
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 11(2); 2020 > Article
-
Original Article
Cross-Country Comparison of Case Fatality Rates of COVID-19/SARS-COV-2 - Morteza Abdullatif Khafaiea, Fakher Rahimb
-
Osong Public Health and Research Perspectives 2020;11(2):74-80.
DOI: https://doi.org/10.24171/j.phrp.2020.11.2.03
Published online: April 30, 2020
aSocial Determinants of Health Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
bHealth Research Institute, Research Center of Thalassemia and Hemoglobinopathies, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
- *Corresponding author: Fakher Rahim, Health Research Institute, Research Center of Thalassemia and Hemoglobinopathies, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran, E-mail: bioinfo2003@gmail.com
• Received: March 13, 2020 • Revised: March 23, 2020 • Accepted: March 23, 2020
Copyright ©2020, Korea Centers for Disease Control and Prevention
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Abstract
-
Objectives
- Case fatality rates (CFR) and recovery rates are important readouts during epidemics and pandemics. In this article, an international analysis was performed on the ongoing coronavirus disease 2019 (COVID-19) pandemic.
-
Methods
- Data were retrieved from accurate databases according to the user’s guide of data sources for patient registries, CFR and recovery rates were calculated for each country. A comparison of CFR between countries with total cases ≥ 1,000 was observed for 12th and 23rd March.
-
Results
- Italy’s CFR was the highest of all countries studied for both time points (12th March, 6.22% versus 23rd March, 9.26%). The data showed that even though Italy was the only European country reported on 12rd March, Spain and France had the highest CFR of 6.16 and 4.21%, respectively, on 23rd March, which was strikingly higher than the overall CFR of 3.61%.
-
Conclusion
- Obtaining detailed and accurate medical history from COVID-19 patients, and analyzing CFR alongside the recovery rate, may enable the identification of the highest risk areas so that efficient medical care may be provided. This may lead to the development of point-of-care tools to help clinicians in stratifying patients based on possible requirements in the level of care, to increase the probabilities of survival from COVID-19 disease.
- A novel coronavirus has spread through China, originating from the city of Wuhan and has caused many deaths so far. It is a highly contagious virus that has spread rapidly and efficiently. Coronavirus disease 2019 (COVID-19) is caused by a virus (SARS-CoV-2) from the same family as the lethal coronaviruses that caused severe acute respiratory syndrome (SARS-CoV) and Middle East respiratory syndrome (MERS-CoV). COVID-19 is a relatively large virus (120 nm) and is enveloped, containing a positive-sense single-stranded RNA [1]. The virus is transmitted through direct contact with the infected person’s respiratory droplets (coughing and sneezing), as well as contact with infected surfaces. COVID-19 virus can survive for days on surfaces, but a simple disinfectant can eliminate this [2]. COVID-19 signs and symptoms include fever, cough, and shortness of breath. In more severe cases, infection can lead to pneumonia, serious respiratory problems and ultimately, fatalities. Thousands of people have been reported to have been infected with the virus so far [3]. Apart from China, other cases of the disease, also known as COVID-2, have been reported in several countries, including Thailand, South Korea, Japan, Taiwan, Australia, Iran, and the United States. According to the Worldometer, as of 10th March 2020, there are over 114,430 identified cases of COVID-19 worldwide in 115 countries and territories [1].
- Of these 115 countries, South Korea and Iran (outside of China) have the largest epidemic of COVID-19 and Italy, France and Spain are the countries with a major epidemic of COVID-19 in Europe [2]. COVID-19 spreads mainly from person-to-person during the latency period before the symptoms appear [4]. There is much more to learn about the spread and severity of COVID-19. COVID-19 can cause mild flu-like symptoms, including fever, cough, dyspnea, myalgia, and fatigue, while more serious forms can cause severe pneumonia, acute respiratory distress syndrome, septic shock, and organ failure, which can lead to death [5]. Without a vaccine for COVID-19, transmission of the virus can be reduced with early detection and patient quarantine [6]. There is epidemiological and clinical evidence to suggest a number of novel compounds, as well as medicines licensed for other conditions, that appear to have potential efficacy against COVID-19 [7,8]. However, in the absence of a safe and effective vaccine or medicine, reducing viral transmission is the only strategy available where general education, and implementing the appropriate prevention and control is key. Precautions can help suppress the risk of infection, such as washing the hands frequently with soap and water or an alcohol-based disinfectant gel, coughing into the elbow or a folded napkin/tissue, avoiding close contact with those who have symptoms, and self-isolating, but medical help must be sought if difficulty in breathing is experienced [5].
- COVID-19 can be diagnosed with diagnostic test kits [9] and imaging techniques such as chest X-ray and pulmonary CT scans that facilitate early diagnosis of pneumonia in patients with COVID-19 [10–12].
- The case fatality rate (CFR), is a measure of the ability of a pathogen or virus to infect or damage a host in infectious disease and is described as the proportion of deaths within a defined population of interest, i.e. the percentage of cases that result in death [13]. CFRs confers the extent of disease severity and CFR is necessary for setting priorities for public health in targeted interventions to reduce the severity of risk [14]. Initial studies reported an estimation of 3% for the global CFR of COVID-19 [15]. Estimating CFR from country-level data requires assessment of information about the delay between the report of the country-specific cases and death from COVID-19, as well as underestimating and under-reporting of death-related cases, which may not be known. Given the importance of CFR and recovery rate (RR), in this current study the CFR and RR of different countries during a COVID-19 ongoing pandemic was observed using up-to-date country-level data.
Introduction
- 1. Source of data and procedure
- The data were retrieved from accurate databases including Worldometer 2, WHO 3, the Center of Disease Control and Prevention [16], and the Morbidity and Mortality Weekly Report series (provided from Center of Disease Control and Prevention), according to the user’s guide of data sources for patient registries [17]. Due to the rapid increase in data, the analysis in this study was performed on the 12th and 23rd of March 2020.
- Raw data was mapped according to countries and CFR and RR were compared for countries with ≥ 1,000 cases. All countries with < 1,000 cases are presented in supplementary Table 1. A comparison of CFR with different known viral diseases was performed.
- 2. Measuring the CFR and RR
- The formulas below were used to measure CFR and RR.
Materials and Methods
- The total number of confirmed cases of COVID-19 was highest in China, followed by Italy and Iran on 12th March, but on 23rd March 2020, total COVID-19 confirmed cases was the highest in China, followed by Italy, USA, and Spain (Table 1). However, Italy’s CFR was the highest on both time points (12th March, 6.22% versus 23rd March, 9.26%). The data showed that Italy was the only European country reported on 12th March, but by the 23rd March 2020, Spain and France had the highest CFR of 6.16 and 4.21%, respectively, which was strikingly higher than the overall CFR of 3.61%. The highest RR was observed in China, with RR values of 76.12% and 89.85% in both analysis time points, respectively, compared with the overall RR of 55.83% and 29.3% on the 12th and 23rd March 2020, respectively.
- The highest CFR was observed in Italy, followed by China, Iran, and USA on 12th March, which changed to Italy, Spain, France, Iran, and China on 23rd March (Figure 1). Among European countries, Spain and France also faced an increasing rate of CFR. Although Morocco, Panama, and Iraq showed higher CFR values, there was only a small number of total cases, therefore the results of countries with highest outbreak and total cases of COVID-19 were preferentially reported.
- China showed encouraging recovery rates from COVID-19 at both time points (76.12% and 89.85% on 12th and 23rd March 2020, respectively; Figure 2). Although the COVID-19 outbreak has led to high rates of death in other Asian countries such as Iran, the recovery rate may be considered acceptable (34%).
- The comparison of CFR between different known infectious and viral diseases was shown in Figure 3. This revealed that the overall clinical concerns of COVID-19 may eventually be more like those of a severe seasonal flu (CFR of approximately 0.1%) or a pandemic flu, rather than SARS or MERS, which have had CFR of approximately 10% and 36%, correspondingly.
Results
- This study aimed to observe the CFR of different countries during an ongoing COVID-19 pandemic using recent country-level data, showing that alongside the outbreak of this virus, there is a frame-shift and transition from China (as the first country faced with the outbreak) to other countries in other continents.
- The outbreak was declared a public health emergency of international concern on 30th January 2020 [18]. Confronting emerging diseases requires universal cooperation in identifying, controlling, and preventing these diseases. The Center for Disease Control obtained a number of factors to establish a geographic risk assessment for the spread of COVID-19 (Supplementary Figure 1). This may be used for international guidelines for public health decisions and travel-related exposure. For instance, China and Iran were categorized as countries where there was widespread ongoing transmission, with restrictions on entry.
- The data from this study supports the fact that the CFR of the COVID-19 pandemic seems to be less than Bird flu, Ebola, SARS, and MERS, but public health concerns remain due to its highly infectious nature, since a large proportion of cases are asymptomatic or mild, which promotes the spread of the disease worldwide. In such situations, the media plays a crucial role in promoting health literacy and advocating limited spread of the disease [19]. Cross-country comparisons of CFR and RR as important indicators of disease characteristics are vital for national and international priority setting and recognizing health system performance. However, many factors can confound the current estimation for CFR and RR of COVID-19, namely, undetected cases or delayed case reporting, which can significantly affect the 2 indicators which are linked with a degree of preparedness and mitigation of both the general public and politicians.
- Since the number of cases in the world is increasing in a heterogeneous form, to obtain a better picture for cross-country compression of medical care performance, we require a limiting denominator of CFR and RR to be applied to cases under official medical care with final disease outcome (death/ recovered or discharged).
Discussion
- Death and severity of COVID-19 are associated with age and comorbidities across the world. Especially in countries with the highest outbreaks, such as China, Italy, and Iran, strategies must be employed to ensure that high-risk groups, such as old people and those with other underlying diseases such as diabetes and cancer, received adequate protection from COVID-19. Therefore, early access to medical care when infected is vital for improving chances of survival. Improving medical supplies to countries such as Iran, which is significantly influenced by US punitive policies, can reduce the deterioration of this politically sensitive situation [20].
- Furthermore, taking detailed and accurate medical history, and scoring CFR alongside RR, may highlight the highest risk areas, and more efficiently direct the intervention to decrease the spread of the virus globally. This may enable the development of point-of-care tools to help clinicians in stratifying patients, based on possible requirements in the level of care to improve probabilities of survival from COVID-19 disease.
Conclusion
Supplementary Information
-
Acknowledgements
- We acknowledge the contribution made by Dr. Asaad Sharhani, Department of Statistics and epidemiology at Ahvaz Jundishapur University of Medical Sciences, in data collection and data management.
Acknowledgments
- 1. Worlometers [Internet]. COVID-19 Coronavirus Pandemic 2020 Available from: https://www.worldometers.info/coronavirus/.
- 2. World Health Organization [Internet]. Coronavirus disease 2019 (COVID-19): Situation Report - 43 Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200303-sitrep-43-covid-19.pdf?sfvrsn=2c21c09c_2.
- 3. Xu XW, Wu XX, Jiang XG, et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. BMJ 2020;368:m606PMID: 10.1136/bmj.m606. PMID: 32075786.ArticlePubMedPMC
- 4. Lauer SA, Grantz KH, Bi Q, et al. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann Intern Med 2020;[Epub ahead of print]. Epub 2020 Mar 10. PMID: 10.7326/M20-0504. PMID: 32150748. PMID: 7081172.Article
- 5. Guan W, Ni Z, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med 2020;[Epub ahead of print]. Epub 2020 Mar 6. PMID: 10.1056/NEJMoa2002032. PMID: 32109013.Article
- 6. Jernigan DB. CDC COVID-19 Response Team. Update: Public Health Response to the Coronavirus Disease 2019 Outbreak - United States, February 24, 2020. MMWR 2020;69(8). 216−9. PMID: 32106216.ArticlePubMedPMC
- 7. Pang J, Wang MX, Ang IYH, et al. Potential Rapid Diagnostics, Vaccine and Therapeutics for 2019 Novel Coronavirus (2019-nCoV): A Systematic Review. J Clin Med 2020;9(3). E623PMID: 10.3390/jcm9030623. PMID: 32110875.Article
- 8. Zhang L, Liu Y. Potential interventions for novel coronavirus in China: A systematic review. J Med Virol 2020;92(5). 479−90. PMID: 10.1002/jmv.25707. PMID: 32052466.ArticlePubMedPMC
- 9. Yi Li Z, Luo YX, et al. Development and Clinical Application of A Rapid IgM-IgG Combined Antibody Test for SARS-CoV-2 Infection Diagnosis. J Med Virol 2020;[Epub ahead of print]. Epub 2020 Feb 27.
- 10. Yang XH, Sun RH, Chen DC. Diagnosis and treatment of COVID-19: Acute kidney injury cannot be ignored. Zhonghua Yi Xue Za Zhi 2020;100(0). E017[in Chinese]. PMID: 32145717.
- 11. Xia W, Shao J, Guo Y, et al. Clinical and CT features in pediatric patients with COVID-19 infection: Different points from adults. Pediatr Pulmonol 2020;[Epub ahead of print]. Epub 2020 Mar 05. PMID: 10.1002/ppul.24718. PMID: 32134205.Article
- 12. Zhao W, Zhong Z, Xie X, Yu Q, Liu J. Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. AJR Am J Roentgenol 2020;[Epub ahead of print]. Epub 2020 Mar 3. PMID: 10.2214/AJR.20.22976. PMID: 32125873.Article
- 13. Kanchan T, Kumar N, Unnikrishnan B. Mortality: Statistics. Encyclopedia of Forensic and Legal Medicine. 2nd ed.Elsevier Inc; 2015. pp 572−7.Article
- 14. Reich NG, Lessler J, Cummings DAT, Brookmeyer R. Estimating absolute and relative case fatality ratios from infectious disease surveillance data. Biometrics 2012;68(2). 598−606. PMID: 10.1111/j.1541-0420.2011.01709.x. PMID: 22276951. PMID: 4540071.ArticlePubMedPMC
- 15. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet 2020;395(10223). 470−3. PMID: 10.1016/S0140-6736(20)30185-9. PMID: 31986257.ArticlePubMedPMC
- 16. Centers of Disease Control and Prevention [Internet]. Cases in U. S. 2020 Mar 23 Available from: https://www.cdc.gov/coronavirus/2019-ncov/cases-in-us.html.
- 17. Gliklich RE, Dreyer NA, Leavy MB. [Internet] Registries for Evaluating Patient Outcomes: A User’s Guide 3rd ed. Rockville (MD): Agency for Healthcare Research and Quality (US); 2014 Available from: https://www.ncbi.nlm.nih.gov/books/NBK208611/.
- 18. Eurosurveillance editorial team. Note from the editors: World Health Organization declares novel coronavirus (2019-nCoV) sixth public health emergency of international concern. Euro Surveill 2020;25(5). 200131ePMID: 7014669.ArticlePubMedPMC
- 19. Mojadam M, Matlabi M, Haji A, et al. Khuzestan dust phenomenon: A content analysis of most widely circulated newspapers. Environ Sci Pollut Res 2018;25:15918−24. PMID: 10.1007/s11356-018-1833-5.ArticlePDF
- 20. Takian A, Raoofi A, Kazempour-Ardebili S. COVID-19 battle during the toughest sanctions against Iran. Lancet 2020;[Epub ahead of print]. Epub 2020 Mar 18. PMID: 10.1016/S0140-6736(20)30668-1. PMID: 32199073.Article
References
Figure 1The cross-country comparison of case fatality rate (CFR) between different countries (n = 116). The circles showed the countries with highest outbreak and positive cases of COVID-19. Countries with CFR value zero has not been illustrated here.
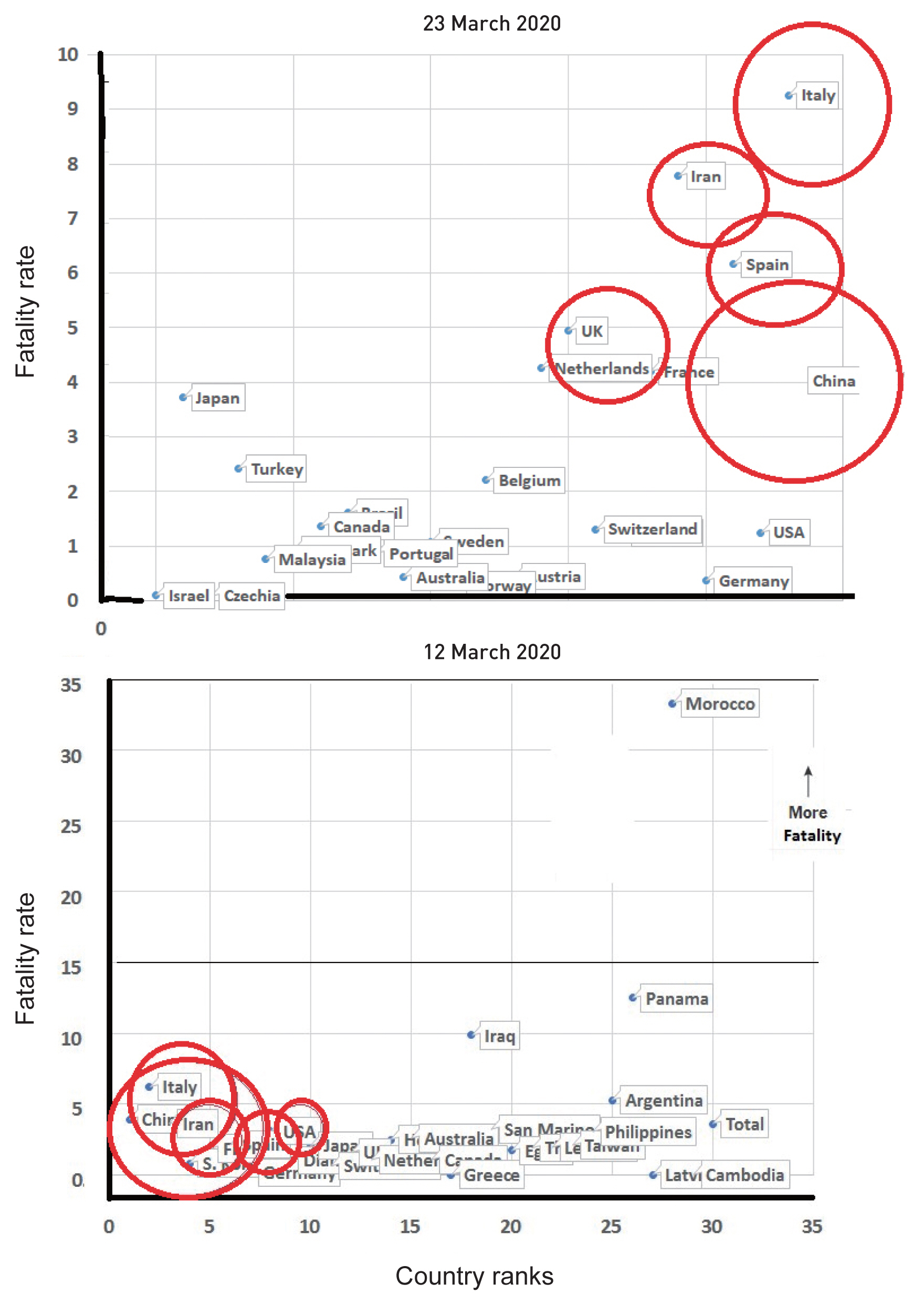
Figure 2The cross-country comparison of recovery rate (RR) between different countries (n = 116). The circles showed the countries with highest outbreak and positive cases of COVID-19. Countries with RR value zero has not been illustrated here.

Figure 3The cross-country comparison of case fatality rate (CFR) between different known infectious and viral diseases (n = 116). The circles showed the estimated value and the reported range of CFR of COVID-19.
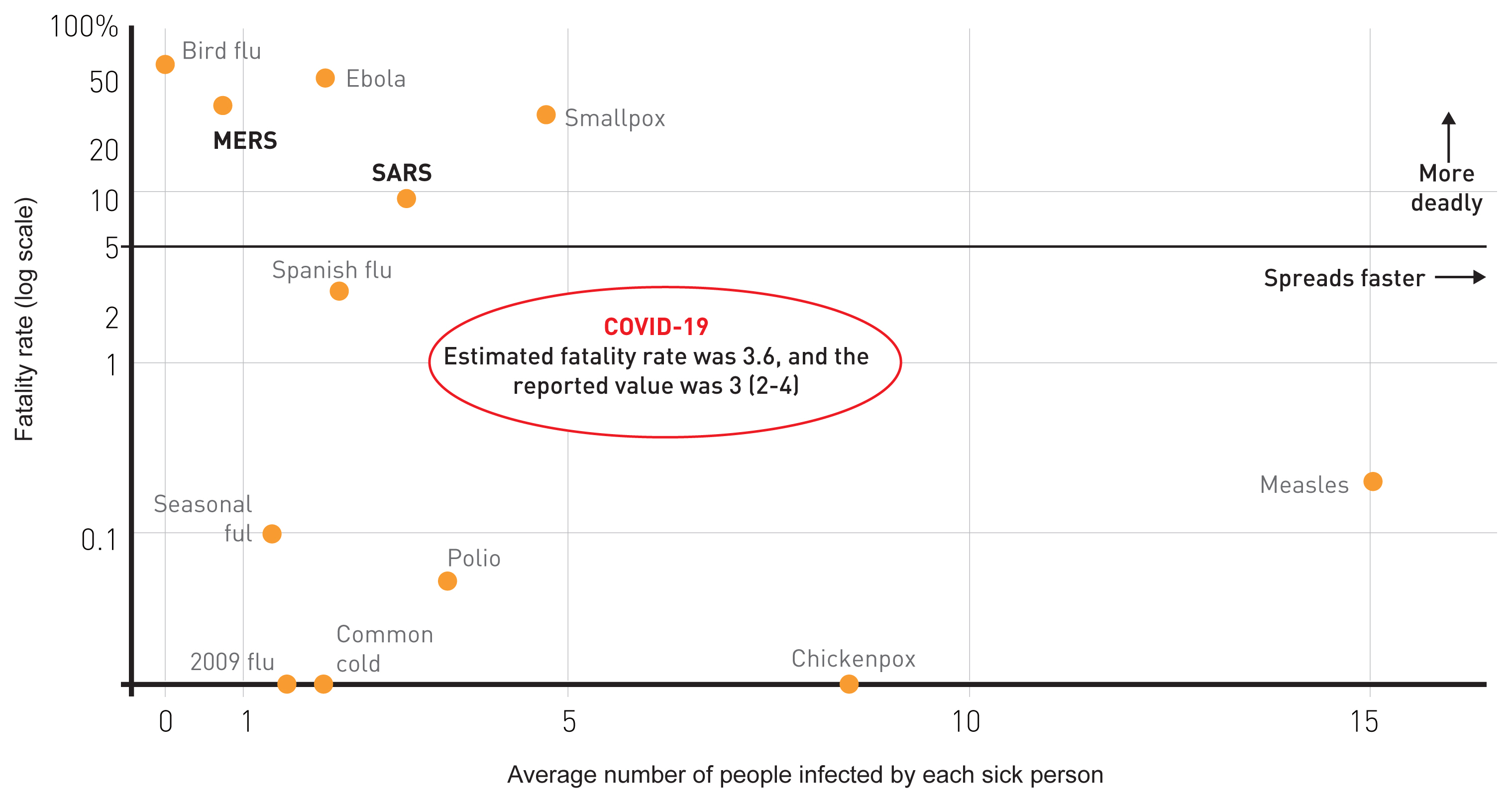
Table 1The comparison of case fatality rate (CFR) and recovery rate (RR) between different countries (n = 116). Only countries with total cases over 1,000 cases depicted (population in million and GDP in trillion USD; n = 116).
Figure & Data
References
Citations
Citations to this article as recorded by 
- Social and Spatial Inequalities during COVID-19: Evidence from France and the Need for a New Sustainable Urban and Regional Development Paradigm
Roula Maya
Sustainability.2024; 16(8): 3501. CrossRef - Impact of pandemic on development and demography in different continents and nations
Pawan Kumar Singh, Alok Kumar Pandey, Ravi Kiran, Rajiv Kumar Bhatt, Anushka Chouhan
International Journal of Finance & Economics.2023; 28(3): 3119. CrossRef - Inhibition of the predicted allosteric site of the SARS-CoV-2 main protease through flavonoids
Bibi Kubra, Syed Lal Badshah, Shah Faisal, Mohamed Sharaf, Abdul-Hamid Emwas, Mariusz Jaremko, Mohnad Abdalla
Journal of Biomolecular Structure and Dynamics.2023; 41(18): 9103. CrossRef - The Probable Protective Effect of Photobiomodulation on the Immunologic Factor’s mRNA Expression Level in the Lung: An Extended COVID-19 Preclinical and Clinical Meta-analysis
Babak Arjmand, Fakher Rahim
Clinical Pathology.2023; 16: 2632010X2211276. CrossRef - Applying Machine Learning to Healthcare Operations Management: CNN-Based Model for Malaria Diagnosis
Young Sik Cho, Paul C. Hong
Healthcare.2023; 11(12): 1779. CrossRef - Resilience strengthening of tuberculosis diagnostic services under national tuberculosis program to withstand pandemic situations
Sarika Jain, Monil Singhai, Vineet Chadha, N. Somashekar
Indian Journal of Medical Sciences.2023; 75: 94. CrossRef - An Assessment on Health And COVID-19 Indicators of OECD Countries
Mustafa FİLİZ
Turkish Journal of Family Medicine and Primary Car.2023; 17(3): 338. CrossRef - A comparison of symptom management and utilization of specialist palliative care in the early COVID-19 pandemic: A multi-site retrospective chart review
Madelaine Baetz-Dougan, Jennifer Guan, Blair Henry, Kalli Stilos, Desmond Leung, Niren Shetty, Shruti Gupta, Anita Chakraborty
Progress in Palliative Care.2023; 31(6): 333. CrossRef - Psychological impact of COVID-19 and determinants among Spanish university students
Jesús Cebrino, Silvia Portero de la Cruz
Frontiers in Public Health.2023;[Epub] CrossRef - Uncovering the impact of COVID-19 on the place of death of cancer patients in South America
Doris Durán, Renzo Calderon Anyosa, Belinda Nicolau, Jay S. Kaufman
Cadernos de Saúde Pública.2023;[Epub] CrossRef - COVID-19 and cardiovascular diseases: Past, present, and future
Barun Kumar, Abhimanyu Nigam, Shishir Soni, Vikas Kumar, Anupam Singh, Omna Chawla
Journal of Cardio-diabetes and metabolic disorders.2022; 2(2): 41. CrossRef - Examining the geographic distribution of six chronic disease risk factors for severe COVID-19: Veteran–nonveteran differences
Michelle McDaniel, Justin T McDaniel
Chronic Illness.2022; 18(3): 666. CrossRef - Suicidal Ideation during the COVID-19 Pandemic among A Large-Scale Iranian Sample: The Roles of Generalized Trust, Insomnia, and Fear of COVID-19
Chung-Ying Lin, Zainab Alimoradi, Narges Ehsani, Maurice M. Ohayon, Shun-Hua Chen, Mark D. Griffiths, Amir H. Pakpour
Healthcare.2022; 10(1): 93. CrossRef - COVID-19 and Sanctions Affecting Afghans in Iran
Athar Shafaei, Karen Block
Journal of Immigrant & Refugee Studies.2022; : 1. CrossRef - Heterogeneity of the COVID-19 Pandemic in the United States of America: A Geo-Epidemiological Perspective
Alexandre Vallée
Frontiers in Public Health.2022;[Epub] CrossRef - COVID-19 mortality, excess mortality, deaths per million and infection fatality ratio, Belgium, 9 March 2020 to 28 June 2020
Geert Molenberghs, Christel Faes, Johan Verbeeck, Patrick Deboosere, Steven Abrams, Lander Willem, Jan Aerts, Heidi Theeten, Brecht Devleesschauwer, Natalia Bustos Sierra, Françoise Renard, Sereina Herzog, Patrick Lusyne, Johan Van der Heyden, Herman Van
Eurosurveillance.2022;[Epub] CrossRef - Assessing the impact of temperature and humidity exposures during early infection stages on case-fatality of COVID-19: A modelling study in Europe
Jingbo Liang, Hsiang-Yu Yuan
Environmental Research.2022; 211: 112931. CrossRef - The Analysis of Turkey’s Fight Against the COVID-19 Outbreak Using K-Means Clustering and Curve Fitting
Fatih Ahmet Şenel
Vietnam Journal of Computer Science.2022; 09(01): 19. CrossRef - China's COVID-19 Control Strategy and Its Impact on the Global Pandemic
Difeng Ding, Ruilian Zhang
Frontiers in Public Health.2022;[Epub] CrossRef - Generalized Susceptible–Exposed–Infectious–Recovered model and its contributing factors for analysing the death and recovery rates of the COVID-19 pandemic
Felin Wilta, Allyson Li Chen Chong, Ganeshsree Selvachandran, Ketan Kotecha, Weiping Ding
Applied Soft Computing.2022; 123: 108973. CrossRef - Is there an association between COVID-19 mortality and Human development index? The case study of Nigeria and some selected countries
Sanyaolu Alani Ameye, Temitope Olumuyiwa Ojo, Tajudin Adesegun Adetunji, Michael Olusesan Awoleye
BMC Research Notes.2022;[Epub] CrossRef - Modeling for the Stringency of Lock-Down Policies: Effects of Macroeconomic and Healthcare Variables in Response to the COVID-19 Pandemic
Giunio Santini, Mario Fordellone, Silvia Boffo, Simona Signoriello, Danila De Vito, Paolo Chiodini
Frontiers in Public Health.2022;[Epub] CrossRef - The association between different predictive biomarkers and mortality of COVID-19
Narges Ansari, Mina Jahangiri, Kimia Shirbandi, Mina Ebrahimi, Fakher Rahim
Bulletin of the National Research Centre.2022;[Epub] CrossRef - Association of COVID-19 Case-Fatality Rate With State Health Disparity in the United States
Yu-Che Lee, Ko-Yun Chang, Mehdi Mirsaeidi
Frontiers in Medicine.2022;[Epub] CrossRef - Leveraging the therapeutic, biological, and self-assembling potential of peptides for the treatment of viral infections
Maya K. Monroe, Han Wang, Caleb F. Anderson, Hongpeng Jia, Charles Flexner, Honggang Cui
Journal of Controlled Release.2022; 348: 1028. CrossRef - COVID-19 Mortality and Related Comorbidities in Hospitalized Patients in Bulgaria
Rositsa Dimova, Rumyana Stoyanova, Vesela Blagoeva, Momchil Mavrov, Mladen Doykov
Healthcare.2022; 10(8): 1535. CrossRef - COVID-19 trends, public restrictions policies and vaccination status by economic ranking of countries: a longitudinal study from 110 countries
Myung-Bae Park, Chhabi Lal Ranabhat
Archives of Public Health.2022;[Epub] CrossRef - Impact of Immunotherapies on SARS-CoV-2-Infections and Other Respiratory Tract Infections during the COVID-19 Winter Season in IBD Patients
Constanze Heike Waggershauser, Cornelia Tillack-Schreiber, Paul Weyh, Eckard Alt, Thorsten Siegmund, Christine Berchthold-Benchieb, Daniel Szokodi, Fabian Schnitzler, Thomas Ochsenkühn, Alessandro Granito
Canadian Journal of Gastroenterology and Hepatolog.2022; 2022: 1. CrossRef - Epidemiological features of COVID-19 in Iran
Negah Tavakolifard, Mina Moeini, Asefeh Haddadpoor, Zahra Amini, Kamal Heidari, Mostafa Rezaie
Journal of Research in Medical Sciences.2022; 27(1): 75. CrossRef - MULTIMOORA ile En İyi Makine Öğrenimi Algoritmasının Seçimi ve Covid-19 Pandemisi için Dünya Çapında Ülke Kümelerinin Belirlenmesi
Sevgi ABDALLA, Özlem ALPU
European Journal of Science and Technology.2022;[Epub] CrossRef - Global variations in the burden of SARS-CoV-2 infection and its outcomes in pregnant women by geographical region and country’s income status: a meta-analysis
Jameela Sheikh, Heidi Lawson, John Allotey, Magnus Yap, Rishab Balaji, Tania Kew, Elena Stallings, Dyuti Coomar, Andrea Gaetano-Gil, Javier Zamora, Shakila Thangaratinam
BMJ Global Health.2022; 7(11): e010060. CrossRef - Predictive Model for National Minimal CFR during Spontaneous Initial Outbreak of Emerging Infectious Disease: Lessons from COVID-19 Pandemic in 214 Nations and Regions
Xiaoli Wang, Lin Fan, Ziqiang Dai, Li Li, Xianliang Wang
International Journal of Environmental Research an.2022; 20(1): 594. CrossRef - A Statistical Analysis and Comparison of the spread of Swine Flu and COVID-19 in India
Hari Murthy, Boppuru Rudra Prathap, Mani Joseph P, Vinay Jha Pillai, Sarath Chandra K, Kukatlapalli Pradeep Kumar
Malaysian Journal of Medicine and Health Sciences.2022; 18(6): 92. CrossRef - More than just a common cold: Endemic coronaviruses OC43, HKU1, NL63, and 229E associated with severe acute respiratory infection and fatality cases among healthy adults
Ana B. Gorini da Veiga, Letícia G. Martins, Irina Riediger, Alix Mazetto, Maria do Carmo Debur, Tatiana S. Gregianini
Journal of Medical Virology.2021; 93(2): 1002. CrossRef - Emergence of European and North American mutant variants of SARS‐CoV‐2 in South‐East Asia
Ovinu Kibria Islam, Hassan M. Al‐Emran, Md. Shazid Hasan, Azraf Anwar, Md. Iqbal Kabir Jahid, Md. Anwar Hossain
Transboundary and Emerging Diseases.2021; 68(2): 824. CrossRef - Automated analysis of fatality rates for COVID 19 across different countries
Shaima Ibraheem Jabbar
Alexandria Engineering Journal.2021; 60(1): 521. CrossRef - Tocilizumab use in patients with moderate to severe COVID‐19: A retrospective cohort study
Sridhar Chilimuri, Haozhe Sun, Ahmed Alemam, Kyoung‐Sil Kang, Peter Lao, Nikhitha Mantri, Lawrence Schiller, Myroslava Sharabun, Elona Shehi, Jairo Tejada, Alla Yugay, Suresh Kumar Nayudu
Journal of Clinical Pharmacy and Therapeutics.2021; 46(2): 440. CrossRef - COVID-19 recovery rate and its association with development
Akancha Singh, Aparajita Chattopadhyay
Indian Journal of Medical Sciences.2021; 73: 8. CrossRef - Compositional diversity and evolutionary pattern of coronavirus accessory proteins
Jingzhe Shang, Na Han, Ziyi Chen, Yousong Peng, Liang Li, Hangyu Zhou, Chengyang Ji, Jing Meng, Taijiao Jiang, Aiping Wu
Briefings in Bioinformatics.2021; 22(2): 1267. CrossRef - Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection
José L Hernández, Daniel Nan, Marta Fernandez-Ayala, Mayte García-Unzueta, Miguel A Hernández-Hernández, Marcos López-Hoyos, Pedro Muñoz-Cacho, José M Olmos, Manuel Gutiérrez-Cuadra, Juan J Ruiz-Cubillán, Javier Crespo, Víctor M Martínez-Taboada
The Journal of Clinical Endocrinology & Metabolism.2021; 106(3): e1343. CrossRef - Use of powered air-purifying respirator(PAPR) as part of protective equipment against SARS-CoV-2-a narrative review and critical appraisal of evidence
Ana Licina, Andrew Silvers
American Journal of Infection Control.2021; 49(4): 492. CrossRef - Postmortem Stability of SARS-CoV-2 in Nasopharyngeal Mucosa
Fabian Heinrich, Kira Meißner, Felicia Langenwalder, Klaus Püschel, Dominik Nörz, Armin Hoffmann, Marc Lütgehetmann, Martin Aepfelbacher, Eric Bibiza-Freiwald, Susanne Pfefferle, Axel Heinemann
Emerging Infectious Diseases.2021; 27(1): 329. CrossRef - COVID-19 caseness: An epidemiologic perspective
Abdel-Hady El-Gilany
Journal of Infection and Public Health.2021; 14(1): 61. CrossRef - Why are ACE2 binding coronavirus strains SARS‐CoV/SARS‐CoV‐2 wild and NL63 mild?
Puneet Rawat, Sherlyn Jemimah, P. K. Ponnuswamy, M. Michael Gromiha
Proteins: Structure, Function, and Bioinformatics.2021; 89(4): 389. CrossRef - COVID-19 case fatality rates across Southeast Asian countries (SEA): a preliminary estimate using a simple linear regression model
George R Puno, Rena Christina C Puno, Ida V Maghuyop
Journal of Health Research.2021; 35(3): 286. CrossRef - Low-Dose Radiation Therapy for COVID-19: Promises and Pitfalls
Bhanu P Venkatesulu, Scott Lester, Cheng-En Hsieh, Vivek Verma, Elad Sharon, Mansoor Ahmed, Sunil Krishnan
JNCI Cancer Spectrum.2021;[Epub] CrossRef - Professional football clubs and empirical evidence from the COVID-19 crisis: Time for sport entrepreneurship?
Jonas Hammerschmidt, Susanne Durst, Sascha Kraus, Kaisu Puumalainen
Technological Forecasting and Social Change.2021; 165: 120572. CrossRef - In silico validation of potent phytochemical orientin as inhibitor of SARS-CoV-2 spike and host cell receptor GRP78 binding
Arijit Bhowmik, Souradeep Biswas, Subhadip Hajra, Prosenjit Saha
Heliyon.2021; 7(1): e05923. CrossRef - SARS-CoV-2 Mediated Endothelial Dysfunction: The Potential Role of Chronic Oxidative Stress
Ryan Chang, Abrar Mamun, Abishai Dominic, Nhat-Tu Le
Frontiers in Physiology.2021;[Epub] CrossRef - The Profile of the Obstetric Patients with SARS-CoV-2 Infection According to Country of Origin of the Publication: A Systematic Review of the Literature
Yolanda Cuñarro-López, Pilar Pintado-Recarte, Ignacio Cueto-Hernández, Concepción Hernández-Martín, María Pilar Payá-Martínez, María del Mar Muñóz-Chápuli, Óscar Cano-Valderrama, Coral Bravo, Julia Bujan, Melchor Álvarez-Mon, Miguel A. Ortega, Juan Antoni
Journal of Clinical Medicine.2021; 10(2): 360. CrossRef - Depressive Symptoms, Fatigue and Social Relationships Influenced Physical Activity in Frail Older Community-Dwellers during the Spanish Lockdown due to the COVID-19 Pandemic
Laura M. Pérez, Carmina Castellano-Tejedor, Matteo Cesari, Luis Soto-Bagaria, Joan Ars, Fabricio Zambom-Ferraresi, Sonia Baró, Francisco Díaz-Gallego, Jordi Vilaró, María B. Enfedaque, Paula Espí-Valbé, Marco Inzitari
International Journal of Environmental Research an.2021; 18(2): 808. CrossRef - A knowledge gap unmasked: viral transmission in surgical smoke: a systematic review
Connal Robertson-More, Ted Wu
Surgical Endoscopy.2021; 35(6): 2428. CrossRef - Geospatial dynamics of COVID‐19 clusters and hotspots in Bangladesh
Ariful Islam, Md. Abu Sayeed, Md. Kaisar Rahman, Jinnat Ferdous, Shariful Islam, Mohammad Mahmudul Hassan
Transboundary and Emerging Diseases.2021; 68(6): 3643. CrossRef - Factors associated with the spatial heterogeneity of the first wave of COVID-19 in France: a nationwide geo-epidemiological study
Jean Gaudart, Jordi Landier, Laetitia Huiart, Eva Legendre, Laurent Lehot, Marc Karim Bendiane, Laurent Chiche, Aliette Petitjean, Emilie Mosnier, Fati Kirakoya-Samadoulougou, Jacques Demongeot, Renaud Piarroux, Stanislas Rebaudet
The Lancet Public Health.2021; 6(4): e222. CrossRef - A preliminary exploration of attitudes about COVID-19 among a group of older people in Iwate Prefecture, Japan
Lauren He, John W. Traphagan
Journal of Cross-Cultural Gerontology.2021; 36(1): 1. CrossRef - Unexpected high frequency of early mortality in COVID‐19: a single‐centre experience during the first wave of the pandemic
Diana Consuegra, Yoshua Seidner‐Isaacs, Didier Larios‐Sanjuan, Julieth Ibarra, Pedro Benavides‐Rodríguez, Samir Viloria, Emiro Buendía, Diego Viasus
Internal Medicine Journal.2021; 51(1): 102. CrossRef - “The Tragedy of the Commons”: How Individualism and Collectivism Affected the Spread of the COVID-19 Pandemic
Yossi Maaravi, Aharon Levy, Tamar Gur, Dan Confino, Sandra Segal
Frontiers in Public Health.2021;[Epub] CrossRef - Sensitivity analysis of the infection transmissibility in the UK during the COVID-19 pandemic
Pardis Biglarbeigi, Kok Yew Ng, Dewar Finlay, Raymond Bond, Min Jing, James McLaughlin
PeerJ.2021; 9: e10992. CrossRef - Contributions of human ACE2 and TMPRSS2 in determining host–pathogen interaction of COVID-19
SABYASACHI SENAPATI, PRATIBHA BANERJEE, SANDILYA BHAGAVATULA, PREM PRAKASH KUSHWAHA, SHASHANK KUMAR
Journal of Genetics.2021;[Epub] CrossRef - Outcomes of Patients With Coronavirus Disease 2019 Receiving Organ Support Therapies: The International Viral Infection and Respiratory Illness Universal Study Registry
Juan Pablo Domecq, Amos Lal, Christopher R. Sheldrick, Vishakha K. Kumar, Karen Boman, Scott Bolesta, Vikas Bansal, Michael O. Harhay, Michael A. Garcia, Margit Kaufman, Valerie Danesh, Sreekanth Cheruku, Valerie M. Banner-Goodspeed, Harry L. Anderson, Pa
Critical Care Medicine.2021; 49(3): 437. CrossRef - The link between vitamin D deficiency and COVID-19
DevasahayamJesudas Christopher, BarneyTJ Isaac, Balamugesh Thangakunam
Lung India.2021; 38(7): 4. CrossRef - Finding the real COVID-19 case-fatality rates for SAARC countries
Md Rafil Tazir Shah, Tanvir Ahammed, Aniqua Anjum, Anisa Ahmed Chowdhury, Afroza Jannat Suchana
Biosafety and Health.2021; 3(3): 164. CrossRef - Estimation of novel coronavirus (COVID‐19) reproduction number and case fatality rate: A systematic review and meta‐analysis
Tanvir Ahammed, Aniqua Anjum, Mohammad Meshbahur Rahman, Najmul Haider, Richard Kock, Md Jamal Uddin
Health Science Reports.2021;[Epub] CrossRef - COVID-SCORE Spain: public perceptions of key government COVID-19 control measures
Trenton M White, Lucinda Cash-Gibson, Jose M Martin-Moreno, Rafael Matesanz, Javier Crespo, Jose L Alfonso-Sanchez, Sonia Villapol, Ayman El-Mohandes, Jeffrey V Lazarus
European Journal of Public Health.2021; 31(5): 1095. CrossRef - How COVID-19 case fatality rates have shaped perceptions and travel intention?
Raymond Rastegar, Siamak Seyfi, S. Mostafa Rasoolimanesh
Journal of Hospitality and Tourism Management.2021; 47: 353. CrossRef - Lockdown strategy worth lives: The SEIRD modelling in COVID-19 outbreak in Indonesia
I Nurlaila, A A Hidayat, B Pardamean
IOP Conference Series: Earth and Environmental Sci.2021; 729(1): 012002. CrossRef - Genomic Surveillance of Circulating SARS-CoV-2 in South East Italy: A One-Year Retrospective Genetic Study
Loredana Capozzi, Angelica Bianco, Laura Del Sambro, Domenico Simone, Antonio Lippolis, Maria Notarnicola, Graziano Pesole, Lorenzo Pace, Domenico Galante, Antonio Parisi
Viruses.2021; 13(5): 731. CrossRef - Dynamics of COVID-19 spreading model with social media public health awareness diffusion over multiplex networks: Analysis and control
Padmavathi Ramamoorthi, Senthilkumar Muthukrishnan
International Journal of Modern Physics C.2021; 32(05): 2150060. CrossRef - The relationship between measures of individualism and collectivism and the impact of COVID-19 across nations
Ravi Philip Rajkumar
Public Health in Practice.2021; 2: 100143. CrossRef - Facilities for Centralized Isolation and Quarantine for the Observation and Treatment of Patients with COVID-19
Xianliang Wang, Jiao Wang, Jin Shen, John S. Ji, Lijun Pan, Hang Liu, Kangfeng Zhao, Li Li, Bo Ying, Lin Fan, Liubo Zhang, Lin Wang, Xiaoming Shi
Engineering.2021; 7(7): 908. CrossRef - SARS-CoV-2 simulations go exascale to predict dramatic spike opening and cryptic pockets across the proteome
Maxwell I. Zimmerman, Justin R. Porter, Michael D. Ward, Sukrit Singh, Neha Vithani, Artur Meller, Upasana L. Mallimadugula, Catherine E. Kuhn, Jonathan H. Borowsky, Rafal P. Wiewiora, Matthew F. D. Hurley, Aoife M. Harbison, Carl A. Fogarty, Joseph E. Co
Nature Chemistry.2021; 13(7): 651. CrossRef - Recent advances in detection technologies for COVID-19
Tingting Han, Hailin Cong, Youqing Shen, Bing Yu
Talanta.2021; 233: 122609. CrossRef - Nanomedicine: A Diagnostic and Therapeutic Approach to COVID-19
Arjun Sharma, Konstantinos Kontodimas, Markus Bosmann
Frontiers in Medicine.2021;[Epub] CrossRef - A cross-sectional pilot study on COVID-19 disease pattern, recovery status and effect of co-morbidities in Bangladesh
Monirul Islam Md., Shahriar Saimon, Jannat Koly Fahima, Kabir Shaila, Asad Choudhury Abu, Ahmed Chowdhury Jakir, Rafat Tahsin Md., Shah Amran Md.
African Journal of Pharmacy and Pharmacology.2021; 15(5): 84. CrossRef - Micronutrient zinc roles in adjunctive therapy for COVID-19 by enhancing patients immunoregulation and tolerance to the pathogen
Ba Xuan Hoang, Bo Han
Reviews in Medical Microbiology.2021; 32(3): 149. CrossRef - Dissecting the common and compartment-specific features of COVID-19 severity in the lung and periphery with single-cell resolution
Kalon J. Overholt, Jonathan R. Krog, Ivan Zanoni, Bryan D. Bryson
iScience.2021; 24(7): 102738. CrossRef - Psychological reaction to Covid-19 of Italian patients with IBD
Mariarosaria Savarese, Greta Castellini, Salvatore Leone, Enrica Previtali, Alessandro Armuzzi, Guendalina Graffigna
BMC Psychology.2021;[Epub] CrossRef - Emerging mutation in SARS-CoV-2 spike: Widening distribution over time in different geographic areas
Ysrafil Ysrafil, Rosdiana Mus, Noviyanty Indjar Gama, Dwi Rahmaisyah, Riskah Nur'amalia
Biomedical Journal.2021; 44(5): 570. CrossRef - The impact of COVID-19 on rural population: A retrospective study
İbrahim Halil İNANÇ, Nurbanu BURSA, Ahmet GÜLTEPE, Cengiz ŞABANOĞLU
Journal of Health Sciences and Medicine.2021; 4(5): 722. CrossRef - Perceptions of primary healthcare physicians in Jordan of their role in the COVID‐19 pandemic: A cross‐sectional study
Rami Saadeh, Mahmoud A. Alfaqih, Amjad Al‐Shdaifat, Mohammad Alyahya, Nasr Alrabadi, Yousef Khader, Othman Beni Yonis, Mohammed Z. Allouh
International Journal of Clinical Practice.2021;[Epub] CrossRef - Counting the Dead: COVID-19 and Mortality in Quebec and British Columbia During the First Wave
Yann Décarie, Pierre-Carl Michaud
Canadian Studies in Population.2021; 48(2-3): 139. CrossRef - Human Amniotic Fluid for the Treatment of Hospitalized, Symptomatic, and Laboratory-verified SARS-CoV-2 Patients
Mojgan Barati, Fakher Rahim
The Open Biology Journal.2021; 9(1): 36. CrossRef - The Drug Repurposing for COVID-19 Clinical Trials Provide Very Effective Therapeutic Combinations: Lessons Learned From Major Clinical Studies
Chiranjib Chakraborty, Ashish Ranjan Sharma, Manojit Bhattacharya, Govindasamy Agoramoorthy, Sang-Soo Lee
Frontiers in Pharmacology.2021;[Epub] CrossRef - Epidemic size, trend and spatiotemporal mapping of SARS-CoV-2 using geographical information system in Alborz Province, Iran
Kourosh Kabir, Ali Taherinia, Davoud Ashourloo, Ahmad Khosravi, Hossien Karim, Hamid Salehi Shahrabi, Mojtaba Hedayat Yaghoobi, Alireza Soleimani, Zaynab Siami, Mohammad Noorisepehr, Ramin Tajbakhsh, Mohammad Reza Maghsoudi, Mehran Lak, Parham Mardi, Behn
BMC Infectious Diseases.2021;[Epub] CrossRef - Micro-environmental conditions and high population density affects the transmission of severe acute respiratory syndrome corona virus-2 in metropolitan cities of India
Sanjay Dwivedi, Seema Mishra, Ruchi Agnihotri, Vishnu Kumar, Pragya Sharma, Geetgovind Sinam, Vivek Pandey
Environmental Disease.2021; 6(4): 116. CrossRef - Underlying Chronic Disease and COVID-19 Infection: A State-of-the-Art Review
Habib Haybar, Khalil Kazemnia, Fakher Rahim
Jundishapur Journal of Chronic Disease Care.2020;[Epub] CrossRef - Twitter Sentiment Analysis during COVID19 Outbreak
Akash Dutt Dubey
SSRN Electronic Journal .2020;[Epub] CrossRef - Challenges in maintaining treatment services for people who use drugs during the COVID-19 pandemic
Adrian Dunlop, Buddhima Lokuge, Debbie Masters, Marcia Sequeira, Peter Saul, Grace Dunlop, John Ryan, Michelle Hall, Nadine Ezard, Paul Haber, Nicholas Lintzeris, Lisa Maher
Harm Reduction Journal.2020;[Epub] CrossRef - Estimating Case Fatality Rate of Symptomatic Patients with COVID-19: Is This the Right Thing to Do?
Morteza Abdullatif Khafaie, Fakher Rahim
SSRN Electronic Journal .2020;[Epub] CrossRef - Three novel prevention, diagnostic, and treatment options for COVID-19 urgently necessitating controlled randomized trials
Richard I. Horowitz, Phyllis R. Freeman
Medical Hypotheses.2020; 143: 109851. CrossRef - Considerations for an Individual-Level Population Notification System for Pandemic Response: A Review and Prototype
Mohammad Nazmus Sakib, Zahid A Butt, Plinio Pelegrini Morita, Mark Oremus, Geoffrey T Fong, Peter A Hall
Journal of Medical Internet Research.2020; 22(6): e19930. CrossRef - Pandemia COVID-19, la nueva emergencia sanitaria de preocupación internacional: una revisión
R. Mojica-Crespo, M.M. Morales-Crespo
Medicina de Familia. SEMERGEN.2020; 46: 65. CrossRef - COVID-19 in the radiology department: What radiographers need to know
N. Stogiannos, D. Fotopoulos, N. Woznitza, C. Malamateniou
Radiography.2020; 26(3): 254. CrossRef - Promoting Physical Activity During the COVID-19 Pandemic: Implications for Obesity and Chronic Disease Management
Geoffrey M. Hudson, Kyle Sprow
Journal of Physical Activity and Health.2020; 17(7): 685. CrossRef - The DOSMD challenge and the COVID-19 conundrum
Ravi Philip Rajkumar
Schizophrenia Research.2020; 222: 475. CrossRef - Considerations for safety in the use of systemic medications for psoriasis and atopic dermatitis during theCOVID‐19 pandemic
Jose W. Ricardo, Shari R. Lipner
Dermatologic Therapy.2020;[Epub] CrossRef - Tocilizumab for treatment of patients with severe COVID–19: A retrospective cohort study
Tariq Kewan, Fahrettin Covut, Mohammed J. Al–Jaghbeer, Lori Rose, K.V. Gopalakrishna, Bassel Akbik
eClinicalMedicine.2020; 24: 100418. CrossRef - Environmental concern regarding the effect of humidity and temperature on 2019-nCoV survival: fact or fiction
Narges Nazari Harmooshi, Kiarash Shirbandi, Fakher Rahim
Environmental Science and Pollution Research.2020; 27(29): 36027. CrossRef - Protocol of a population-based prospective COVID-19 cohort study Munich, Germany (KoCo19)
Katja Radon, Elmar Saathoff, Michael Pritsch, Jessica Michelle Guggenbühl Noller, Inge Kroidl, Laura Olbrich, Verena Thiel, Max Diefenbach, Friedrich Riess, Felix Forster, Fabian Theis, Andreas Wieser, Michael Hoelscher, Abhishek Bakuli, Judith Eckstein,
BMC Public Health.2020;[Epub] CrossRef - COVID-19 PANDEMİSİ DÖNEMİNDE ÜLKELERİN COVID-19, SAĞLIK VE FİNANSAL GÖSTERGELER BAĞLAMINDA SINIFLANDIRILMASI: HİYERARŞİK KÜMELEME ANALİZİ
Bilgehan TEKİN
Finans Ekonomi ve Sosyal Araştırmalar Dergisi.2020; 5(2): 336. CrossRef - Epidemiological characteristics of the COVID-19 outbreak in a secondary hospital in Spain
Christine Giesen, Laura Diez-Izquierdo, Carmen María Saa-Requejo, Inmaculada Lopez-Carrillo, Carmen Alejandra Lopez-Vilela, Alicia Seco-Martinez, María Teresa Ramirez Prieto, Eduardo Malmierca, Cristina Garcia-Fernandez
American Journal of Infection Control.2020;[Epub] CrossRef - Accounting for Underreporting in Mathematical Modeling of Transmission and Control of COVID-19 in Iran
Meead Saberi, Homayoun Hamedmoghadam, Kaveh Madani, Helen M. Dolk, Andrei S. Morgan, Joan K. Morris, Kaveh Khoshnood, Babak Khoshnood
Frontiers in Physics.2020;[Epub] CrossRef - Reflecting on the safety zoo: Developing an integrated pandemics barrier model using early lessons from the Covid-19 pandemic
Paul Lindhout, Genserik Reniers
Safety Science.2020; 130: 104907. CrossRef - Novel SARS-CoV-2 outbreak and COVID19 disease; a systemic review on the global pandemic
Abdulmohsen H. Al-Rohaimi, Faisal Al Otaibi
Genes & Diseases.2020; 7(4): 491. CrossRef - Sequential battery of COVID-19 testing to maximize negative predictive value before surgeries
NEERAJ SINHA, GALIT BALAYLA
Revista do Colégio Brasileiro de Cirurgiões.2020;[Epub] CrossRef - How a Barcelona Post-Acute Facility became a Referral Center for Comprehensive Management of Subacute Patients With COVID-19
Marco Inzitari, Cristina Udina, Oscar Len, Joan Ars, Cristina Arnal, Hugo Badani, Vanessa Davey, Ester Risco, Pere Ayats, Ana M. de Andrés, Cristina Mayordomo, Francisco J. Ros, Alessandro Morandi, Matteo Cesari
Journal of the American Medical Directors Associat.2020; 21(7): 954. CrossRef - Prior infection with intestinal coronaviruses moderates symptom severity and mortality in patients with COVID-19: A hypothesis and preliminary evidence
Ravi Philip Rajkumar
Medical Hypotheses.2020; 143: 110116. CrossRef - Spread of variants with gene N hot spot mutations in russian SARS-CoV-2 isolates
SA Kiryanov, TA Levina, MYu Kirillov
Bulletin of Russian State Medical University.2020; (2020(4)): 21. CrossRef - The COVID-19 pandemic: diverse contexts; different epidemics—how and why?
Wim Van Damme, Ritwik Dahake, Alexandre Delamou, Brecht Ingelbeen, Edwin Wouters, Guido Vanham, Remco van de Pas, Jean-Paul Dossou, Por Ir, Seye Abimbola, Stefaan Van der Borght, Devadasan Narayanan, Gerald Bloom, Ian Van Engelgem, Mohamed Ali Ag Ahmed, J
BMJ Global Health.2020; 5(7): e003098. CrossRef - The COVID-19 Pandemic: Diverse Contexts; Different Epidemics—How and Why?
Wim Van Damme, Ritwik Dahake, Alexandre Délamou, Brecht Ingelbeen, Edwin Wouters, Guido Vanham, Remco van de Pas, Jean-Paul Dossou, Por Ir, Seye Abimbola, Stefaan Van der Borght, Narayanan Devadasan, Gerald Bloom, Ian Van Engelgem, Mohamed Ali Ag Ahmed, J
SSRN Electronic Journal .2020;[Epub] CrossRef - Promising effects of tocilizumab in COVID-19: A non-controlled, prospective clinical trial
Farzaneh Dastan, Ali Saffaei, Sara Haseli, Majid Marjani, Afshin Moniri, Zahra Abtahian, Atefeh Abedini, Arda Kiani, Sharareh Seifi, Hamidreza Jammati, Seyed Mohammad Reza Hashemian, Mihan Pourabdollah Toutkaboni, Alireza Eslaminejad, Jalal Heshmatnia, Mo
International Immunopharmacology.2020; 88: 106869. CrossRef - Obese communities among the best predictors of COVID-19-related deaths
Antoine Fakhry AbdelMassih, Ramy Ghaly, Abeer Amin, Amr Gaballah, Aya Kamel, Bassant Heikal, Esraa Menshawey, Habiba-Allah Ismail, Hend Hesham, Josephine Attallah, Kirollos Eshak, Mai Moursi, Mariam Khaled-Ibn-ElWalid, Marwa Tawfik, Mario Tarek, Mayan Moh
Cardiovascular Endocrinology & Metabolism.2020; 9(3): 102. CrossRef - A Japanese case of COVID‐19: An autopsy report
Koji Okudela, Hiroyuki Hayashi, Yukihiro Yoshimura, Hiroaki Sasaki, Hiroshi Horiuchi, Nobuyuki Miyata, Natsuo Tachikawa, Yuki Tsuchiya, Hideaki Mitsui, Kenichi Ohashi
Pathology International.2020; 70(10): 820. CrossRef - Innate Immune Responses to Highly Pathogenic Coronaviruses and Other Significant Respiratory Viral Infections
Hanaa Ahmed-Hassan, Brianna Sisson, Rajni Kant Shukla, Yasasvi Wijewantha, Nicholas T. Funderburg, Zihai Li, Don Hayes, Thorsten Demberg, Namal P. M. Liyanage
Frontiers in Immunology.2020;[Epub] CrossRef - Assessment of Epidemiological Determinants of COVID-19 Pandemic Related to Social and Economic Factors Globally
Mohammad Mahmudul Hassan, Md. Abul Kalam, Shahanaj Shano, Md. Raihan Khan Nayem, Md. Kaisar Rahman, Shahneaz Ali Khan, Ariful Islam
Journal of Risk and Financial Management.2020; 13(9): 194. CrossRef - Pathophysiology and treatment strategies for COVID-19
Manoj Kumar, Souhaila Al Khodor
Journal of Translational Medicine.2020;[Epub] CrossRef - Laboratory biosafety measures involving SARS-CoV-2 and the classification as a Risk Group 3 biological agent
Alexa M. Kaufer, Torsten Theis, Katherine A. Lau, Joanna L. Gray, William D. Rawlinson
Pathology.2020; 52(7): 790. CrossRef - Molecular epidemiology of the first wave of severe acute respiratory syndrome coronavirus 2 infection in Thailand in 2020
Jiratchaya Puenpa, Kamol Suwannakarn, Jira Chansaenroj, Pornjarim Nilyanimit, Ritthideach Yorsaeng, Chompoonut Auphimai, Rungrueng Kitphati, Anek Mungaomklang, Amornmas Kongklieng, Chintana Chirathaworn, Nasamon Wanlapakorn, Yong Poovorawan
Scientific Reports.2020;[Epub] CrossRef - Can climatic factors explain the differences in COVID-19 incidence and severity across the Spanish regions?: An ecological study
Pedro Muñoz Cacho, José L. Hernández, Marcos López-Hoyos, Víctor M. Martínez-Taboada
Environmental Health.2020;[Epub] CrossRef - A comprehensive review about SARS-CoV-2
SK Manirul Haque, Omar Ashwaq, Abdulla Sarief, Abdul Kalam Azad John Mohamed
Future Virology.2020; 15(9): 625. CrossRef - Harnessing Recent Advances in Synthetic DNA and Electroporation Technologies for Rapid Vaccine Development Against COVID-19 and Other Emerging Infectious Diseases
Ziyang Xu, Ami Patel, Nicholas J. Tursi, Xizhou Zhu, Kar Muthumani, Daniel W. Kulp, David B. Weiner
Frontiers in Medical Technology.2020;[Epub] CrossRef - COVID-19 Patients: A Systematic Review and Meta-Analysis of Laboratory Findings, Comorbidities, and Clinical Outcomes Comparing Medical Staff versus the General Population
Mina Ebrahimi, Amal Saki Malehi, Fakher Rahim
Osong Public Health and Research Perspectives.2020; 11(5): 269. CrossRef - The Relationship Between Demographic, Socioeconomic, and Health-Related Parameters and the Impact of COVID-19 on 24 Regions in India: Exploratory Cross-Sectional Study
Ravi Philip Rajkumar
JMIR Public Health and Surveillance.2020; 6(4): e23083. CrossRef - Coronavirus Disease 2019 (COVID-19): A Modeling Study of Factors Driving Variation in Case Fatality Rate by Country
Jennifer Pan, Joseph Marie St. Pierre, Trevor A. Pickering, Natalie L. Demirjian, Brandon K.K. Fields, Bhushan Desai, Ali Gholamrezanezhad
International Journal of Environmental Research an.2020; 17(21): 8189. CrossRef - Investigating duration and intensity of Covid-19 social-distancing strategies
C. Neuwirth, C. Gruber, T. Murphy
Scientific Reports.2020;[Epub] CrossRef - Survival and Estimation of Direct Medical Costs of Hospitalized COVID-19 Patients in the Kingdom of Saudi Arabia
Anas Khan, Yazed AlRuthia, Bander Balkhi, Sultan Alghadeer, Mohamad-Hani Temsah, Saqer Althunayyan, Yousef Alsofayan
International Journal of Environmental Research an.2020; 17(20): 7458. CrossRef - Time dynamics of COVID-19
Cody Carroll, Satarupa Bhattacharjee, Yaqing Chen, Paromita Dubey, Jianing Fan, Álvaro Gajardo, Xiner Zhou, Hans-Georg Müller, Jane-Ling Wang
Scientific Reports.2020;[Epub] CrossRef - https://www.crossref.org/webDeposit/
Betsy Varghese, Siba Shajahan, Harikrishnan Anilkumar, Retheesh K. Haridasan, Arya Rahul, Hariprasad Thazhathedath, Anish T. Surendran Nair
Journal of Evolution of Medical and Dental Science.2020; 9(46): 3411. CrossRef - COVID-19: Spatial analysis of hospital case-fatality rate in France
Marc Souris, Jean-Paul Gonzalez, Muhammad Adrish
PLOS ONE.2020; 15(12): e0243606. CrossRef - Investigating the Determinants of High Case-Fatality Rate for Coronavirus Disease 2019 in Italy
Francesco Barone-Adesi, Luca Ragazzoni, Maurizio Schmid
Disaster Medicine and Public Health Preparedness.2020; 14(4): e1. CrossRef - Riesgos, contaminación y prevención frente al COVID-19 en el quehacer odontológico: una revisión
Paul Martin Herrera-Plasencia, Erika Raquel Enoki-Miñano, Miguel Angel Ruiz-Barrueto
Revista de Salud Pública.2020; 22(5): 1. CrossRef - Environmental Concern Regarding the Effect of Humidity and Temperature on SARS-COV-2 (COVID-19) Survival: Fact or Fiction
Narges Nazari Harmooshi, Kiarash Shirbandi, Fakher Rahim
SSRN Electronic Journal .2020;[Epub] CrossRef - COVID-19 Infection in Medical Staffs versus Patients: A Systematic Review and Meta-analysis of Laboratory Findings, Comorbidities, and Clinical Outcome
Mina Ebrahimi, Amal Saki Malehi, Fakher Rahim
SSRN Electronic Journal .2020;[Epub] CrossRef - Infectious diseases epidemiology, quantitative methodology, and clinical research in the midst of the COVID-19 pandemic: Perspective from a European country
Geert Molenberghs, Marc Buyse, Steven Abrams, Niel Hens, Philippe Beutels, Christel Faes, Geert Verbeke, Pierre Van Damme, Herman Goossens, Thomas Neyens, Sereina Herzog, Heidi Theeten, Koen Pepermans, Ariel Alonso Abad, Ingrid Van Keilegom, Niko Speybroe
Contemporary Clinical Trials.2020; 99: 106189. CrossRef - Elective Surgery during SARS-Cov-2/COVID-19 Pandemic: Safety Protocols with Literature Review
Lázaro Cárdenas-Camarena, Jorge Enrique Bayter-Marin, Héctor Durán, Alfredo Hoyos, César Octavio López-Romero, José Antonio Robles-Cervantes, Ernesto Eduardo Echeagaray-Guerrero
Plastic and Reconstructive Surgery - Global Open.2020; 8(6): e2973. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


