Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 14(4); 2023 > Article
-
Review Article
Public health agencies’ use of social media for communication during pandemics: a scoping review of the literature -
Babatunde Abiodun Balogun1
 , Anne Hogden1,2, Nenagh Kemp3, Lin Yang4, Maria Agaliotis1
, Anne Hogden1,2, Nenagh Kemp3, Lin Yang4, Maria Agaliotis1 -
Osong Public Health and Research Perspectives 2023;14(4):235-251.
DOI: https://doi.org/10.24171/j.phrp.2023.0095
Published online: August 9, 2023
1Australian Institute of Health Service Management, College of Business and Economics, University of Tasmania, Sydney, Australia
2School of Population Health, Faculty of Medicine & Health, University of New South Wales, Sydney, Australia
3School of Psychological Sciences, College of Health and Medicine, University of Tasmania, Hobart, Australia
4Department of Marketing, College of Business and Economics, University of Tasmania, Hobart, Australia
- Corresponding author: Babatunde Abiodun Balogun Australian Institute of Health Service Management, College of Business and Economics, University of Tasmania, Rozelle campus, Glover Street, Lilyfield, Sydney, New South Wales, Australia E-mail: babatunde.balogun@utas.edu.au
© 2023 Korea Disease Control and Prevention Agency.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
- 1,740 Views
- 150 Download
Abstract
- Public health agencies (PHAs) have increasingly incorporated social media into their communication mix during successive pandemics in the 21st century. However, the quality, timing, and accuracy of their health messages have varied significantly, resulting in mixed outcomes for communication, audience engagement, and pandemic management. This study aimed to identify factors influencing the effectiveness of pandemic-related health messages shared by PHAs on social media and to report their impact on public engagement as documented in the literature. A scoping literature review was conducted following a predefined protocol. An electronic search of 7 relevant databases and 5 grey literature repositories yielded 9,714 papers published between January 2003 and November 2022. Seventy-three papers were deemed eligible and selected for review. The results underscored the insufficiency of social media guidance policies for PHAs. Six themes were identified: message source, message topic, message style, message timing, content credibility and reliability, and message recipient profile. These themes encompassed 20 variables that could inform PHAs’ social media public health communication during pandemics. Additionally, the findings revealed potential interconnectedness among the variables, and this study concluded by proposing a conceptual model that expands upon existing theoretical foundations for developing and evaluating pandemic-related health messaging.
- Social media has introduced a new dimension to communication and interaction in today’s world. Built on advanced Web 2.0 technology and applications, social media platforms enable real-time, multi-directional communication, interaction, and engagement among users, as well as the sharing of user-generated content [1]. Consequently, social media has revolutionized the way we communicate by fostering the continuous exchange of information and co-creation of user experiences. Messages can be targeted at a specific audience of followers without the need for an intermediary, which is typically required in traditional forms of communication. Additionally, feedback can be received directly from the audience.
- Public health agencies (PHAs) have gradually embraced social media as an essential communication tool. This positive development is particularly important during pandemics when the public seeks regular, relevant updates and information. The 21st century has witnessed a series of pandemics, coinciding with the rise of social media [2,3]. Over time, PHAs have expanded their ability to use social media as one of the tools for managing pandemics.
- A pandemic is a disease that simultaneously breaks out in multiple geographical locations worldwide, caused by a new and highly pathogenic microbe (or a variant thereof) to which humans have no prior immunological resistance [4]. A pandemic disease can easily cross international borders and spread within communities, constituting a public health emergency of international concern (PHEIC). Therefore, a swift and coordinated effort that focuses the attention and resources of governments and the public health community is always necessary to respond to and ultimately end a pandemic [4]. In the past 20 years, the World Health Organisation (WHO) has declared 6 diseases as constituting PHEICs (Table 1) [4−7]. Given the frequency of PHEIC declarations, global preparedness for managing another potential declaration in the future is crucial.
- One of the primary reasons that PHAs are established at all levels of government is to guide and coordinate efforts and initiatives aimed at preventing the spread of pandemics. Modern PHAs have evolved over 300 years, reflecting the growing sophistication of territories in managing diseases with the potential for rapid community transmission [8]. This crucial responsibility of PHAs is rooted in one of the most fundamental principles of public health: the control of communicable infections [9]. Public health communication during pandemics is a core responsibility of PHAs [9,10]. The success of preparedness, response, and control measures for pandemics relies on the dissemination of accurate health messages that inform and empower individuals to make sound health decisions [11,12]. When misconceptions exist among the public, there is an increased risk of pandemic spread [13]. Effective communication fosters positive action from the population.
- PHAs have increasingly incorporated the use of social media into their communication mix with each successive pandemic [14]. Pandemics typically involve significant uncertainty and knowledge gaps, which intensify the demand for accurate and reliable health information [15]. As individuals increasingly turn to social media for health-related information, PHAs have established social media accounts to address these needs [16]. The effectiveness of using social media to disseminate health message is demonstrated by increased reach [17] and interaction with the public [18]. However, social media communication during a pandemic presents unique challenges. Pandemics involve novel diseases that often necessitate continuously evolving messages from PHAs as the situation develops [19]. This complexity can be compounded by unscrupulous and unauthorized individuals and organizations spreading inaccurate health information, which can undermine and overshadow credible sources [20]. The number of followers on PHAs’ social media accounts tends to increase significantly during pandemics [21]. However, followers may soon become dissatisfied with the level of engagement they receive due to conflicting messages from different agencies on the same topic within the same timeframe [22,23] or from a particular agency on the same issue at different times [22,24].
- There is a growing body of research that evaluates and promotes the use of social media platforms by PHAs for communicating health messages during pandemics. However, it remains unclear whether these studies have comprehensively captured all the potential components of pandemic-related health messages by PHAs via their social media accounts that could foster effective public engagement and influence societal behavior [25−27]. This argument is based on the diverse contexts and research methodology used in studies [28,29], which limit the replicability of results. This scoping review aimed to synthesize the variables that influence the effectiveness of health messages from PHAs via their social media accounts during pandemics. To achieve this, we conducted a comprehensive overview of the existing research literature on PHAs’ social media health communication during pandemics over the past 20 years.
Introduction
- We conducted a scoping literature review to identify studies and documents relevant to our research scope. The scoping review methodology is well-suited for exploring a new field where evidence from previous research is scarce [30]. Therefore, the search for pertinent references in a scoping review encompasses both published journal articles and grey literature [30]. We followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) [31].
- Search Strategy and Selection
- We searched 7 bibliographic databases (Sociological Abstracts, Medline, PsycInfo, Scopus, Health Business Elite, Health Policy Reference Centre, and Embase) for relevant peer-reviewed publications. These databases encompass reference sources for biomedical research, behavioral and sociological research, healthcare administration and policy issues, and related fields of interest. For grey literature searches, we consulted 5 sources: Bielefeld Academic Search Engine (BASE), WHO’s Institutional Repository for Information Sharing (IRIS), and the .gov.au and .edu.au domains of the Google platform (each search limited to the first 5 pages).
- We developed the search terms based on our research aim and in consultation with a healthcare specialist university research librarian, using the Sample-Phenomenon-of-Interest-Design-Evaluation-Research-type (SPIDER) framework [32]. We defined our sample (population of interest) as publicly funded health agencies at all levels of governance, and the phenomenon of interest as social media communication of public health messages during a pandemic. The design described the research methodologies used, while the evaluation focused on how members of the public engaged with and utilized the public health messages.
- Following this process, we selected 3 key search terms: “social media”, “healthcare communication”, and “pandemic management”. We then subjected the search terms to explosion and critical evaluation using Medical Subject Headings (MeSH) to generate keywords for the search strategy. Finally, we employed the resulting keywords for each database search. An example is provided in Table 2.
- Inclusion and Exclusion Criteria
- The SPIDER framework facilitated the process of determining inclusion and exclusion criteria [32]. First, key search terms were defined. “Social media” referred to online platforms that utilize Web 2.0 technology to enable the creation and exchange of user-generated content across a variety of communication activities, supporting user interactions [1]. “Health communication” pertained to the dissemination of health messages aimed at influencing behavior change within the realm of health [33]. A “pandemic” was characterized as an emerging infectious disease with rapid international spread among humans, where no prior immunity existed [4]. Out of the 6 diseases declared as PHEICs in the past 20 years, poliomyelitis and monkeypox were excluded. These diseases did not meet the definition of a pandemic, as they were not new at the time of the outbreak and had existing vaccines [7,34,35]. The remaining 4 diseases—coronavirus disease 2019 (COVID-19), Ebola, H1N1 influenza, and Zika—met the definition of a pandemic. Middle East respiratory syndrome and severe acute respiratory syndrome (SARS) were also included in our list, despite not being declared as PHEICs by the WHO [7], because they met the definition of a pandemic (Table 1) [4]. The SARS outbreak occurred before the 2007 revision of the International Health Regulations by the WHO and the introduction of the “PHEIC” term [5]. Thus, the WHO termed SARS “a worldwide health threat” [36].
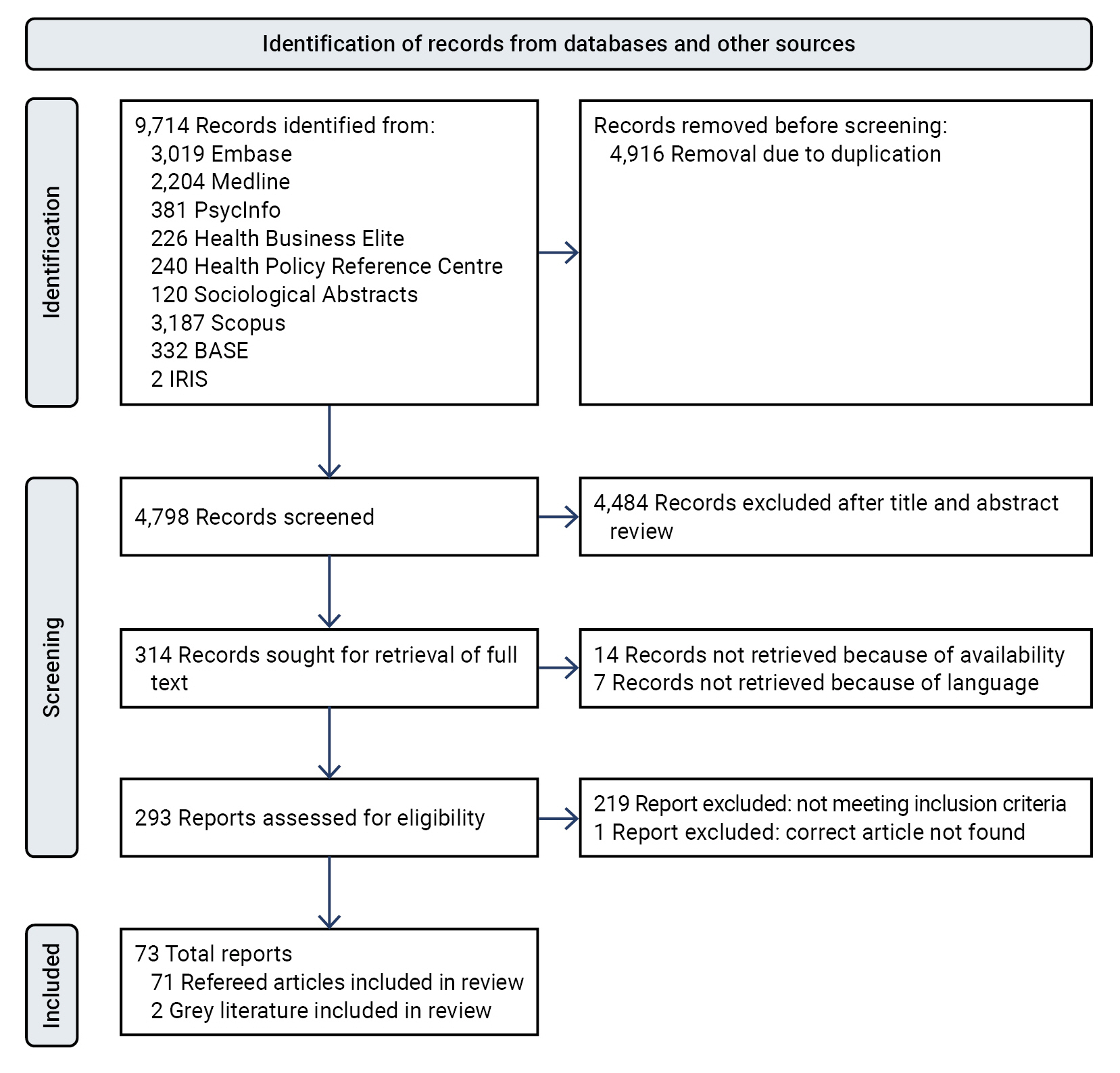
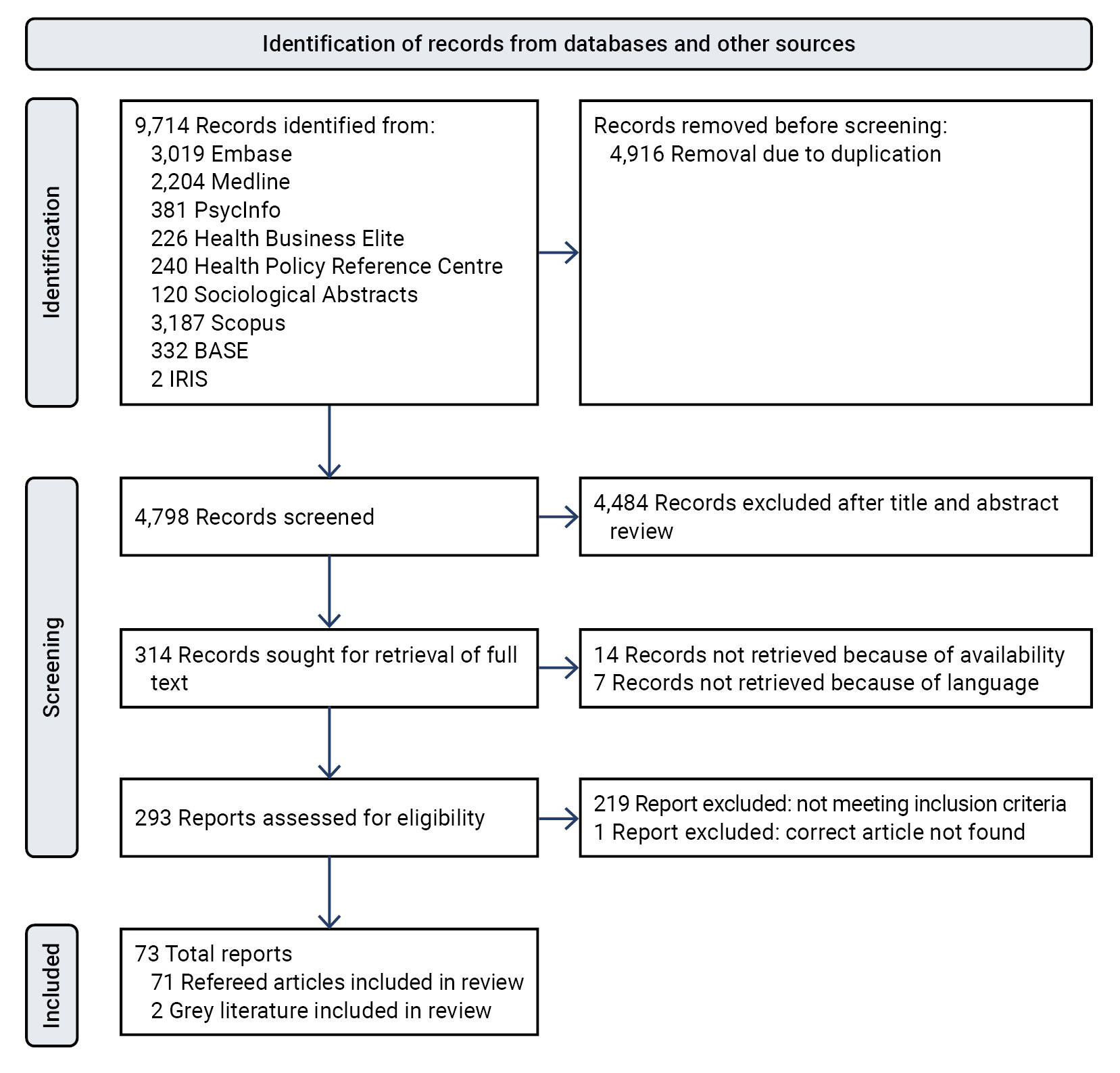
- After finalizing our definitions, we established the following inclusion criteria: full-text publications in English, evaluations of health messages from PHAs posted on their social media accounts focusing on acute communicable diseases of pandemic proportions, and publications between January 2003 and August 2022. Our initial database searches yielded 4,208 non-duplicated papers. After applying the inclusion and exclusion criteria, 73 eligible papers were selected for the scoping review. The first author conducted the stepwise process, while the other 4 authors reviewed each step and addressed discrepancies. Figure 1 presents the flowchart in accordance with the PRISMA-ScR guidelines [31]. The first author served as the primary coder, extracting variables that influenced the effectiveness of PHAs’ health messages on their social media accounts during pandemics from the full text of the 73 eligible papers. These variables were then integrated into sub-themes and further aggregated into themes. The second author independently coded 10% of the studies at random to ensure consistency. All remaining authors reviewed the codes to confirm reliability. Consequently, an iterative approach involving independent work and group discussions was employed to eliminate individual bias and enhance data validity.
Materials and Methods
- Characteristics of Included Studies
- The resulting records included 71 peer-reviewed papers and 2 pieces of grey literature (Figure 1) [31]. Only 25% of the studies were published within the first 10 years of research output (Table 3). The remaining 75% were published in the last 3 years, coinciding with the COVID-19 pandemic. Three other pandemics covered by the studies were Ebola, Zika, and H1N1. The relative number of publications for each pandemic corresponded to the duration of their PHEIC status (Table 1) [4]. The publications originated from 18 countries, with approximately half coming from the United States of America (USA). China, Canada, and Singapore were other significant contributors, while countries from Africa, Europe, Oceania, and South America were less represented. These publications examined the social media public health communication activities of PHAs in 42 countries. The USA was the focus of 32 studies, either partially (n=5) or entirely (n=27), while 27 countries were each the subject of no more than 1 study. The WHO was analyzed in 15 studies, and 12 studies compared multiple countries. Twitter and Facebook were the primary social media sources of research data, with 76% of the studies relying exclusively on one or the other. Twitter was included in all 7 studies that utilized data from multiple social media platforms. Single-method studies, either quantitative (42%) or qualitative (37%), were more common than mixed-method studies (21%). Of the 22 papers analyzed, 30% employed a theoretical framework or approach for their study, with the crisis and emergency risk communication (CERC) model being the most prominent (Table 4) [15,18,27,29,37−54].
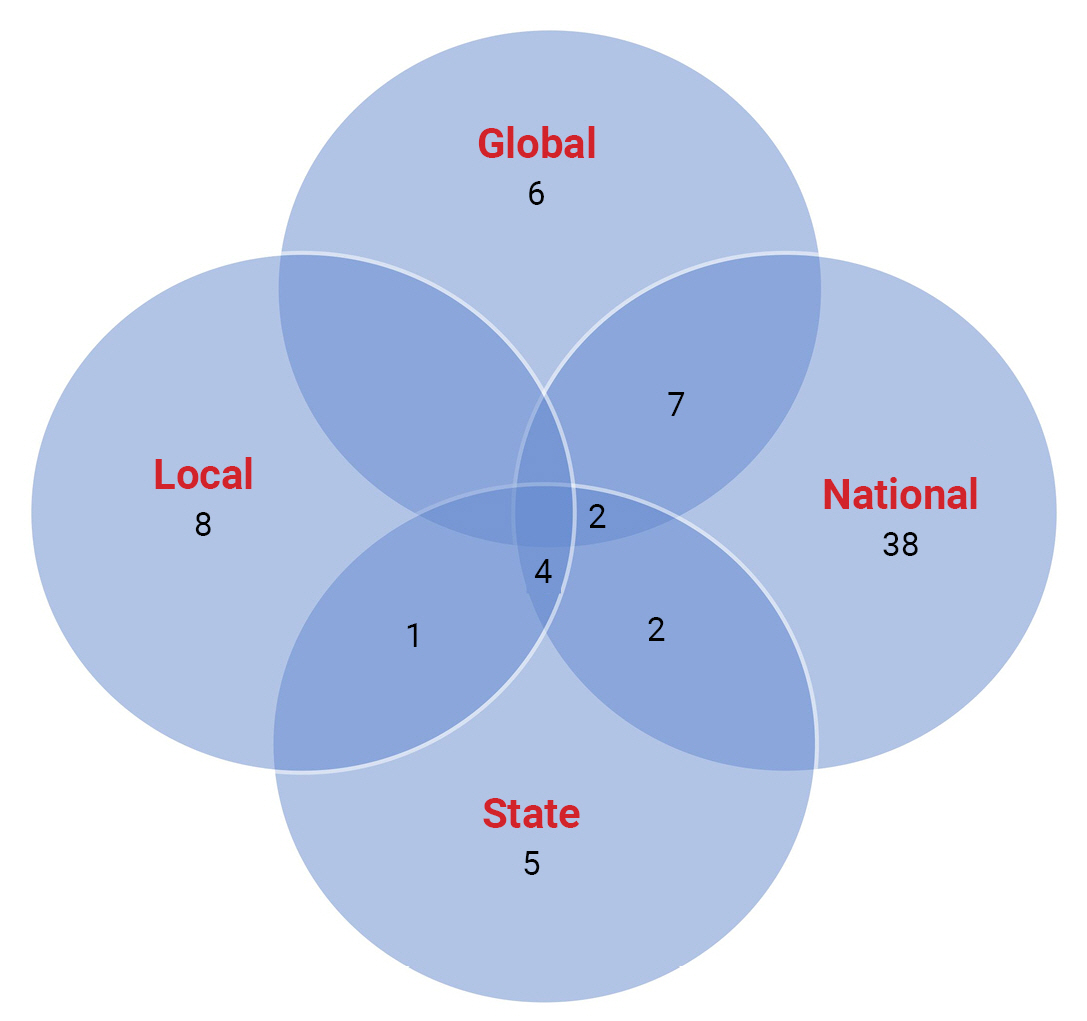
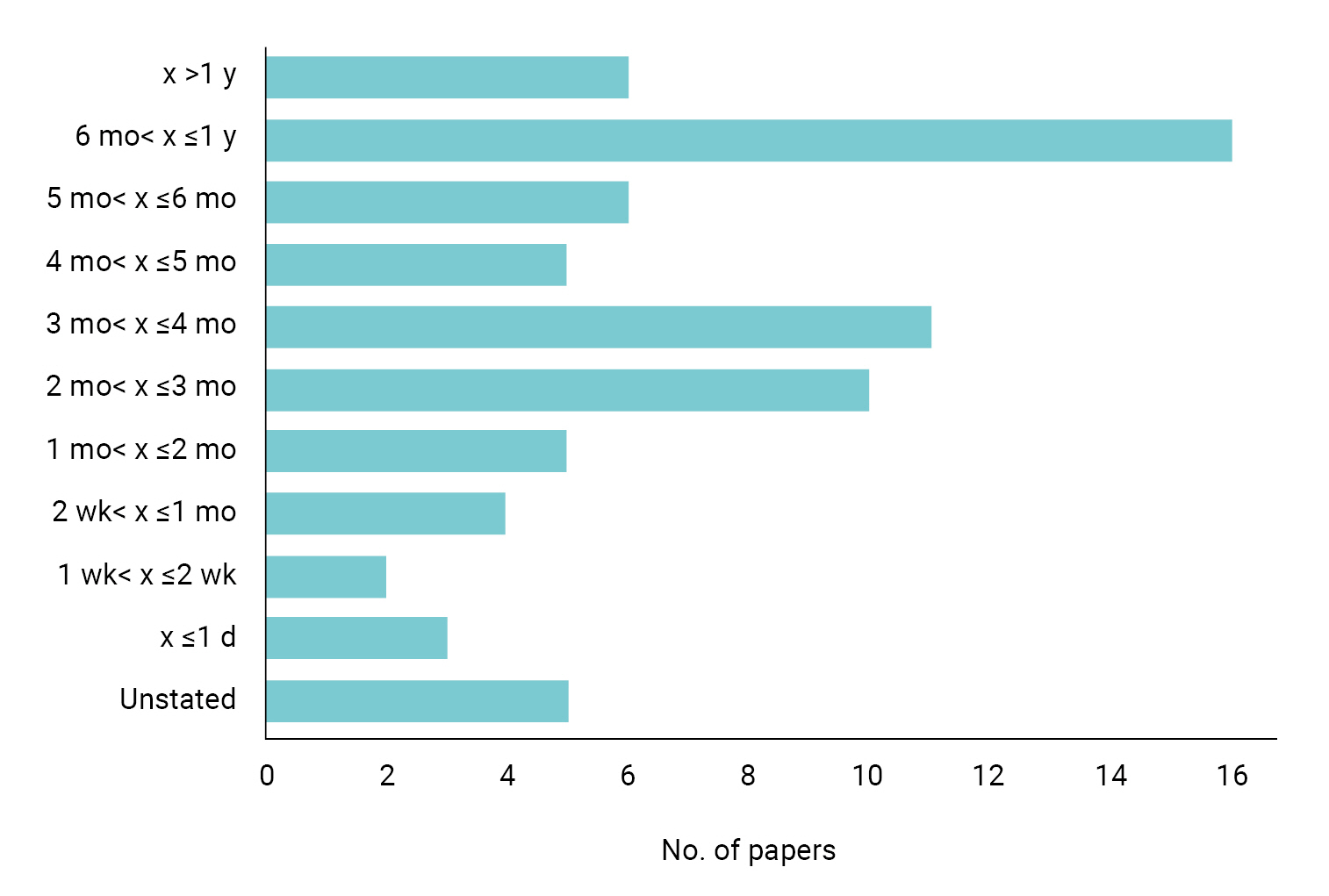
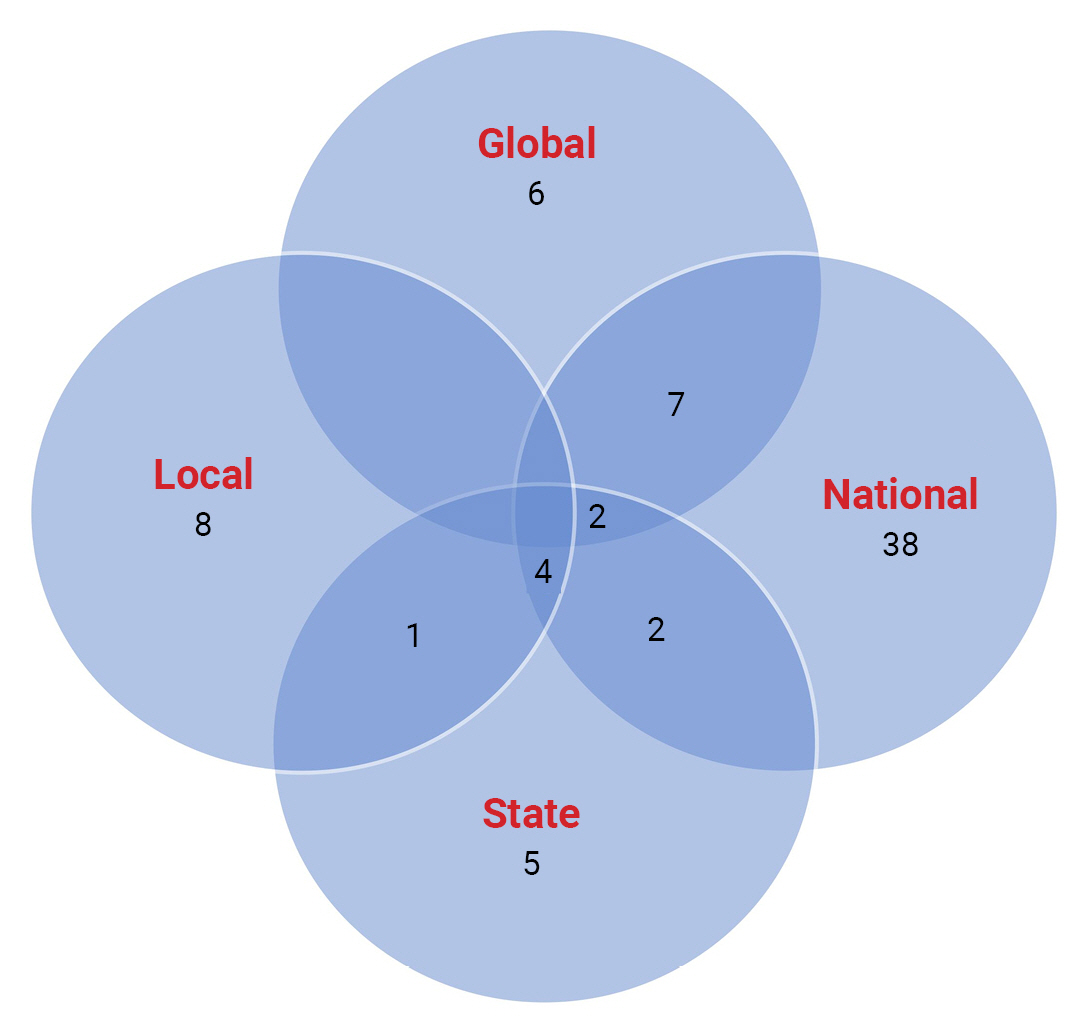
- A wide diversity is evident in the volume of social media data used in the studies (Table S1). Some studies analyzed only tens of health messages, while others examined thousands. The health messages studied ranged from low-media-styled posts (plain text) to high-media-styled posts (videos, infographics, and photos). Fifty-seven papers (78%) assessed PHAs at 1 of the following levels: global, national, state, or local (Figure 2). National-level PHAs were the most studied, with 52 papers in total; 38 of these focused solely on that level, and 14 compared them with PHAs belonging to other levels. Local-level PHAs were the least studied, involving 13 papers, 1 fewer than state-level PHAs. Only 4 papers examined PHAs’ social media health messages across all tiers of government in a country. Thirty-one papers studied 1 PHA each, while 42 studied multiple PHAs; 12 of these papers focused on PHAs from multiple countries (Table 5). The United States’ Centers for Disease Control and Prevention was the most studied PHA, followed by the WHO (Table S1). There was also a wide variety in the timeframe of social media data used in the studies (Figure 3). The most prevalent range was 2 to 4 months (28%), followed by 6 to 12 months (22%). Half of all the studies fell between both timeframes. Twenty-one studies (29%) based their timeframes on the period surrounding a PHEIC or national health emergency declaration. The assortment of PHAs studied, pandemics of interest, social media data volume, and data timeframe in the reviewed papers underscore the plurality of researchers’ scope and attention.
- Variables Influencing PHAs’ Social Media Health Messaging during Pandemics
- A total of 20 variables were identified as playing a role in the effectiveness of PHAs’ use of their social media accounts to communicate relevant health messages during pandemics, based on the 73 reviewed studies. These variables were grouped under 6 broad themes: the origin of health information, the topic addressed, the semantics and style of messaging, the timing of messaging, the diversity of platforms and audience profile, and the credibility and reliability of message content (Table 6). The findings are further explained below, followed by a review of implications for practice and future research.
- Origin of Health Information
- Sixty-two selected papers (85%) examined variables related to the reputation, internal players, and strategies of PHAs. Four sub-themes emerged under the sender of health information—namely, the status, tactics, policies, and personnel of PHAs.
- The status of having a track record in pandemic management was found to be critical to a PHA’s effectiveness when using social media to communicate health messages during a pandemic [55−59]. PHAs were perceived by the public as high-impact organizations that should serve as the primary source of health information during pandemics [60−62]. To ensure the effectiveness of social media health messages, there must be no ambiguity regarding which PHA in a country or territory is the authorized information source [63]. An absence of ambiguity enabled PHAs to act as agenda-setters on social media for both other PHAs and the public. These agenda-setters occupy strategic network positions, which amplify the reach of their health messages and generate widespread public engagement as other PHAs share the messages with their own followers [25,51]. PHAs that have earned public trust tend to be more effective in disseminating health messages during pandemics than those with a trust deficit [39,64,65]. Not only should PHAs be trustworthy, but they should also actively work to build mutual trust [47].
- Nimble tactics also influenced PHAs’ effectiveness. To increase their reach within their jurisdiction, PHAs adopted multilingual health messages [14,15,66]. They also utilized appropriate terminology in their messages [67] and offered advice using culturally fitting strategies [54,68]. PHAs featured diverse personalities as subjects or spokespersons on their social media channels, such as social media influencers [14,40,69], celebrities [70,71], medical personnel [72], political leaders [73], or victims sharing personal experiences [42,72]. Another tactic was “attribution of responsibility,” which negatively labelled non-conforming members of the public [67,74]. At other times, PHAs sometimes opted for “ethical disengagement” [10] as a means of enhancing the effectiveness of its messages. PHAs also collaborated by sharing one another’s health messages [25,51]. The tactics implemented by PHAs enabled them to disseminate their messages to various special populations and target audiences.
- In-house social media policies providing guidelines have been shown to influence the characteristics and effectiveness of health messages shared by PHAs during pandemics [49,75]. Policy frameworks for PHAs were helpful in setting goals and strategies, as well as identifying the target audience for its social media health communication. Twenty-nine studies discussed 17 guidelines that PHAs followed to create and share health messages on social media. Among these guidelines, the most prominent focused on emphasizing the transmission of health messages [17,26,69], fostering public interaction and engagement [10,37], and expressing empathy to those directly affected by pandemics [27,29]. PHAs were also encouraged to put risks into proper perspective [12,68], promote transparency of information and efforts [49,65], and be timely [38]. Utilizing multiple social media platforms was found to be valuable in effectively reaching a larger audience [18], while members of the public could be recognized as advocates and partners in the co-creation and dissemination of health messages [49,55]. If necessary, PHAs could discontinue further interaction with any member of the public [10,26]. However, Chen et al. [46] noted that adhering strictly to guidelines without flexibility could hinder effective social media messaging for PHAs.
- Nine studies shed light on the impact that the personnel in charge of PHAs’ social media accounts could have on the effectiveness of health messages shared during pandemics. Possessing expertise in areas such as journalism, public information management, or public health was associated with enhanced quality of PHAs’ social media health messages [26,75,76]. These professionals demonstrated a greater aptitude for employing appropriate strategies to develop and distribute content on behalf of PHAs. However, disclosing the identity of these individuals could be detrimental if they have had a negative past with the public [24]. Alongside the personnel’s ability to perform their jobs, emphasis was placed on providing them with the necessary digital tools and equipment [75].
- Topical Issues Addressed
- Sixty-two selected papers (85%) examined variables related to the general message topics of PHAs. There was considerable diversity in how PHAs framed their social media health messages during pandemics [63,77]. The 6 categories within the subject of messages comprised education, government efforts, collaboration, news updates, misinformation, and supplementary messages.
- Education dealt with PHAs’ health messages that aimed to raise public awareness about the risks associated with pandemics [46,53,78]. These messages offered specific insights into disease mechanisms, as well as preventive and safety measures that individuals should adopt [44,79,80]. Public consciousness was heightened regarding pandemic epidemiology, accompanied by recommendations on preventive strategies to prevent both community and hospital transmission [63,72]. This educational approach successfully captured public attention. Topics addressed included the use of personal protective equipment [24,52,63], vaccination and vaccine hesitancy [55,72], lockdowns, isolation, and physical distancing [45,51,73], personal sanitation [68,77], routine immunological testing [41,66], and contact tracing [29,73].
- Government efforts to implement public health policies, enhance healthcare delivery, initiate or sponsor epidemiological studies, announce significant scientific breakthroughs, and modify the usual social and economic order comprise another category of health messages [27,29,52,53,59,67,68,77,81−83]. The extent to which this information was communicated impacted the effectiveness of these messages. Regular updates on government actions provided the public with incremental knowledge, offering reassurance during the uncertainties of pandemics [29,71]. These messages reflected the preparedness of governments at all levels [76]. Consequently, the public was eager to discuss and share these messages with other social media users [52,81]. Health messages of this nature maintained high public engagement throughout all stages of a pandemic [27,81,84].
- PHAs’ health messages also encouraged active public collaboration in efforts to combat pandemics by soliciting philanthropic donations of personal resources, including time, skills, and funds [50,79,81]. Utilizing local and international collaborations provided the solidarity PHAs needed to drive their narratives [12,44,68]. Other messages expressed appreciation to donors and contributors [37,82], with special mentions for healthcare workers [78,83], and construction workers [29]. PHAs’ tendency to acknowledge the concerted efforts of the public during pandemics influenced the effectiveness of their health messages, as people were more likely to like and share the messages [27].
- News updates were identified as another prominent feature of PHAs’ social media health messages [14,78]. These messages aim to inform the public about the changing pandemic indices by providing real-time information on morbidity and mortality cases, as well as other related data [27,56,64] and the latest updates on hospital services [76,82]. Health messages often came in various forms, such as broadcasts of press conferences [37,63,76,81,85]. Framing health messages as news enables the public to gain situational awareness of a pandemic as it unfolds. However, not all PHAs utilized this approach, which may hinder the effectiveness of their health messages within their jurisdiction [76].
- PHAs also shared health messages on their social media accounts to combat the spread of misinformation and fake news that incited panic among social media users [18,26,64,86]. They raised the public’s awareness on how to avoid falling for misinformation [14,37] and corrected false information when necessary [10,87]. However, in many cases, inaccurate information from unverifiable sources was disseminated more widely by irresponsible social media users than the accurate health messages provided by PHAs [88]. In some instances, even reliable government sources inadvertently shared incorrect information [12]. The dedication of PHAs to addressing uncertainties and clarifying inaccurate health information played a major role in the effectiveness of their social media messaging during pandemics.
- Finally, PHAs also posted messages unrelated to the ongoing pandemic [15,67,83]. Often, PHAs were slow to respond at the beginning of a pandemic, as evidenced by the predominance of non-pandemic messages in their social media communications [48,62,67,88]. However, when compared to messages not related to the pandemic, those addressing the pandemic were read by more people, and readers spent more time engaging with them [37,48,62]. It remains unclear why PHAs hesitated to increase their pandemic-related messaging in response to the public’s growing information needs during outbreaks. It appears that PHAs may be uncertain about what information to share at the onset of pandemics [83].
- Structure and Style of Messaging
- Fifty-five papers (75%) examined variables that focused on the structure, style, and supplementary elements of the messages of PHAs. The 3 resulting sub-themes were the dialogic tools, media richness, and message tone of PHAs.
- Dialogic tools refer to elements incorporated into social media health messages that facilitate engagement and interaction between the sender and the audience [27]. The presence of dialogic tools in PHAs’ health messages influenced the effectiveness of those messages. Hashtags and hyperlinks were the most commonly used dialogic tools by PHAs [39,41,62]. For example, the use of hashtags was associated with higher levels of public engagement while the opposite was true for hyperlinks [15,53]. When both were combined in a post, public engagement levels increased [76]. Health messages featuring multiple dialogic features tended to garner more engagement than those with a single feature [46]. Higher-level PHAs often used hyperlinks to direct their audience to their own websites for more information [41], but state-level PHAs preferred to send their audience to the websites of federal-level PHAs and other reputable organizations [42]. Although PHAs used dialogic tools in various ways, they generally used such tools to collaborate, which in turn reinforced one another’s messages [25,56,63,89]. This approach effectively demonstrated the coherence of the views of different PHAs on the same issue. Other dialogic tools used less frequently by PHAs included the @ mention function, question and exclamation marks, live chats, reply, forward, and quote functions [46,52,53,76,87]. These tools were effective to varying degrees in generating public engagement with health messages. The public’s perception of the effectiveness of health messages is related to the degree to which 2-way communication is accommodated [60,90]. Two-way communication benefitted the public by promoting consensus building and mutual trust [10,27].
- Media richness refers to the ability of a message to generate shared meanings and facilitate smooth interactions between the sender and receiver of the message [46]. Generally, health messages with high media richness were less likely to engage users on text-oriented platforms like Twitter and Sina Weibo [46]. However, combining images with plain text can increase public attention [56]. Infographics and pictures were the commonest media enrichment tools used by PHAs [56,68,70]. The current pandemic phase at the time of infographic development influenced their design and layout [91]. Factors such as the choice of background colors, the language used, and the personality presented in the image were all subtle but influential elements of graphics and pictures incorporated into PHAs’ health messages [40,92]. Higher-level PHAs further enriched their health messages (e.g., by using videos) more frequently than lower-level PHAs [92]. As with infographics, PHAs had different options for creative video styles to adopt for their health messages, ranging from animations to live-action videos [63,89]. More creative videos were more effective. Factors such as video duration, tone, and title length significantly influence the effectiveness of health messages in generating public engagement [14,63,84]. However, engagement levels with videos were lower than with plain text on text-oriented social media platforms such as Twitter [15], WeChat [82], and Sina Weibo [46].
- The choice of message tone was another sub-theme. As the language used on social media tends to be more similar to spoken communication rather than written, the effectiveness of PHAs’ health messages was related to the extent to which the messages exhibited a conversational tone [38,39,47]. PHAs, however, typically adopted either an authoritative formal tone or an interactive informal tone [47,54]. PHAs were more likely to use a formal tone in their social media messaging when emphasizing guidelines, instructions, and warnings [68]. Although the public often perceived PHAs’ formality negatively as mere grandstanding, certain situations, such as addressing misinformation, made the formal stance non-negotiable [10,18]. Conversely, when informality, cordiality, and humor were incorporated into health messages, public engagement increased with more views and reactions [69]. In the same vein, PHAs may choose to convey positive, negative, or both tones in their messaging. Positive messages tend to focus on solutions, while negative messages can dampen public morale [56,72]. The more positive a health message is, the more engaging it becomes. Message tone also involves communicating emotion-laden cues to which the public responds [67,84]. The emotional valence of PHAs’ health messages influences their effectiveness in triggering public sentiments, emotional support, diffusion, and engagement [58,67,84,93].
- Diversity of Platforms and Audience Profile
- Fifty selected papers (68%) examined variables related to the reach of PHAs’ health messages to the public, with an emphasis on the subscribers and followers of the social media accounts of PHAs. This theme was consolidated from 2 sub-themes: community and platforms.
- During pandemics, the followership of PHAs’ social media channels consistently increased as people sought health messages from authentic sources [18,26,42,57,62]. Higher-level PHAs with broader jurisdictional coverage tended to attract more followers than lower-level PHAs [48]. PHAs established social media accounts on platforms where their target audience was most likely to be found [83,91]. The geographic location of a PHA played a role in distinguishing its audience characteristics from those of other PHAs [10,14,42]. However, each PHA had to contend with diverse audience profiles in terms of demographic features [17,38,39,57,63,64]. PHAs tailored their health messages to specific target audience profiles and social media channels [40,49,56,70,94]. The engagement patterns of the audience also tended to influence subsequent messaging from PHAs [44,48,63,95].
- Accessibility to social media platforms within a PHA’s jurisdiction encourages users to engage with the PHA’s social media channels. The most popular social media accounts for PHAs were found on Facebook, followed by Twitter, across various regions and countries, including Anglophone Africa [14], the USA [42,48,57,65,71], Italy [27,70], Canada [38,39,62], New Zealand [27], the United Kingdom [27,71], Denmark, Norway, and Sweden [10], Singapore [71], and for the WHO [55,65]. Twitter provided the most connections to PHAs’ social media accounts in India [73]. Sina Weibo was the most popular in China, followed by TikTok [46,53,82,84]. Despite YouTube’s ubiquity, few users connected with PHAs’ social media accounts on the platform [14,63,89]. Channel popularity did not always correlate with PHA usage. For example, while a large Facebook following prompted health communication by PHAs in Singapore and Macao [49,81], the less popular Twitter was more frequently used by PHAs in the USA [49,57,78,88] and Africa [14]. Nevertheless, PHAs often used multiple platforms to share their health messages [56,85], as each social media platform exhibited unique characteristics [15,81,94] and [14] supported public engagement differently [41,85,94].
- Timeliness and Relevance
- Forty-nine selected papers (67%) investigated variables associated with the relevance of health messages from PHAs at the time of delivery. This theme encompassed 2 sub-themes: pandemic milestones and phases, as well as message frequency.
- PHAs recognized certain milestones or new developments during a pandemic, such as the announcement of a PHEIC, during which health information demand is highest [37,45]. Notwithstanding, while some PHAs posted the preponderance of their pandemic-related health messages around these landmark events [52,60,70,94], others shared a disproportionately small volume of information [42]. When PHAs trended together with pandemic-related events, their health messages were highly effective in attracting public engagement [43,62,71] and generating diverse emotional reactions from the public [67]. Conversely, Madvig et al. [26] and Lwin et al. [29] reported no consistent relationship between PHAs’ health message volume during landmark pandemic-related events and the level of public engagement.
- The pandemic phase during which PHAs shared health messages could influence the effectiveness of messaging [81]. Pandemics can be segmented into phases based on the disease progression in the community. However, there was no shared basis for this segmentation in the literature, and the number of phases was presented as 5 [15,29,37], 4 [51,59,81,83] or 3 [65]. Ahmed et al. [79] and Radwan and Mousa [68] restricted the segmentation to the lockdown period only. PHAs’ pandemic-related health messages varied with pandemic phases, irrespective of the segmentation type adopted [15,83]. The volume of messages and the range of topical issues addressed were lowest during the prodromal phase, but rose significantly when the first pandemic cases were reported [14,15,59,63,81,83,88]. However, despite the higher volume of messages, certain population groups were often not targeted [96]. Batova [24] attributed this apparent oversight to PHAs’ limited knowledge about pandemics during the early stages of an outbreak.
- Early messaging from PHAs following an outbreak was helpful in guiding the public [41,62], although such messaging was often delayed until a sharp increase in cases occurred [14,76,78]. Frequently, the content of these health messages did not meet the public’s information needs [59,80,83], which evolved with the different phases of the pandemic [29]. There were instances when the messaging from PHAs did not align with the rate of disease spread, rendering the messages less relevant to the audience [88,97]. Within the same pandemic phase, individual PHAs shared health messages on topics they deemed appropriate [79] or established common ground with other PHAs [51]. The posting of conflicting messages from different PHAs was widespread during the early phases of pandemics, but coherence and collaboration gradually became more evident as pandemics progressed [77]. With social media, PHAs could communicate at the public’s most preferred times of the day [64,76,98], resulting in a wider reach for well-timed communication strategies. Similarly, maintaining a regular frequency of health messaging [37,56] allowed the public to build trust and confidence in the activities of PHAs.
- Content Credibility and Reliability
- Forty-five selected papers (62%) investigated variables related to the credibility and reliability of health messages conveyed by PHAs. Within these studies, 3 sub-themes were identified: congruence, transparency, and consistency of the messages.
- Congruence refers to the extent to which PHAs display consistency in content and context within their pandemic-related health messages. This is particularly crucial for PHAs operating within the same jurisdiction or catering to the same audience. Incongruence among PHAs is not uncommon during pandemics, as situations continually evolve [65,77,91]. Instances of incongruence have been observed in message volume, the selection of topics addressed, and the timeliness of addressing issues by different PHAs [14,27,40,47,65,79,89,95−98]. For example, PHAs’ health messages addressed misinformation differently during the COVID-19 pandemic [71]. Incongruence can lead to varying levels of public emotional diffusion across PHAs [93]. Dissonance among PHAs negatively affects the public’s response to conflicting health messages, while congruence has the opposite effect [77]. Sharing health messages with similar themes at comparable times and frequencies, as well as referencing one another, indicated coordination and collaboration among PHAs [25,51].
- Health messages from PHAs could be perceived to be insufficiently transparent and objective [74,91]. The transparency of PHAs was called into question when they faced a deficit in public trust, as evidenced by fear-inducing health messages that suggested hidden motives related to financial gain, corruption, conspiracy [24,58,60,85] or political interference [26]. Health messages that are perceived as non-transparent often prompt public responses calling for PHAs to be more forthright. However, message transparency could be hindered by the public’s level of scientific literacy [72]. The public frequently associates transparency with the jurisdictional level of PHAs [50,53]. Nevertheless, PHAs at all levels have the potential to exhibit transparency, which can influence the effectiveness of their pandemic-related health messages [98].
- The consistency of opinions expressed in PHAs’ pandemic-related health messages was another influential factor. Perceived inconsistency diminished the relevance of PHAs’ health messages to the public [18,24,26,39,77]. Inconsistency and ambiguity in PHAs’ communication of pandemic-related risks arose when successive health messages continually shifted, leading to public anger and criticism [18,24,77,86]. This caused some individuals to become more anxious, while others downplayed the risks [48]. Since PHAs’ health messages did not consistently address the public’s concerns, the resulting demand-supply mismatch undermined the effectiveness of their health messages [37,47,59,80,83].
Results
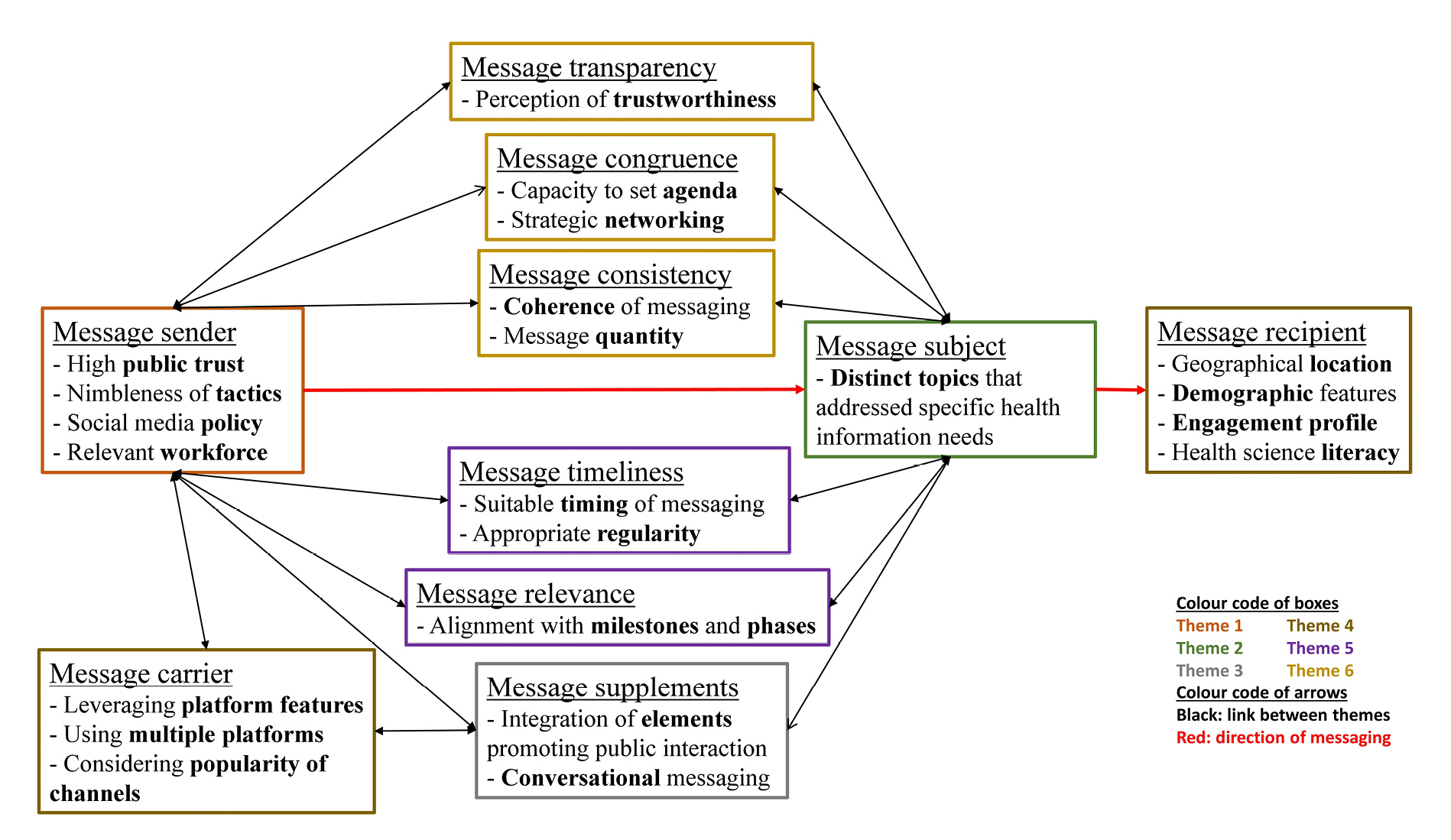
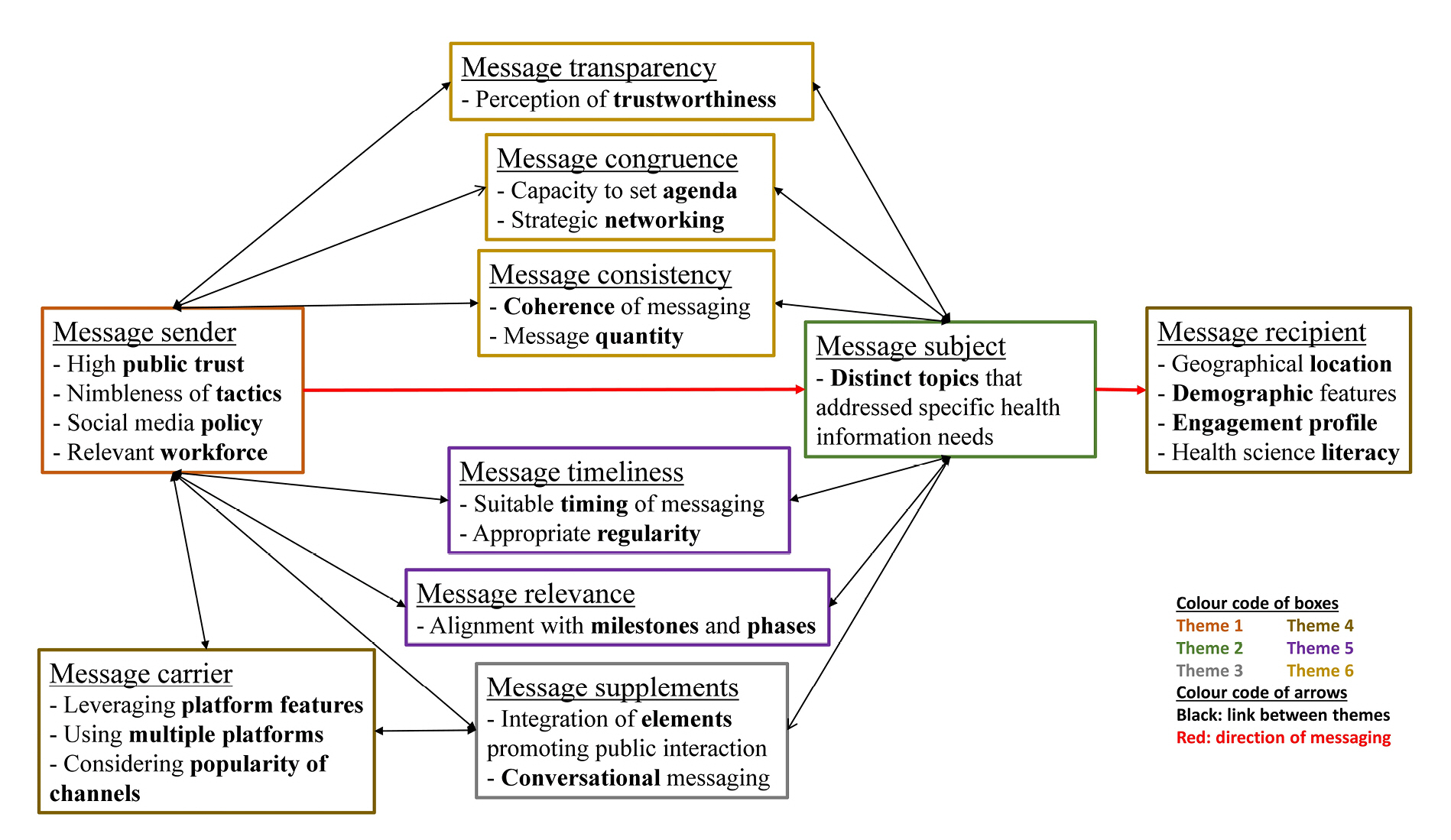
- This review examined the evidence in the literature concerning PHAs’ use of social media for disseminating public health messages during a pandemic and assessed the resulting public engagement. Twenty key factors were identified for PHAs to consider when using social media for health communication during a pandemic. These 20 factors (sub-themes) were then grouped into 6 overarching themes. The review highlighted the interconnections between the themes and sub-themes, which work together to enhance effective public engagement via PHAs’ social media accounts. This ecosystem is encapsulated in a conceptual model, which is displayed in Figure 4.
- Even though pandemics have different courses (Table 1) [4], this literature review has identified general criteria that can guide PHAs in crafting pandemic-related health messages for their social media accounts. PHAs create and disseminate messages on diverse topics, tailored to audiences with differing locations, demographics, engagement profiles, and health literacy levels. In developing these messages, PHAs rely on their inherent factors, such as trust capital, social media policies, tactics, and skilled personnel, to fulfill their communication responsibilities. For example, the absence of internal social media policies for PHAs impeded effective health communication activities on social media during the pandemic [67,75]. However, PHAs’ intrinsic factors were not the sole determinants of effective messaging, as they were also influenced by other variables within the ecosystem. For instance, a recipient could be a contributor, promoter, or champion. Contributors frequently interacted with PHAs’ health messages, often as detractors, while champions engaged less frequently but typically as advocates and partners of PHAs [48,55]. Each category of recipient perceived pandemic-related health messages differently and engaged accordingly [50,73]. They evaluated the messages based on relevance, transparency, congruence, consistency, timeliness, and tone [40,47,52,82,92]. The public experienced various stages and milestones during pandemics, which continually affected the communication strategies of PHAs and the content of their health messages [15,29,37,59,65,68,81,83]. Consequently, PHAs needed to learn from the public’s engagement with previous messages before moving forward with new ones.
- Contribution to Theory and Practice
- The grounding of public health communication science and practice in social media theory is still in its early stages. This literature review discovered that only 22 studies (30%) employed a theoretical approach or framework for critical data analysis. Thirteen distinct theoretical frameworks were utilized, with the CERC model being the most prominent. The variety of theories applied indicates that they are still being tested in health communication research. This finding supports the arguments made by Hannawa et al. [99] and Hannawa et al. [100], who posited that empirical research in health communication lacked theoretical rigor and a clear epistemological approach, which are 2 essential components for framing practical solutions in the field.
- Only 1 study, by Vijaykumar et al. [49], discussed a framework. This framework, risk amplification through media spread (RAMS), was conceptualized as a potential tool to guide future public health communication activities of PHAs during pandemics. However, the framework was designed for the entire health communication spectrum, not social media only. Liu and Kim [67] called for further investigation into viable communication frameworks during pandemics. Pandemics and their associated effects typically last longer than most crises, which tend to be acute and have a more limited geographical spread. Conversely, Vijaykumar et al. [49] emphasized the importance of evaluating the ways in which social media efforts impact societal behavior during pandemics. It is not enough for PHAs to simply post health messages on social media; the influence on societal behavior should also be monitored and measured. This literature review proposes a conceptual model (Figure 4) that could serve as a foundation for additional research into social media health communication by PHAs during a pandemic.
- Research Gaps: Directions for Future Research
- Each successive pandemic of the 21st century has increasingly exposed the gaps in social media health messaging by PHAs [14]. The year 2003 marked the beginning of the social media revolution as we know it today [3]. SARS, the first pandemic recorded in the social media era [2], occurred the same year [36]. This scoping review found no evidence that any PHA used social media platforms for relevant communication during SARS. As social media was still in its infancy [3], PHAs would not have considered it as an option for their public health communication. The next pandemic, H1N1 [5,7], presented a different narrative. Three studies [49,67,75] revealed that PHAs utilized their social media channels to communicate pertinent health messages about the pandemic. However, these studies focused solely on the USA. By the time of the most recent pandemic, COVID-19, studies have covered 42 countries to varying extents (Table 3). Consequently, there is a gap in knowledge about the situation in many countries during a pandemic. Likewise, there are gaps in understanding how social media platforms can be effectively used. This literature review identified 7 social media platforms that were used for study purposes. However, there are over a hundred other social media platforms where the public gathers and health communication circulates. PHAs cannot afford to overlook such platforms.
Discussion
- This scoping literature review aimed to identify and synthesize the variables that influence the effectiveness of PHAs health messages on their social media accounts during pandemics. Our review categorized these variables into 6 themes: origin of health information, topical issues discussed, structure and style of messaging, timeliness and relevance, content credibility and reliability, and diversity of platforms and audience profiles. These factors can be considered by PHAs when using their social media accounts for effective pandemic-related health communication. However, we identified a significant research gap in determining the relative importance of these variables. Furthermore, the existing theoretical frameworks in the studies examined were insufficient in addressing this gap. We have proposed a conceptual model to hypothesize the interconnectedness of these variables and advocate for more research to provide insight, as PHAs need to be better equipped in health communication for potential future pandemics.
Conclusion
- • During pandemics, the public has a multitude of communication needs and expectations that public health agencies grapple with, as they face an avalanche of misinformation on social media.
- • Public health agencies must uphold public trust in their social media communications, despite the initial knowledge gaps and constantly changing dynamics that are characteristic of pandemics.
- • Effective audience engagement can be achieved by public health agencies sharing relevant, timely, and persuasive pandemic-related health messages on social media.
- • Six overarching themes define how public health agencies can enhance the efficacy of their health messages through their social media accounts during pandemics.
HIGHLIGHTS
Supplementary Material
Table S1.
-
Ethics Approval
Not applicable.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Availability of Data
All data generated and analyzed during this study are included in this published article. Other data may be requested through the corresponding author.
-
Authors’ Contributions
Conceptualization: all authors, AH; Design: all authors; Methodology: all authors; Supervision: AH, NK, LY, MA; Literature review: BAB, AH; Validation: all authors; Visualization: BAB; Writing–original draft: BAB; Writing–review & editing: all authors. All authors read and approved the final manuscript.
-
Additional Contributions
The authors are grateful to the librarians at the University of Tasmania who provided guidance on the use of the SPIDER tool and electronic database search.
Article information


| Serial no. | Infectious diseases |
PHEIC status |
Pandemic statusa) | ||
|---|---|---|---|---|---|
| Considered | Announced | Duration (d) | |||
| 1 | Poliomyelitis | Yes | Yes | 3,303 (ongoing) | No |
| 2 | COVID-19 | Yes | Yes | 1,192 | Yes |
| 3 | Ebola (first outbreak) | Yes | Yes | 600 | Yes |
| 4 | H1N1 influenza | Yes | Yes | 473 | Yes |
| 5 | Ebola (third outbreak) | Yes | Yes | 346 | No |
| 6 | Zika | Yes | Yes | 292 | Yes |
| 7 | Monkeypox | Yes | Yes | 293 | No |
| 8 | SARSb) | No | No | - | Yes |
| 9 | MERS | Yes | No | - | Yes |
| 10 | Ebola (second outbreak) | Yes | No | - | No |
| 11 | Yellow fever | Yes | No | - | No |
PHEIC, public health emergency of international concern; SARS, severe acute respiratory syndrome; MERS, Middle East respiratory syndrome.
a) The authors used the definition of Doshi [4] as a criterion.
b) SARS did not undergo a PHEIC evaluation as it predates the revised International Health Regulations policy of the World Health Organization. It was called “a worldwide health threat” instead.
| Theoretical frameworks used for data analysis | No. of studies |
|---|---|
| Crisis and emergency risk communication model [15,18,29,37−40] | 7 |
| Health belief model [41−45] | 5 |
| Media richness theory [46,47] | 2 |
| Social amplification of risks framework [48,49] | 2 |
| Agenda-setting theory [50] | 1 |
| Dialogic accounting framework [27] | 1 |
| Dialogic communication theory [46] | 1 |
| Disaster communication ecology framework [51] | 1 |
| Extended parallel process model [52] | 1 |
| Frame theory [53] | 1 |
| Mixed game model [54] | 1 |
| Public value theory [47] | 1 |
| Socially mediated crisis communication model [49] | 1 |
| Total | 25a) |
| Level of PHA |
Focus of study |
||
|---|---|---|---|
| Single PHA | Multiple PHAs (one country) | Multiple PHAs (multiple countries) | |
| Global | 4 | 7 | 4 |
| National | 24 | 19 | 10 |
| State | 0 | 14 | 0 |
| Local | 3 | 10 | 0 |
| Total | 31 | 30 | 12 |
- 1. van Osch W, Coursaris CK. Organizational social media: a comprehensive framework and research agenda. In: 2013 46th Hawaii International Conference on System Sciences; 2013 Jan 7-10; Wailea, HI, USA. IEEE; 2013. p. 700−7.Article
- 2. LeDuc JW, Barry MA. SARS, the first pandemic of the 21st century. Emerg Infect Dis 2004;10:e26.ArticlePMC
- 3. Lama UT. Understanding social media: functionality and differentiating social media and social networking sites. Int J Res Eng Appl Manag 2018;4:1−6.
- 4. Doshi P. The elusive definition of pandemic influenza. Bull World Health Organ 2011;89:532−8.ArticlePubMedPMC
- 5. Mullen L, Potter C, Gostin LO, et al. An analysis of International Health Regulations Emergency Committees and Public Health Emergency of International Concern designations. BMJ Glob Health 2020;5:e002502.ArticlePubMedPMC
- 6. Nuzzo JB, Borio LL, Gostin LO. The WHO declaration of monkeypox as a global public health emergency. JAMA 2022;328:615−7.ArticlePubMed
- 7. Wilder-Smith A, Osman S. Public health emergencies of international concern: a historic overview. J Travel Med 2020;27:taaa227. ArticlePubMedPDF
- 8. Institute of Medicine (US) Committee for the Study of the Future of Public Health. The future of public health [Internet]. National Academies Press (US); 1988 [cited 2023 Jun 24]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK218218/pdf/Bookshelf_NBK218218.pdf.
- 9. Knai C. What is public health? In: Thornbory G, editor. Public health nursing: a textbook for health visitors, school nurses and occupational health nurses. Wiley-Blackwell; 2009. p. 1–20..
- 10. Offerdal TS, Ihlen O, Just SN, et al. “We do not have any further info to add, unfortunately”: strategic disengagement on public health facebook pages. Int J Strateg Commun 2022;16:499−515.Article
- 11. Dickmann P, McClelland A, Gamhewage GM, et al. Making sense of communication interventions in public health emergencies: an evaluation framework for risk communication. J Commun Healthc 2015;8:233−40.Article
- 12. Munoz-Sastre D, Rodrigo-Martin L, Rodrigo-Martin I. The role of twitter in the WHO’s fight against the infodemic. Int J Environ Res Public Health 2021;18:11990. ArticlePubMedPMC
- 13. Adebimpe WO, Adeyemi DH, Faremi A, et al. The relevance of the social networking media in Ebola virus disease prevention and control in Southwestern Nigeria. Pan Afr Med J 2015;22(Suppl 1). 7. Article
- 14. Asubiaro T, Badmus O, Ikenyei U, et al. Exploring Sub-Saharan Africa’s communication of COVID-19-related health information on social media. Libri 2021;71:123−39.Article
- 15. Alhassan FM, AlDossary SA. The Saudi Ministry of Health’s Twitter communication strategies and public engagement during the COVID-19 pandemic: content analysis study. JMIR Public Health Surveill 2021;7:e27942.ArticlePubMedPMC
- 16. Ali ZS, Dang H. Factors impacting the use of the NZ COVID Tracer application in New Zealand. Smart Health (Amst) 2022;24:100278. ArticlePubMedPMC
- 17. Strekalova YA. Emergent health risks and audience information engagement on social media. Am J Infect Control 2016;44:363−5.ArticlePubMed
- 18. Dalrymple KE, Young R, Tully M. “Facts, not fear”: negotiating uncertainty on social media during the 2014 Ebola crisis. Sci Commun 2016;38:442−67.
- 19. Michel J, Rehsmann J, Mettler A, et al. Public health communication: attitudes, experiences, and lessons learned from users of a COVID-19 digital triage tool for children. Front Public Health 2022;10:901125. ArticlePubMedPMC
- 20. Ahmed N, Shahbaz T, Shamim A, et al. The COVID-19 infodemic: a quantitative analysis through Facebook. Cureus 2020;12:e11346.ArticlePubMedPMC
- 21. Lovari A. Spreading (dis)trust: COVID-19 misinformation and government intervention in Italy. Media Commun 2020;8:458−61.ArticlePDF
- 22. Battiston P, Kashyap R, Rotondi V. Reliance on scientists and experts during an epidemic: evidence from the COVID-19 outbreak in Italy. SSM Popul Health 2021;13:100721. ArticlePubMed
- 23. Greenhalgh T, Ozbilgin M, Tomlinson D. How COVID-19 spreads: narratives, counter narratives, and social dramas. BMJ 2022;378:e069940.Article
- 24. Batova T. To wear or not to wear: a commentary on mistrust in public comments to CDC tweets about mask-wearing during COVID19. Int J Bus Commun 2022;59:287−308.ArticlePDF
- 25. Kim HM, Saffer AJ, Liu W, et al. How public health agencies break through COVID-19 conversations: a strategic network approach to public engagement. Health Commun 2022;37:1276−84.ArticlePubMed
- 26. Madvig F, Achiam M, Adler-Nissen R, et al. Coming closer to citizens?: frustrated dialogue on the Danish Health Authority’s Facebook page during COVID-19. Front Commun 2022;7:822471. Article
- 27. Landi S, Costantini A, Fasan M, et al. Public engagement and dialogic accounting through social media during COVID-19 crisis: a missed opportunity? Account Audit Account J 2022;35:35−47.Article
- 28. Gesser-Edelsburg A, Stolero N, Mordini E, et al. Emerging infectious disease (EID) communication during the 2009 H1N1 influenza outbreak: literature review (2009-2013) of the methodology used for EID communication analysis. Disaster Med Public Health Prep 2015;9:199−206.ArticlePubMed
- 29. Lwin MO, Lu J, Sheldenkar A, et al. Strategic uses of facebook in Zika outbreak communication: implications for the crisis and emergency risk communication model. Int J Environ Res Public Health 2018;15:1974. ArticlePubMedPMC
- 30. Hagg E, Dahinten VS, Currie LM. The emerging use of social media for health-related purposes in low and middle-income countries: a scoping review. Int J Med Inform 2018;115:92−105.ArticlePubMedPMC
- 31. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 2021;372:n160. ArticlePubMedPMC
- 32. Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res 2012;22:1435−43.ArticlePubMedPDF
- 33. Morrison FP, Kukafka R, Johnson SB. Analyzing the structure and content of public health messages. AMIA Annu Symp Proc 2005;2005:540−4.PubMedPMC
- 34. Centers for Disease Control and Prevention (CDC). Polio vaccination [Internet]. CDC; 2022 [cited 2023 Jun 24]. Available from: https://www.cdc.gov/vaccines/vpd/polio/index.html#:~:text=There%20is%20no%20cure%20for,the%20United%20States%20since%202000.
- 35. World Health Organization (WHO). Mpox (monkeypox) [Internet]. WHO; 2023 [cited 2023 Jun 24]. Available from: https://www.who.int/news-room/fact-sheets/detail/monkeypox.
- 36. Enserink M. SARS: chronology of the epidemic. Science 2013;339:1266−71.ArticlePubMed
- 37. Fissi S, Gori E, Romolini A. Social media government communication and stakeholder engagement in the era of COVID-19: evidence from Italy. 2022. Int J Public Sect Manag 2022;35:276−93.
- 38. MacKay M, Cimino A, Yousefinaghani S, et al. Canadian COVID-19 crisis communication on Twitter: mixed methods research examining tweets from government, politicians, and public health for crisis communication guiding principles and tweet engagement. Int J Environ Res Public Health 2022;19:6954. ArticlePubMedPMC
- 39. MacKay M, Colangeli T, Gillis D, et al. Examining social media crisis communication during early COVID-19 from public health and news media for quality, content, and corresponding public sentiment. Int J Environ Res Public Health 2021;18:7986. ArticlePubMedPMC
- 40. Malik A, Khan ML, Quan-Haase A. Public health agencies outreach through Instagram during the COVID-19 pandemic: crisis and emergency risk communication perspective. Int J Disaster Risk Reduct 2021;61:102346. ArticlePubMedPMC
- 41. Guidry JP, O'Donnell NH, Meganck SL, et al. Tweeting a pandemic: communicating #COVID19 across the globe. Health Commun 2022;May 5 [Epub]. https://doi.org/10.1080/10410236.2022.2071192.Article
- 42. Laestadius LI, Guidry JP, Bishop A, et al. State health department communication about long COVID in the United States on Facebook: risks, prevention, and support. Int J Environ Res Public Health 2022;19:5973. ArticlePubMedPMC
- 43. Sesagiri Raamkumar A, Tan SG, Wee HL. Use of health belief model-based deep learning classifiers for COVID-19 social media content to examine public perceptions of physical distancing: model development and case study. JMIR Public Health Surveill 2020;6:e20493.ArticlePubMedPMC
- 44. Tang L, Liu W, Thomas B, et al. Texas public agencies’ tweets and public engagement during the COVID-19 pandemic: natural language processing approach. JMIR Public Health Surveill 2021;7:e26720.ArticlePubMedPMC
- 45. Tan SG, Sesagiri Raamkumar A, Wee HL. Users’ beliefs toward physical distancing in Facebook pages of public health authorities during COVID-19 pandemic in early 2020. Health Educ Behav 2021;48:404−11.ArticlePubMedPDF
- 46. Chen Q, Min C, Zhang W, et al. Unpacking the black box: how to promote citizen engagement through government social media during the COVID-19 crisis. Comput Human Behav 2020;110:106380. ArticlePubMedPMC
- 47. Wu L, Li J, Qi J, et al. How to promote public engagement and enhance sentiment through government social media during the COVID-19 crisis: a public value management perspective. J Organ End User Comput 2022;34:1−24.
- 48. Strekalova YA. Health risk information engagement and amplification on social media. Health Educ Behav 2017;44:332−9.ArticlePubMedPDF
- 49. Vijaykumar S, Jin Y, Nowak G. Social media and the virality of risk: the risk amplification through media spread (RAMS) model. J Homel Secur Emerg Manag 2015;12:653−77.Article
- 50. Tahamtan I, Potnis D, Mohammadi E, et al. The mutual influence of the World Health Organization (WHO) and Twitter users during COVID-19: network agenda-setting analysis. J Med Internet Res 2022;24:e34321.ArticlePubMedPMC
- 51. Liu W, Xu W, John S. Organizational disaster communication ecology: examining interagency coordination on social media during the onset of the COVID-19 pandemic. Am Behav Sci 2021;65:914−33.ArticlePDF
- 52. Vos SC, Sutton J, Yu Y, et al. Retweeting risk communication: the role of threat and efficacy. Risk Anal 2018;38:2580−98.ArticlePubMedPDF
- 53. Xie J, Liu L. Identifying features of source and message that influence the retweeting of health information on social media during the COVID-19 pandemic. BMC Public Health 2022;22:805. ArticlePubMedPMCPDF
- 54. El-Dakhs DA. #StayHome: a pragmatic analysis of COVID-19 health advice in Saudi and Australian tweets. Lang Dialogue 2021;11:223−45.Article
- 55. Azer J, Alexander M. COVID-19 vaccination: engagement behavior patterns and implications for public health service communication. J Serv Theory Pract 2022;32:323−51.Article
- 56. Guidry JP, Jin Y, Orr CA, et al. Ebola on Instagram and Twitter: how health organizations address the health crisis in their social media engagement. Public Relat Rev 2017;43:477−86.Article
- 57. Khokhar A, Spaulding A, Niazi Z, et al. A panel evaluation of the changes in the general public’s social-media-following of United States’ Public Health Departments during COVID-19 pandemic. J Prim Care Community Health 2021;12:2150132721995450. ArticlePubMedPMCPDF
- 58. Pathak TS, Athavale H, Pathak AS, et al. Sentiments evoked by WHO public health posts during the COVID-19 pandemic: a neural network-based machine learning analysis. Cureus 2021;13:e19141.ArticlePubMedPMC
- 59. Tang S, Wu X, Chen J, et al. Release and demand of public health information in social media during the outbreak of COVID-19 in China. Front Public Health 2022;9:829589. ArticlePubMedPMC
- 60. Laurent-Simpson A, Lo CC. Risk society online: Zika virus, social media and distrust in the Centers for Disease Control and Prevention. Sociol Health Illn 2019;41:1270−88.ArticlePubMedPDF
- 61. Sanders A, Ray-Majumder D, Erickson J, et al. Should we tweet this?: generative response modeling for predicting reception of public health messaging on Twitter. In: WebSci '22: Proceedings of the 14th ACM Web Science Conference 2022; 2022 Jun 26–29; Barcelona, Spain. Association for Computing Machinery; 2022. p. 307–18.Article
- 62. Slavik CE, Buttle C, Sturrock SL, et al. Examining tweet content and engagement of Canadian public health agencies and decision makers during COVID-19: mixed methods analysis. J Med Internet Res 2021;23:e24883.ArticlePubMedPMC
- 63. Loiti-Rodriguez S, Genaut-Arratibel A, Cantalapiedra-Gonzale MJ. Crisis communication in audiovisual format: information from Spain’s National Health System on YouTube in 2020. Prof Inf 2021;30:e300416.
- 64. Flores R, Asuncion XV. Toward an improved risk/crisis communication in this time of COVID-19 pandemic: a baseline study for Philippine local government units. J Sci Commun 2020;19:A09. Article
- 65. Sastry S, Lovari A. Communicating the ontological narrative of Ebola: an emerging disease in the time of “Epidemic 2.0”. Health Commun 2017;32:329−38.ArticlePubMed
- 66. Elgersma IH, Fretheim A, Indseth T, et al. The evaluation of a social media campaign to increase COVID-19 testing in migrant groups: cluster randomized trial. J Med Internet Res 2022;24:e34544.ArticlePubMedPMC
- 67. Liu BF, Kim S. How organizations framed the 2009 H1N1 pandemic via social and traditional media: implications for U.S. health communicators. Public Relat Rev 2011;37:233−44.Article
- 68. Radwan AF, Mousa SA. Government communication strategies during coronavirus pandemic: United Arab Emirates lessons. J Health Manag 2020;22:516−27.ArticlePDF
- 69. Basch CH, Fera J, Pierce I, et al. Promoting mask use on TikTok: descriptive, cross-sectional study. JMIR Public Health Surveill 2021;7:e26392.ArticlePubMedPMC
- 70. Locatelli E, Lovari A. Platformization of healthcare communication: insights from the early stage of the COVID-19 pandemic in Italy. Catalan J Commun Cult Stud 2021;13:249−66.Article
- 71. Sesagiri Raamkumar A, Tan SG, Wee HL. Measuring the outreach efforts of public health authorities and the public response on Facebook during the COVID-19 pandemic in early 2020: cross-country comparison. J Med Internet Res 2020;22:e19334.ArticlePubMedPMC
- 72. Obreja DM. Narrative communication regarding the COVID-19 vaccine: a thematic analysis of comments on Romanian official Facebook page “RO Vaccinare”. SN Soc Sci 2022;2:119. ArticlePubMedPMCPDF
- 73. Roy D, Das M, Deshbandhu A. Postcolonial pandemic publics: examining social media health promotion in India during the COVID-19 crisis. Health Promot Int 2022;37:daab076. ArticlePubMedPDF
- 74. Gesser-Edelsburg A, Hijazi R, Cohen R. It takes two to tango: how the COVID-19 vaccination campaign in Israel was framed by the health ministry vs. the television news. Front Public Health 2022;10:887579. ArticlePubMedPMC
- 75. Johnson TD. Utah health department launches public health YouTube series. Nations Health 2010;40:10.
- 76. Wong R, Harris JK, Staub M, et al. Local health departments tweeting about Ebola: characteristics and messaging. J Public Health Manag Pract 2017;23:e16−24.ArticlePubMed
- 77. Wang Y, Hao H, Platt LS. Examining risk and crisis communications of government agencies and stakeholders during early-stages of COVID-19 on Twitter. Comput Hum Behav 2021;114:106568. Article
- 78. Syn SY. Health information communication during a pandemic crisis: analysis of CDC Facebook page during COVID-19. Online Inf Rev 2021;45:672−86.Article
- 79. Ahmed MA, Sadri AM, Amini MH. Data-driven inferences of agency-level risk and response communication on COVID-19 through social media-based interactions. J Emerg Manag 2021;19:59−82.ArticlePubMedPDF
- 80. Glowacki EM, Lazard AJ, Wilcox GB, et al. Identifying the public’s concerns and the Centers for Disease Control and Prevention’s reactions during a health crisis: an analysis of a Zika live Twitter chat. Am J Infect Control 2016;44:1709−11.ArticlePubMed
- 81. Pang PC, Cai Q, Jiang W, et al. Engagement of government social media on Facebook during the COVID-19 pandemic in Macao. Int J Environ Res Public Health 2021;18:3508. ArticlePubMedPMC
- 82. Yang Y, Deng W, Zhang Y, et al. Promoting public engagement during the COVID-19 crisis: how effective is the Wuhan local government’s information release? Int J Environ Res Public Health 2021;18:118. Article
- 83. Zhang T, Yu L. The relationship between government information supply and public information demand in the early stage of COVID-19 in China: an empirical analysis. Healthcare (Basel) 2021;10:77. ArticlePubMedPMC
- 84. Chen Q, Min C, Zhang W, et al. Factors driving citizen engagement with government TikTok accounts during the COVID-19 pandemic: model development and analysis. J Med Internet Res 2021;23:e21463.ArticlePubMedPMC
- 85. Hodson J, Veletsianos G, Houlden S. Public responses to COVID-19 information from the public health office on Twitter and YouTube: implications for research practice. J Inf Technol Politics 2022;19:156−64.Article
- 86. Crook B, Glowacki EM, Suran M, et al. Content analysis of a live CDC Twitter chat during the 2014 Ebola outbreak. Commun Res Rep 2016;33:349−55.Article
- 87. Lazard AJ, Scheinfeld E, Bernhardt JM, et al. Detecting themes of public concern: a text mining analysis of the Centers for Disease Control and Prevention’s Ebola live Twitter chat. Am J Infect Control 2015;43:1109−11.ArticlePubMed
- 88. Chen S, Xu Q, Buchenberger J, et al. Dynamics of health agency response and public engagement in public health emergency: a case study of CDC tweeting patterns during the 2016 Zika epidemic. JMIR Public Health Surveill 2018;4:e10827.ArticlePubMedPMC
- 89. Shortt MT, Smeets I, Wiig S, et al. Shortcomings in public health authorities’ videos on COVID-19: limited reach and a creative gap. Front Commun 2021;6:764220. Article
- 90. Durowaye TD, Rice AR, Konkle AT, et al. Public health perinatal promotion during COVID-19 pandemic: a social media analysis. BMC Public Health 2022;22:895. ArticlePubMedPMCPDF
- 91. Pinto PA, Brasileiro FS, Lopes Antunes MJ, et al. Face masks on Instagram: an analysis of public health authorities’ guidance toward prevention. Procedia Comput Sci 2022;196:409−17.ArticlePubMedPMC
- 92. Das R, Banerjee I. Digital technology and health advocacy on COVID-19: a case study of Twitter handles of the World Health Organization and Ministry of Health of India. J Lib Int Aff 2021;7:97−117.Article
- 93. Xi H, Zhang C, Zhao Y, et al. Public emotional diffusion over COVID-19 related tweets posted by major public health agencies in the United States. Data Intell 2022;4:66−87.ArticlePDF
- 94. Lwin MO, Lu J, Sheldenkar A, et al. Temporal and textual analysis of social media on collective discourses during the Zika virus pandemic. BMC Public Health 2020;20:804. ArticlePubMedPMCPDF
- 95. Vijaykumar S, Meurzec RW, Jayasundar K, et al. What’s buzzing on your feed? Health authorities’ use of Facebook to combat Zika in Singapore. J Am Med Inform Assoc 2017;24:1155−9.ArticlePubMedPMCPDF
- 96. Bradford NJ, Amani B, Walker VP, et al. Barely tweeting and rarely about racism: assessing US state health department Twitter use during the COVID-19 vaccine rollout. Ethn Dis 2022;32:257−64.ArticlePubMedPMCPDF
- 97. Wong R, Harris JK. Geospatial distribution of local health department tweets and online searches about Ebola during the 2014 Ebola outbreak. Disaster Med Public Health Prep 2018;12:287−90.ArticlePubMed
- 98. Li Z, Wang M, Zhong J, et al. Improving the communication and credibility of government media in response to public health emergencies: analysis of tweets from the WeChat official accounts of 10 Chinese health commissioners. Front Public Health 2022;10:900776. ArticlePubMedPMC
- 99. Hannawa AF, Kreps GL, Paek HJ, et al. Emerging issues and future directions of the field of health communication. Health Commun 2014;29:955−61.ArticlePubMed
- 100. Hannawa AF, Garcia-Jimenez L, Candrian C, et al. Identifying the field of health communication. J Health Commun 2015;20:521−30.ArticlePubMed
 Cite
Cite