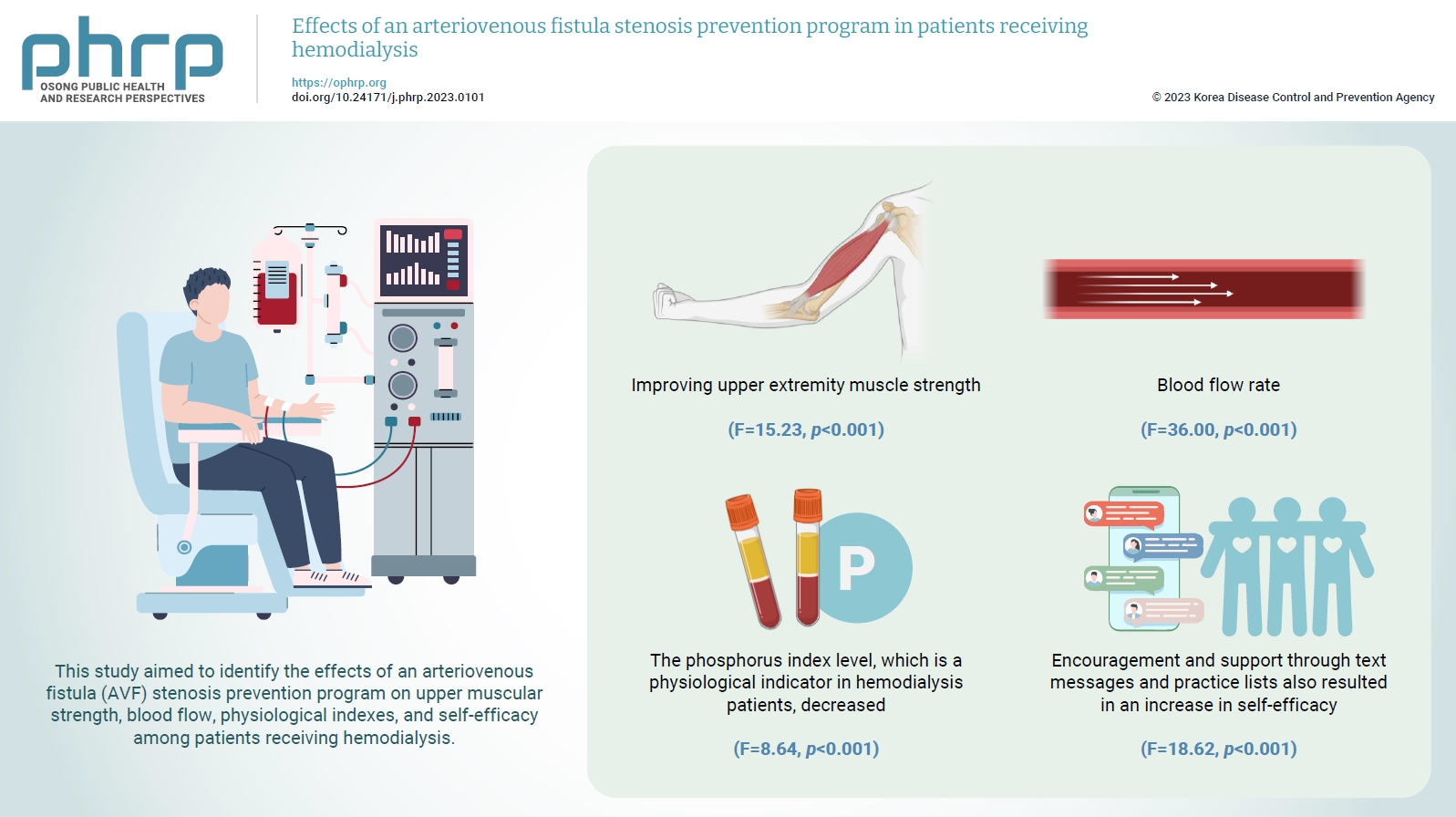
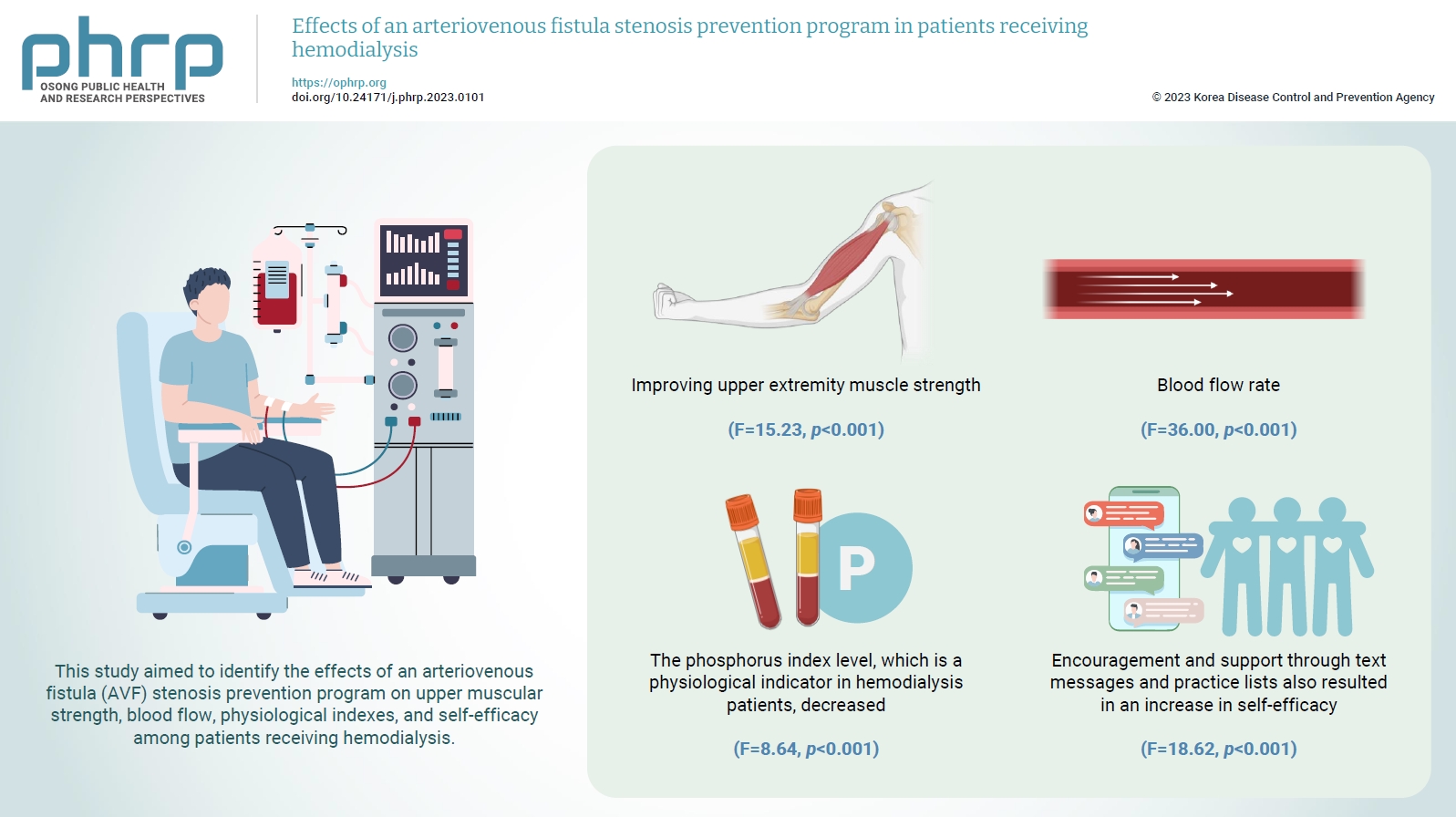
- To increase the efficiency of hemodialysis, an appropriate vascular pathway must be created, and its function must be maintained. This study aimed to identify the effects of an arteriovenous fistula (AVF) stenosis prevention program on upper muscular strength, blood flow, physiological indexes, and self-efficacy among patients receiving hemodialysis.
-
Methods
- The participants were patients receiving hemodialysis at Keimyung University Dongsan Medical Center in Daegu, Republic of Korea. They were divided into experimental and control groups based on the day of the week they received hemodialysis at the outpatient department and included 25 participants each. The study was conducted for 8 weeks.
-
Results
- The AVF stenosis prevention program was effective in improving upper extremity muscle strength (F=15.23, p<0.001) and blood flow rate (F=36.00, p<0.001). As a result of the program, the phosphorus index level, which is a physiological indicator in hemodialysis patients, decreased (F=8.64, p<0.001). Encouragement and support through text messages and practice lists also resulted in an increase in self-efficacy (F=18.62, p<0.001).
-
Conclusion
- The AVF stenosis prevention program in this study resulted in an increase in upper extremity muscle strength through grip strength exercises and was effective in preventing AVF stenosis by increasing the blood flow rate.
- Chronic kidney disease (CKD) affects more than 10% of the global population [1,2]. The worldwide prevalence of CKD in 2017 was 9.1% and has increased by 29.3% since 1990 [3]. According to the Centers for Disease Control, 15% of adults in the United States have CKD [4], and approximately 80% receive hemodialysis [5], which removes uremic substances from the blood by adsorption using convection and diffusion dialysis membranes with a semipermeable membrane as a boundary [6]. Long-term hemodialysis requires an arteriovenous fistula (AVF) that can withstand repeated punctures and maintain a blood flow rate of 600 mL/min or more [2].
- However, complications related to vascular access in patients receiving hemodialysis increase with the dialysis period. The incidence of AVF stenosis is 16% to 28% within 1 year and 26% to 36% within 2 years [7]. Approximately 30% of cases are caused by the failure of vascular maturation due to a lack of overall AVF management, interventions due to early loss of function, and reoperations [8]. Vascular access complications, including AVF, are responsible for numerous hospitalizations and substantial medical expenses in patients receiving hemodialysis [9]. Nonetheless, the rate of noncompliance concerning self-management in patients receiving hemodialysis may be as high as 50% [10,11].
- To prevent AVF stenosis and occlusion, exercise therapy to improve upper extremity muscle strength and maintain the patency of blood vessels and a diet that helps prevent blood clots are crucial [12,13]. The upper extremity muscle strength of patients receiving hemodialysis is extremely weak, and patients’ mean physical performance is significantly lower than that of healthy adults by an average of 50% [11,14]. Gradual strength exercise improves patients’ upper extremity muscle strength [15], arteriosclerosis, blood pressure, and the blood flow rate, resulting in structural and functional changes in blood vessels [9,14]. Vascular calcification, which causes AVF stenosis, is common in these patients, with risk factors including sex, age, underlying disease, dialysis period, AVF type, and blood calcium and phosphorus levels [16]. Vascular calcification can be controlled by maintaining stable levels of calcium and phosphorus in the blood through dialysis while also incorporating exercise therapy and a healthy diet [17,18]. Education combined with exercise and diet increases the size and blood flow of AVFs and prevents hyperphosphatemia [11,15,17]. However, there are few studies on programs that combine exercise therapy and diet to prevent AVF stenosis.
- In patients receiving hemodialysis, active self-management including strict water restriction, diet, medication, and vascular channel management is essential for minimizing discomfort and complications related to renal dysfunction [11,15]. Self-efficacy refers to an individual’s belief in their ability to practice certain behaviors under certain situations, and its promotion induces behavioral changes by increasing trust in treatment and confidence in health promotion behaviors [19]. Therefore, patients should understand AVF management, treatment procedures, and their role in treatment procedures, and programs should be conducted to enhance their perceived self-efficacy [20].
- In previous studies on exercise therapy for dialysis patients, simple repetitive motion exercises using rubber balls [15,21], rubber bands [22], and grippers [23] were predominant. However, muscle exercise using a gripper is more effective in increasing the venous size and blood flow of an AVF than simple repetitive training using a rubber ball with low elasticity [24]. Kim and Choi [18] also conducted a survey on a phosphorus-restricted diet and related patient knowledge and self-monitoring of one’s eating habits using a journal; their intervention also involved diet education and counseling to demonstrate the effects of calcium and phosphorus levels.
- Therefore, this study conducted a complex program combining the strengthening of upper extremity muscles through progressive exercise therapy using a gripper and a phosphorus-restricted diet to prevent vascular calcification, evaluated changes in physiological indicators of vascular calcification in patients receiving hemodialysis, and investigated the effect on blood flow velocity, which is a clinical indicator of stenosis. Additionally, patients receiving hemodialysis received health education using videos and informational magazines for vascular self-care, health counseling using AVF self-management practice checklists, and text messages to encourage active participation in various programs. This study investigated the effects of the program on AVF stenosis and self-efficacy.
Introduction
- Study Design
- This study used a non-equivalent control group pretest-posttest design to develop a nursing intervention program for AVF management and verify its effectiveness. The study design is illustrated in Table 1.
- Participants
- The participants included 50 outpatients receiving hemodialysis at Keimyung University Dongsan Medical Center in Daegu, Republic of Korea, from December 15, 2016, to February 5, 2017. Convenience sampling was used. To prevent the spread and contamination of the experimental effect, 25 dialysis patients on Mondays, Wednesdays, and Fridays were selected as the experimental group, and 25 dialysis patients on Tuesdays, Thursdays, and Saturdays were selected as the control group. The specific selection criteria were as follows: (1) those aged from 20 to 75 years who had undergone hemodialysis through an AVF 3 times a week for more than 6 months; (2) those with no history of mental illness; (3) those who understand the content of the AVF stenosis prevention program and could verbally communicate; and (4) those with a blood flow rate of 600 mL/min or more [25].
- The sample size for this study was calculated using G*Power 3.1 (Heinrich-Heine-Universität Düsseldorf), and the number of participants was based on a previous study involving an intervention program for patients receiving hemodialysis [25,26]. Based on a significance level of 0.05, median effect size of 0.35, and power of 0.80 for 2 groups with 3 measurements, the required sample size was at least 46. Considering a possible dropout rate of 10%, 50 participants were recruited, with 25 each in the experimental and control groups. No participants dropped out during the study [27].
- Measurements
- The participants’ general characteristics comprised 7 items: sex, age, marital status, family type, education, occupation, and economic status. Eleven disease-related characteristics were collected: dialysis period, causative disease, current body weight, weight gain after dialysis, heparin usage during dialysis, maturation period after AVF surgery, vascular occlusion experience, current location of AVF, current AVF use period, smoking status, and current medications.
- Upper extremity muscle strength was measured using a digital dynamometer (KH-100; Gyeongin Industrial Co.), which was held such that the second joint of the finger formed a right angle. The participant then lowered the arm naturally to ensure that the dynamometer did not touch the torso or lower body. A higher grip strength score indicated better upper extremity muscle strength.
- After exchanging the position of the arterial and venous conduits with the value measured using the ultrasound dilution method, the speed of the dialyzer was maintained at 200 to 250 mL/min, and temporary recirculation was induced. After injecting 10 mL of normal saline, the measured value was recorded using an ultrasound machine. The normal blood flow rate range is more than 600 mL/min, and rates below that threshold indicate the progression of AVF stenosis [25].
- Blood tests for calcium and phosphorus, which are risk factors for vascular calcification, were performed at the Department of Diagnostic Laboratory Medicine after collecting 5 mL of blood from a plain tube after 12 hours of fasting immediately before starting hemodialysis. Blood calcium and phosphorus levels were measured using the results of routine monthly testing performed in a hemodialysis room. In patients receiving hemodialysis, the normal range for serum calcium is 8.5 to 10.2 mg/dL, and it is 3.5 to 5.5 mg/dL for serum phosphorus [18].
- The self-efficacy tool developed by Kim and Kim [28] for patients receiving hemodialysis was modified and supplemented by Choi and Lee [29] to create the 10-item measurement tool used in this study. Each item is scored on a 4-point scale with 4 points for “strongly agree,” 3 points for “somewhat agree,” 2 points for “not very much,” and 1 point for “hardly ever.” Higher scores indicate higher self-efficacy. At the time of the tool’s development, the tool had a Cronbach’s α of 0.81 [28], and it was 0.73 in the study by Choi and Lee [29] and 0.71 in this study.
- Data Collection
- The data were collected from outpatients receiving hemodialysis in the artificial kidney room of Keimyung University Dongsan Medical Center. The purpose and methods of this study were explained to the professor of nephrology and the head nurse in the artificial kidney room, and consent was obtained before proceeding with the study. Gift certificates were given to the study subjects as a gesture of appreciation.
- Procedure
- The general and disease-related characteristics, self-efficacy, and upper grip strength of the experimental and control groups were measured using a pre-experiment questionnaire, and blood calcium and blood phosphorus tests were performed before starting hemodialysis. After starting dialysis, the blood flow rate was measured using the ultrasound dilution method.
- The program featured upper extremity strength exercises, a phosphorus-restricted diet, health education and health counseling on AVF management methods, and text messages. Its validity was verified by 5 experts: 1 professor of nephrology, 1 kidney center nurse, and 3 nursing professors. The content validity index (CVI) was determined. The composition and content of the AVF program were evaluated using a content validity evaluation table. Possible answers included “very appropriate” (4 points), “suitable” (3 points), “inappropriate” (2 points), and “very inappropriate” (1 point). Based on the number of expert-assigned scores of 3 or more points, the CVI was calculated to be ≥0.8 points.
- Weekly training on AVF muscle strength exercises, diet, and AVF management was provided for patients receiving hemodialysis via health information magazines, direct demonstrations, and videos.
- (1) AVF upper extremity strength exercise: Based on a previous study, the upper extremity of the AVF was exercised using a hand gripper, and the gripper strength was gradually increased. The intensity of the gripper (GD Grip) was set based on 8 step-by-step exercises, and the intensity and frequency were adjusted. During weekly counseling, we monitored patients’ performance of the exercise and provided direct demonstrations. Step 1 started by adjusting the strength of the gripper to 8 kg and with 30 repetitions. Two sets of 30 repetitions were performed per day. The second, third, and fourth steps required 40, 50, and 60 repetitions, respectively. In step 5, the strength of the gripper was adjusted to 16 kg, and 2 sets of 30 repetitions were performed per day. Similarly, steps 6, 7, and 8 required 2 sets each of 40, 50, and 60 repetitions, respectively.
- (2) Diet: Diets lasted for 8 weeks based on previous research and covered the following areas: phosphorus and the role it plays in the body, problems that occur when the blood phosphate level is high, how to prevent complications, foods with high phosphorus content, and the relationship between calcification and vascular ducts. Health information magazines were used to educate patients receiving hemodialysis on healthy eating regimens and complications.
- (3) AVF management: To educate patients about AVF vascular management, video education was provided on AVF complications, self-management, lifestyle, proper hemostasis methods, and vascular compression methods.
- Health counseling involved a checklist of AVF upper extremity strength exercises, explaining the results of physiological indicators, confirming the correct upper extremity strength exercise methods, determining whether exercises were performed, and confirming the implementation of AVF self-management and a phosphorus-restricted diet.
- Weekly text messages were sent to encourage the participants to practice the AVF exercises, the phosphorus-restricted diet, and vascular self-management.
- The experimental group received a nursing intervention focused on AVF prevention, while the control group received general nursing interventions. Before the intervention, the experimental group was educated about the purpose of the study and the process of the program. A list of actions was prepared to confirm whether each participant performed the upper extremity exercises according to the plan, which was checked weekly. AVF management and phosphorus-restricted diet education were conducted using health information magazines and videos. The program was implemented in 8 sessions, and health education was conducted for 20 minutes during dialysis, including 10 minutes of education using videos and a health information magazine. After completing dialysis every Friday, individual counseling was conducted for 20 minutes in the counseling room, and a text message was sent.
- In the first week of the experiment, the first stage of the AVF upper extremity exercise was introduced, and a demonstration was performed using an actual gripper. The strength of the gripper was adjusted to 8 kg, and the participants were taught to practice the grasping and unfolding exercise in 1 set of 30 repetitions, with 2 sets each day.
- The patients were taught about the significance of a phosphorus-restricted diet and vascular calcification, and AVF management was taught through a video. Counseling was conducted to ensure that the participants practiced the exercises and diet and to encourage them to practice. A text message was sent after the video training on AVF management. In weeks 2, 3, and 4 of the experiment, upper extremity grip exercises were introduced at each stage. After training was provided using a health information magazine, the practice list was checked, and text messages were sent. In week 5, the results of the risk index after the first post-survey were interpreted, and the researchers explained the action plan, gave feedback, and sent a text message to those in the high-risk group, which performed poorly. In weeks 6, 7, and 8, step-by-step upper extremity grip exercises were introduced, and dietary education and AVF management methods were retaught using health information magazines. The patient’s practice list was checked, and text messages were sent.
- Follow-up surveys were completed 4 and 8 weeks after individual education and counseling. Upper grip strength, blood flow rate, physiological indicators, and self-efficacy were measured in both groups. The AVF stenosis prevention program structure is depicted in Table 2.
- Data Analysis
- The collected data were analyzed using IBM SPSS ver. 23.0 (IBM Corp.). The general and disease-related characteristics of the participants were analyzed using frequencies, percentages, means, and standard deviations. Pre-intervention homogeneity tests for general characteristics, disease-related characteristics, upper extremity muscle strength, self-efficacy, physiological indicators, and blood flow velocity were conducted using the chi-square test, Fisher exact test, and the t-test. For dependent variables, a normality test was performed using the Shapiro-Wilk test, and differences between the experimental and control groups were analyzed using repeated measures analysis of variance (ANOVA).
- Ethical Considerations
- Data were collected after receiving approval (IRB No: 40525-201610-HR-114-01) through research deliberation by the Institutional Review Board of Keimyung University.
Materials and Methods
Participants’ general and disease-related characteristics
Upper extremity strength
Blood flow rate
Physiological indicators
Self-efficacy
Preliminary investigation
Content of the AVF stenosis prevention program
Health education
Health counseling
Text messages
Program application
Follow-up surveys
- Tests for Homogeneity between Groups
- Between-group baseline homogeneity was confirmed for all general and disease-related characteristics.
- In total, 56% of participants in the experimental group were male, and 60% of those in the control group were female. Additionally, 52% of the experimental group and 56% of the control group were aged 54 years or older. The duration of dialysis was fewer than 5 years for 56% of the experimental group and more than 5 years for 60% of the control group. Hypertension was the most common causative disease in each group, at 40% in the experimental group and 48% in the control group. There was no AVF occlusion in 60% and 48% of those in the experimental and control groups, respectively, and the most common AVF location was the left forearm in both groups (experimental group, 44%; control group, 40%). The duration of AVF was fewer than 4 years in 56% of the experimental group and more than 4 years in 64% of the control group. Information on other demographic and disease-related characteristics is presented in Table 3.
- No statistically significant differences were observed in the baseline homogeneity test for the dependent variables; therefore, the homogeneity of the 2 groups was confirmed (t=0.85−1.30, p=0.201−0.968). Prior to the experiment, the average upper hand grip strength was 22.68 points in the experimental group and 22.77 points in the control group, and the average blood flow rate was 1,221.20 mL/min in the experimental group and 1,319.20 mL/min in the control group. The average serum calcium was 9.25 mg/dL in the experimental group and 9.37 mg/dL in the control group, and the average serum phosphorus was 6.36 mg/dL in the experimental group and 5.87 mg/dL in the control group. Additionally, the average self-efficacy was 2.66 points in the experimental group and 2.61 points in the control group (Table 4).
- Hypothesis Validation
- Hypothesis 1: There will be differences in the upper extremity muscle strength of the experimental and control groups participating in the AVF stenosis prevention program over time.
- The mean grip strength score of the experimental group was 22.68 points at baseline, 26.04 points after 4 weeks, and 32.21 points after 8 weeks; for the control group, the mean score was 22.77 points at baseline, 22.12 points after 4 weeks, and 20.98 points after 8 weeks. Repeated measures ANOVA for changes in upper extremity muscle strength between the groups showed a statistically significant interaction between the group and time point (F=15.23, p<0.001). A significant difference was observed between the groups (F=4.32, p=0.043) as well as between the measurement time points (F=7.09, p=0.002) (Table 5). Therefore, the first hypothesis was confirmed.
- Hypothesis 2: There will be a difference in the blood flow velocity between the experimental and control groups participating in the AVF stenosis prevention program over time.
- The mean blood flow velocity of the experimental group was 1,221.20 mL/min at baseline, 1,252 mL/min after 4 weeks, and 1,499.20 mL/min after 8 weeks. For the control group, it was 1,319.20 mL/min at baseline, 1,296.80 mL/min after 4 weeks, and 1,212.80 mL/min after 8 weeks. The results of repeated measures ANOVA for changes in blood flow velocity in the groups showed a significant interaction between the group and time point (F=36.00, p<0.001) and between the groups. (F=300.89, p<0.001). A significant difference was also observed between the time points (F=7.17, p=0.010) (Table 5). Therefore, the second hypothesis was confirmed.
- Hypothesis 3: The experimental and control groups participating in the AVF stenosis prevention program will experience changes in physiological indicators over time.
- Additional hypothesis 3−1: The serum calcium index will differ between the experimental and control groups participating in the AVF stenosis prevention program over time.
- The average serum calcium of the experimental group was 9.25 mg/dL at baseline, 9.01 mL/min after 4 weeks of the intervention, and 9.29 mg/dL after 8 weeks. For the control group, it was 9.37 mg/dL at baseline and 9.26 mg/dL after 4 weeks. After 8 weeks, it was 9.14 mg/dL. The results of repeated measures ANOVA on the change in the calcium index between the groups showed no interaction between the groups and the time point (F=2.23, p=0.142), no significant difference between the groups (F=0.33, p=0.570), and no significant difference between time points (F=2.20, p=0.277) (Table 5). Additional hypothesis 3−1 was rejected.
- Additional hypothesis 3−2: The experimental and control groups participating in the AVF stenosis prevention program will show differences in the serum phosphorus index over time.
- The average serum phosphorus of the experimental group was 6.36 mg/dL at baseline, 5.48 mg/dL after 4 weeks, and 5.01 mg/dL after 8 weeks. For the control group, it was 5.87 mg/dL at baseline, 5.52 mg/dL after 4 weeks, and 5.47 mg/dL after 8 weeks. As a result of repeated measures ANOVA for the changes in the phosphorus index of the groups, a significant difference was found in the interaction between the groups and the time point (F=8.64, p<0.001) and between the groups (F=3.72, p<0.001). A significant difference was also observed between the time points (F=0.09, p<0.001) (Table 5). Additional hypothesis 3−2 was confirmed.
- Hypothesis 4: There will be a difference in self-efficacy between the experimental and control groups participating in the AVF stenosis prevention program over time.
- The mean self-efficacy of the experimental group was 2.66 points at baseline, 2.76 points after 4 weeks, and 3.00 points after 8 weeks. For the control group, it was 2.60 points at baseline, 2.60 points after 4 weeks, and 2.61 points after 8 weeks. Repeated measures ANOVA for the change in self-efficacy between the groups showed a statistically significant interaction between the groups and the time point (F=18.62, p<0.001). Significant differences between the measurement time points (F=19.59, p<0.001) and between the groups (F=4.26, p=0.045) were also observed (Table 5). Therefore, hypothesis 4 was confirmed.
Results
Homogeneity of general characteristics and disease-related characteristics
Baseline homogeneity tests for dependent variables
Validation of hypothesis 1
Validation of hypothesis 2
Validation of hypothesis 3
Validation of hypothesis 4
- This study investigated the effects of an AVF stenosis prevention program for patients receiving hemodialysis on upper extremity muscle strength, blood flow rate, physiological indicators, and self-efficacy and to examine the clinical implementation of an AVF nursing intervention program.
- The AVF stenosis prevention program featured exercise therapy, a phosphorus-restricted diet, and AVF self-care; these have been used in previous studies [12,13,20,30] to prevent vascular maturation failure and vascular calcification, which are factors that correspond to AVF stenosis. Exercise therapy aims to increase the blood vessel size and blood flow of AVF blood vessels [31]. The phosphorus-restricted diet was intended to prevent hyperphosphatemia, a factor in vascular calcification [12]. Previous studies utilized single therapies despite the pathophysiological complexity of vascular calcification; therefore, the therapy regimen in this study that combined exercise, dietary restriction, and vascular self-management was designed to comprehensively mediate factors related to vascular calcification in patients receiving hemodialysis. Additionally, given the low rate of self-management of patients receiving hemodialysis [18], self-monitoring was strengthened to enhance self-efficacy using a practice list to foster self-actualization, and text message support and feedback counseling were included to increase patients’ self-management practice. Therefore, in this study, upper extremity muscle strength and blood flow velocity (as clinical indicators of AVF stenosis), serum calcium and phosphorus (as risk indicators of vascular calcification), and self-efficacy were utilized as variables to understand the effects of the AVF program.
- Consequently, the AVF stenosis prevention program for patients receiving hemodialysis applied in this study was found to be effective in enhancing upper extremity muscle strength through gripping exercises and preventing AVF stenosis by reducing blood phosphorus levels and improving the blood flow rate.
- Upper extremity strength exercises are recommended to promote the arterialization of veins after AVF surgery in patients receiving hemodialysis and to increase blood vessel patency through increased blood flow and vasodilation. In patients receiving hemodialysis who participated in the AVF stenosis prevention program, upper extremity muscle strength showed a synergistic effect with time, with scores increasing by 3.36 points after 4 weeks and 6.18 points after 8 weeks. These results were higher than the 0.9-point increase in the study by Lee [32], in which muscle-strengthening exercises were used to increase the patency of blood vessels in the same participants, resulting in a 1.79-point decrease in the control group. Additionally, Heo [24] reported that, as grip strength improved, the hand, elbow, and shoulder joints also showed higher muscle strength. Kim [33] reported that patients using a gripper could prevent muscle atrophy or loss without applying 100% force, suggesting that gripper exercises are effective in improving upper extremity muscle strength. Exercises with grippers are considered extremely effective in increasing muscle strength in the weakened AVF-containing upper extremities of patients receiving hemodialysis due to the proven effect of gradual muscle exercise in improving upper extremity muscle strength. In particular, the grip strength scores at 4 and 8 weeks were 26.04 points and 32.21 points, respectively, indicating a greater strength increase in the final 4 weeks than in the first 4 weeks. Thus, 2 months of steady exercise was shown to be more effective than 1 month of exercise. Although more women participated in this study than men and a higher proportion of patients received dialysis for 5 or more years in the control group than in the experimental group, the upper extremity muscle strength results were significant. This could be the result of steady and systematic upper grip strength exercise and management, and it was found that more active interventions by nurses are crucial in clinical practice.
- Blood flow velocity, a clinical indicator of AVF stenosis, showed increases of 31 mL/min after 4 weeks and 278 mL/min after 8 weeks compared to before the program. The blood flow rate significantly increased after 8 weeks rather than 4 weeks, showing similar results to those of the increases in upper extremity exercise after 8 weeks and 4 weeks, which is likely attributable to increased blood flow velocity as blood flow increases. This finding is the same as that in a study by Henedy [21], in which the blood flow rate of the AVF increased as a result of increased blood flow due to an increase in the thickness of the arteries and veins from AVF exercise. These results are likely due to the encouragement and support given to patients receiving hemodialysis via text messages and the assistance given to them regarding the proper implementation of the exercise method through repeated and systematic health education and weekly demonstrations. Although it was not possible to measure the increase in vein thickness after routine upper extremity grip exercises, the participants shared that they visually observed the thickening of the AVF blood vessels during counseling. As a result of training to directly assess the thrill in the AVF during AVF self-management, the participants shared that the thrill increased after the start of exercise. However, the measured blood flow rate never fell below 600 mL/min, and in the control group, which did not practice the exercises, the blood flow rate decreased by 106.4 mL/min compared to before the program.
- In this study, a phosphorus-restricted diet program was implemented to control calcium and phosphorus levels, which are risk indicators for the vascular calcification of AVFs in patients receiving hemodialysis. Consequently, among those who participated in this study’s AVF stenosis prevention program, normal calcium levels were maintained, while phosphorus levels decreased over time. The blood calcium level was 9.25 mg/dL before the program, 9.00 mg/dL after 4 weeks, and 9.28 mg/dL after 8 weeks, with no significant difference between time points and the interaction between the groups and time points. This indicates that the patients maintained a normal level. Contrary to the results regarding the multiplication of calcium and phosphorus levels as a physiological index in a study by Lee et al. [34], who conducted a phosphorus-related nursing intervention, calcium levels did not change in the present study. Among the risk indicators of vascular calcification, the average phosphorus value was 6.36 mg/dL before the program; it decreased by 0.88 to 5.48 mg/dL after 4 weeks and further decreased to 5.01 mg/dL after 8 weeks. Therefore, reducing serum phosphorus levels through periodic and repeated education and counseling is considered effective in terms of the development and application of the program.
- In this study, the average self-efficacy score of patients receiving hemodialysis was 2.66 out of 4 points; in the study by Kim and Choi [18], who used the same tool for patients receiving hemodialysis, the average self-efficacy score was 3.24, indicating low self-efficacy. In terms of the self-efficacy measurement, water and dietary management scores were high, but the exercise and blood vessel management scores were relatively low. However, after the program, the self-efficacy scores for exercise and vascular management increased. This was likely due to the effect of weekly individual counseling and education on upper grip strength exercises and AVF management. In this study, direct health counseling was provided to identify difficulties and problems in self-care, devise more suitable methods, and encourage motivation and confidence through text messages. The majority of patients (60%−76%) did not have jobs due to their frequent hospitalization and prolonged illness. Participation in this research program increased social contact, which invigorated patients and improved their quality of life, which is thought to have led to increased social activity. Therefore, patients receiving hemodialysis with chronic diseases should receive assistance to maintain a healthy lifestyle through self-care, including dieting and blood vessel management, and routine, rather than one-off, nursing interventions.
- To summarize, the program in this study was confirmed to be effective in preventing AVF stenosis in patients receiving hemodialysis, and it is expected to be useful for continuous vascular management. Additionally, it will be useful in nursing intervention programs to increase the effectiveness of AVF self-management, as it has shown promising results in patients receiving hemodialysis for ensuring homogeneity in the improvement of upper extremity muscle strength, self-efficacy, the phosphorus index, and the blood flow rate to prevent AVF stenosis. However, future studies should be conducted to supplement our findings since this study included patients receiving hemodialysis in an artificial kidney room at a single hospital only, and the exogenous variables related to the participants’ meal intake and nutritional status were insufficient.
Discussion
- This study aimed to prevent AVF stenosis in patients undergoing hemodialysis by conducting an AVF stenosis prevention program over 8 weeks for 50 outpatient dialysis patients at Keimyung University Dongsan Medical Center in Daegu, Republic of Korea. The AVF stenosis prevention program resulted in an increase in upper extremity muscle strength through grip strength exercises and was effective in preventing AVF stenosis by increasing the blood flow rate. A phosphorus-restricted diet and AVF management methods ensured normal calcium index values and led to a decrease in phosphorus index levels. Additionally, given that encouragement and support through text messages and practice lists improved self-efficacy, a program should be implemented that provides ongoing education.
- Our suggestions for future studies are as follows. First, for the treatment and self-management of patients receiving hemodialysis, routine individual education programs and materials that consider patients’ dietary intake and nutritional status should be designed. Second, the program in this study should be expanded and repeated as an effective nursing intervention for the prevention and management of AVF stenosis in patients receiving hemodialysis. Third, a follow-up study is needed to determine whether the preventive effect on AVF stenosis continues after the end of the program.
Conclusion
- • Patients undergoing hemodialysis for end-stage renal failure should receive knowledge about self-care through ongoing individual education and feedback rather than temporary education interventions.
- • In this study, text messages and self-care practice helped patients lead a healthy lifestyle during dialysis by enhancing their self-efficacy.
- • The program in this study effectively prevented arteriovenous fistula (AVF) stenosis in hemodialysis patients, and it is expected to be useful for continuous vascular management and as part of nursing interventions for the effective self-management of AVFs.
HIGHLIGHTS
-
Ethics Approval
This study was approved by the Institutional Review Board of Keimyung University (IRB No: 40525-201610-HR-114-01) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained for the publication of this study and accompanying images.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Availability of Data
The datasets are not publicly available but are available from the corresponding author upon reasonable request.
-
Authors’ Contributions
Conceptualization: all authors; Data curation: all authors; Formal analysis: all authors; Funding acquisition: all authors; Investigation: HL; Methodology: GB, EL; Project administration: all authors; Resources: all authors; Software: all authors; Supervision: all authors; Validation: all authors; Visualization: all authors; Writing–original draft: all authors; Writing–review & editing: all authors. All authors read and approved the final manuscript.
Article information
| Subject | Preliminary investigation | Intervention | Post-investigation 1 | Post-investigation 2 |
|---|---|---|---|---|
| Experimental group | Ye1 | Xe | Ye2 | Ye3 |
| Control group | Yc1 | Yc2 | Yc3 |
AVF, arteriovenous fistula; Xe, AVF stenosis prevention program (AVF upper extremity strength exercise, health education on phosphorus-restricted diet and AVF management, health counseling, and text messages); Ye1, Yc1, investigation of general and disease-related characteristics, upper extremity muscle strength measurement, blood flow velocity measurement, serum calcium and phosphorus measurement, and self-efficacy measurement; Ye2, Ye3, Yc2, and Yc3, measurement of upper extremity muscle strength, blood flow rate, serum calcium and phosphorus levels, and self-efficacy.
| Characteristic | Experimental group (n=25) | Control group (n=25) | χ2/Fishera) | p |
|---|---|---|---|---|
| Sex | ||||
| Male | 14 (56.0) | 10 (40.0) | 1.28 | 0.258 |
| Female | 11 (44.0) | 15 (60.0) | ||
| Age (y) | ||||
| <54 | 12 (48.0) | 11 (44.0) | 0.08 | 0.777 |
| ≥54 | 13 (52.0) | 14 (56.0) | ||
| Marital status | ||||
| Married | 18 (72.0) | 14 (56.0) | 1.61a) | 0.517 |
| Not married | 4 (16.0) | 5 (20.0) | ||
| Otherb) | 3 (12.0) | 6 (24.0) | ||
| Family | ||||
| Yes | 22 (88.0) | 21 (84.0) | 0.17a) | 0.500 |
| No | 3 (12.0) | 4 (16.0) | ||
| Education | ||||
| Less than middle school | 6 (24.0) | 7 (28.0) | 0.14 | 0.931 |
| High school | 11 (44.0) | 11 (44.0) | ||
| College or higher | 8 (32.0) | 7 (28.0) | ||
| Job status | ||||
| Employed | 10 (40.0) | 6 (24.0) | 1.47 | 0.225 |
| Not employed | 15 (60.0) | 19 (76.0) | ||
| Economic status | ||||
| Medium or higher | 15 (60.0) | 12 (48.0) | 0.73 | 0.395 |
| Low | 10 (40.0) | 13 (52.0) | ||
| Dialysis period (y) | ||||
| <5 | 14 (56.0) | 10 (40.0) | 1.28 | 0.258 |
| ≥5 | 11 (44.0) | 15 (60.0) | ||
| Causative disease | ||||
| Diabetes | 6 (24.0) | 3 (12.0) | 1.37a) | 0.821 |
| Hypertension | 10 (40.0) | 12 (48.0) | ||
| Chronic glomerulonephritis | 7 (28.0) | 8 (32.0) | ||
| Otherc) | 2 (8.0) | 2 (8.0) | ||
| Body weight (kg) | ||||
| <60 | 12 (48.0) | 12 (48.0) | 0.00 | 1.000 |
| 60−69 | 8 (32.0) | 8 (32.0) | ||
| ≥70 | 5 (20.0) | 5 (20.0) | ||
| Weight gain after dialysis (kg) | ||||
| 1−2 | 7 (28.0) | 7 (28.0) | 1.80 | 0.407 |
| 2−3 | 8 (32.0) | 12 (48.0) | ||
| >3 | 10 (40.0) | 6 (24.0) | ||
| Heparin usage (U) | ||||
| ≤600 | 23 (92.0) | 19 (76.0) | 2.38a) | 0.123 |
| ≥800 | 2 (8.0) | 6 (24.0) | ||
| Maturity period (wk) | ||||
| ≤5 | 7 (28.0) | 7 (28.0) | 0.00 | 1.000 |
| ≥6 | 18 (72.0) | 18 (72.0) | ||
| Occlusion experience | ||||
| None | 15 (60.0) | 12 (48.0) | 5.33a) | 0.083 |
| 1 or 2 | 9 (36.0) | 6 (24.0) | ||
| ≥3 | 1 (4.0) | 7 (28.0) | ||
| Location of AVF | ||||
| Left wrist | 5 (20.0) | 3 (12.0) | 5.34a) | 0.394 |
| Left forearm | 11 (44.0) | 10 (40.0) | ||
| Left upper arm | 6 (24.0) | 3 (12.0) | ||
| Right wrist | 0 (0) | 3 (12.0) | ||
| Right forearm | 1 (4.0) | 3 (12.0) | ||
| Right upper arm | 2 (8.0) | 3 (12.0) | ||
| Duration of AVF use (y) | ||||
| <4 | 14 (56.0) | 9 (36.0) | 2.01 | 0.156 |
| ≥4 | 11 (44.0) | 16 (64.0) | ||
| Smoking status | ||||
| Non-smoker | 23 (92.0) | 21 (84.0) | 0.76a) | 0.334 |
| Smoker | 2 (8.0) | 4 (16.0) | ||
| No. of medications | ||||
| <7 | 13 (52.0) | 12 (48.0) | 0.08 | 0.777 |
| ≥8 | 12 (48.0) | 13 (52.0) |
- 1. Duan J, Wang C, Liu D, et al. Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in Chinese rural residents: a cross-sectional survey. Sci Rep 2019;9:10408. ArticlePubMedPMCPDF
- 2. Jafari-Koulaee A, Moosazadeh M, Bagheri Nesami M, et al. Effect of cryotherapy on arteriovenous fistula puncture-related pain in hemodialysis patients: a systematic review and meta-analysis. Complement Ther Med 2020;49:102326. ArticlePubMed
- 3. GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020;395:709−33.PubMedPMC
- 4. Centers for Disease Control and Prevention (CDC). Chronic kidney disease in the United States, 2019. US Department of Health and Human Services, CDC; 2019.
- 5. Lyu B, Chan MR, Yevzlin AS, et al. Catheter dependence after arteriovenous fistula or graft placement among elderly patients on hemodialysis. Am J Kidney Dis 2021;78:399−408.ArticlePubMed
- 6. Kazemzadeh G, Modaghegh M, Ravari H, et al. Investigation of affecting factors on early artery-venous fistulas failure in patients with less than 20 years old. Med J Mashhad Univ Med Sci 2017;60:580−5.
- 7. Yoon SE, Choi SY, Cho SB. Safety and efficacy of the percutaneous manual aspiration thrombectomy technique to treat thrombotic occlusion of native arteriovenous fistulas for hemodialysis. Taehan Yongsang Uihakhoe Chi 2020;81:409−17. Korean.ArticlePubMedPMCPDF
- 8. Shin D, Kim YJ, Yang SB, et al. Effectiveness and influencing factors of percutaneous transluminal angioplasty for stenosis of transposed brachiobasilic arteriovenous fistula. J Korean Soc Radiol 2019;80:477−89.ArticlePDF
- 9. Gameiro J, Ibeas J. Factors affecting arteriovenous fistula dysfunction: a narrative review. J Vasc Access 2020;21:134−47.ArticlePubMedPDF
- 10. Al-Jaishi AA, Oliver MJ, Thomas SM, et al. Patency rates of the arteriovenous fistula for hemodialysis: a systematic review and meta-analysis. Am J Kidney Dis 2014;63:464−78.ArticlePubMed
- 11. Yoo CS, Kim Y, Kim HY. Impact of chronic kidney disease on depression, perceived health, and health-related quality of life: results from the Korea National Health and Nutrition Examination Survey in 2014 and 2016. Korean J Adult Nurs 2020;32:374−84. Korean.ArticlePDF
- 12. Brown RS, Patibandla BK, Goldfarb-Rumyantzev AS. The survival benefit of “fistula first, catheter last” in hemodialysis is primarily due to patient factors. J Am Soc Nephrol 2017;28:645−52.ArticlePubMed
- 13. Wilmink T, Hollingworth L, Powers S, et al. Natural history of common autologous arteriovenous fistulae: consequences for planning of dialysis. Eur J Vasc Endovasc Surg 2016;51:134−40.PubMed
- 14. Tanner NC, da Silva AF. Medical adjuvant treatment to improve the patency of arteriovenous fistulae and grafts: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg 2016;52:243−52.ArticlePubMed
- 15. Ki EJ, So HS. Development and effects of smartphone app-based exercise program for hemodialysis patients. J Korean Acad Nurs 2020;50:52−65. Korean.ArticlePubMedPDF
- 16. Shin SY, Han KH, Jeong HY, et al. Vascular calcification scores are associated with arterial stiffness, inflammation, and nutrition in hemodialysis patients. Korean J Med 2014;87:42−52. Korean.Article
- 17. Gebrie MH, Ford J. Depressive symptoms and dietary non-adherence among end stage renal disease patients undergoing hemodialysis therapy: systematic review. BMC Nephrol 2019;20:429. ArticlePubMedPMCPDF
- 18. Kim S, Choi Y. The effects of tailored dietary education among role failure hemodialysis patients on self-care compliance, self-efficacy and physiologic indices. Korean J Rehabil Nurs 2021;24:46−55. Korean.Article
- 19. Bandura A. The explanatory and predictive scope of self-efficacy theory. J Soc Clin Psychol 1986;4:359−73.Article
- 20. Fuzari HK, Leite J, Souza H, et al. Exercise effectiveness of arteriovenous fistula maturation in chronic renal patients: a systematic review with meta-analysis. Int J Ther Rehabil 2017;24:98−104.Article
- 21. Henedy WM. Effect of designed nursing intervention protocol on postoperative arteriovenous fistula complications and maturation among patients with end stage renal disease. Int J Novel Res Healthc Nurs 2019;6:226−39.
- 22. Fontsere N, Mestres G, Yugueros X, et al. Effect of a postoperative exercise program on arteriovenous fistula maturation: a randomized controlled trial. Hemodial Int 2016;20:306−14.ArticlePubMedPDF
- 23. Kim SK, Park HJ, Yang DH, et al. Influences on the performance based frailty of physical performance, exercise self-efficacy, decisional balance, and health related quality of life in adults undergoing hemodialysis. Korean J Adult Nurs 2018;30:149−60. Korean.ArticlePDF
- 24. Heo M. Effects of a functional upper extremity motor task on upper extremity functions and daily living activities for inpatients with stroke. J Korean Entertain Ind Assoc 2016;7:131−6. Korean.
- 25. Lim HJ, Choi EH, Kim EJ, et al. The effect of arteriovenous fistula cannulation direction and puncture distance on the recirculation rate of hemodialysis patients. J Korean Crit Care Nurs 2018;11:28−34.
- 26. Chun Y, Park S. Effects of the auricular acupressure on pruritus and fatigue in hemodialysis patients. Korean J Adult Nurs 2016;28:436−46. Korean.ArticlePDF
- 27. Park HY, Nam SI. A qualitative case study on dialysis adaptation experience in chronic kidney disease patients. Korean J Qual Res Soc Welf 2021;15:5−30. Korean.
- 28. Kim JH, Kim MJ. Factors affecting the quality of life of hemodialysis patients. J Soc Adult Nurs 1995;7:299−312. Korean.
- 29. Choi EY, Lee HY. The relationship of fatigue, self efficacy, family support and sleep factor in hemodialysis patients. J Korean Acad Adult Nurs 2005;17:435−43.
- 30. Lee K, Lim S, Kang Y. Psychometric evaluation of self-management scale for hemodialysis patients with arteriovenous fistula. Korean J Adult Nurs 2017;29:637−46. Korean.ArticlePDF
- 31. Mo Y, Song L, Sun C, et al. Effect of dumbbell exercise on arteriovenous fistula in patients undergoing maintenance haemodialysis: a prospective randomized controlled trial. Blood Purif 2020;49:16−24.ArticlePubMedPDF
- 32. Lee J. Effects of a muscle strength reinforcement exercise program for older adult patients on hemodialysis. J Korean Gerontol Nurs 2018;20:204−16. Korean.ArticlePDF
- 33. Kim JH. Relationship between handgrip strength and cardiopulmonary fitness in patients with myocardial infarction. J Korea Acad Ind Coop Soc 2018;19:506−14. Korean.
- 34. Lee JH, Kam S, Kim KY, et al. The effect of phosphorus-related nursing intervention on physiologic indicators of hemodialysis patients. J Health Info Stat 2016;41:239−47. Korean.ArticlePDF
 Cite
Cite