Insufficient weight management in pregnant women with gestational diabetes mellitus
Article information

Abstract
Objectives
This study investigated whether weight was managed appropriately in pregnant women with gestational diabetes mellitus (GDM) and examined the association between insufficient gestational weight gain (GWG) and adverse pregnancy outcomes.
Methods
The study included 235 pregnant women with GDM from the Korean Pregnancy Outcome Study. GWG from the second to the third trimester (kg/wk ) and total GWG (kg) were classified as insufficient, appropriate, or excessive according to the 2009 Institute of Medicine guidelines. Adverse pregnancy outcomes included maternal (hypertensive disorders of pregnancy, preterm birth, cesarean delivery, and delivery complications) and infant (low birth weight, high birth weight, neonatal intensive care unit admission, and congenital anomalies) outcomes.
Results
The proportion of pregnant women with GDM who had insufficient GWG from the second to the third trimester was 52.3%, and that of participants with total insufficient GWG was 48.1%. There were no significant associations between insufficient GWG from the second to the third trimester and adverse pregnancy outcomes. Participants with total insufficient GWG had a significantly lower risk of preterm birth (odds ratio [OR], 0.17; 95% confidence interval [CI], 0.05–0.60) and high birth weight (OR, 0.23; 95% CI, 0.07–0.80).
Conclusion
Our findings suggest the importance of appropriate weight management and the need for GWG guidelines for pregnant women with GDM.

Introduction
Gestational diabetes mellitus (GDM) is a common pregnancy-related complication with a prevalence of 11.5% in Asian populations [1]. GDM has been associated with adverse maternal and neonatal outcomes, including preeclampsia, cesarean delivery, macrosomia, hyperbilirubinemia, and neonatal hypoglycemia [2,3]; it has also been associated with maternal diabetes development after delivery [4]. Therefore, attention and management are needed to prevent GDM and reduce GDM-related complications.
GDM is known to be more common in pregnant women who were overweight or obese before pregnancy, or who gained excessive weight during pregnancy [5,6]. In addition, a cohort study reported that excessive gestational weight gain (GWG) in pregnant women with GDM might further increase the risk of adverse pregnancy outcomes, such as hypertensive disorders of pregnancy (HDP), cesarean delivery, and macrosomia [7]. Therefore, pregnant women with GDM are encouraged to avoid excessive GWG during and after pregnancy to improve outcomes for both the mother and the newborn.
Our previous study found that insufficient GWG was significantly related to the risk of GDM, and suggested that it might be because pregnant women diagnosed with GDM paid more attention to weight control, including diet and physical activity, during the remainder of their pregnancy [8]. Another study showed that half of women with GDM had insufficient GWG, which was associated with an increased risk of preterm birth or respiratory distress in the infant [9]. Similarly, a previous study of pregnant women with GDM suggested that a total GWG below the Institute of Medicine (IOM) guidelines increased the risk of preterm birth and small for gestational age infants and decreased the risk of large for gestational age infants [7]. Nevertheless, few studies have examined the effects of insufficient GWG on pregnancy outcomes in pregnant women with GDM.
In this study, we investigated whether weight was managed appropriately, according to the IOM guidelines, in pregnant women with GDM and studied the association between insufficient GWG after the diagnosis of GDM or total insufficient GWG and adverse pregnancy outcomes.
Materials and Methods
Study Design and Participants
This study analyzed data from pregnant women who participated in the Korean Pregnancy Outcome Study (KPOS), a prospective cohort study, conducted by Cheil General Hospital & Women’s Healthcare Center and CHA Gangnam Medical Center between March 2013 and January 2017 [10]. Pregnant women participated in 5 visits: around 12, 24, and 36 weeks, at the end of pregnancy, and 4 to 6 weeks postpartum, with interview-based questionnaires and clinical assessments at each visit. Of the 3,232 participants, 235 pregnant women (7.3%) were diagnosed with GDM, after the exclusion of participants who had twin pregnancies; lacked information on socioeconomic, psychological, behavioral, and medical histories; or lacked information on reproductive factors, trimester-specific gestational weight, and pregnancy outcomes. Screening for GDM was performed as follows: (1) a 50-g glucose challenge test (GCT) between 24 and 28 weeks, and (2) an oral glucose tolerance test (OGTT) if the result of the GCT was ≥140 mg/dL. GDM was diagnosed by Cheil General Hospital using a 75-g OGTT based on new criteria from the International Association of Diabetes and Pregnancy Study Group and by CHA Gangnam Medical Center using a 100-g OGTT based on the Carpenter-Coustan criteria [10].
Ethics Statement
The study protocol was approved by the Institutional Review Board (IRB) of Cheil General Hospital (IRB No: CGH-IRB-2013-10), CHA Gangnam Medical Center (IRB No: 2013-14-KNC13018), and the Korea National Institute of Health, Korea Disease Control and Prevention Agency (IRB No: 2021-04-02-1C-A). All participants provided written informed consent, and this was confirmed by the IRB.
Prepregnancy Body Mass Index and GWG
The weight and height of the participants were measured, using standard procedures, in units of 0.1 kg on a digital scale and 0.1 cm on a stadiometer, respectively, while participants wore light clothes and were barefoot. Prepregnancy weight was self-reported at visit 1 (during the first trimester), and gestational weight in the second and the third trimesters and total GWG were measured at visits 2, 3, and 4, respectively. Prepregnancy body mass index (BMI) was calculated by dividing the prepregnancy weight by the height squared (kg/m2) and categorized as underweight (<18.5 kg/m2), normal weight (18.5–25.0 kg/m2), or obese (≥25.0 kg/m2) [11]. GWG was considered as weight gain (kg/wk ) from the second to the third trimester and total weight gain (kg) and classified into 3 categories (insufficient, appropriate, and excessive), considering prepregnancy BMI and gestational age according to the 2009 IOM guidelines for weight gain during pregnancy (Figure S1) [12].
Adverse Pregnancy Outcomes
Adverse pregnancy outcomes included maternal and infant outcomes. The maternal outcomes were HDP, preterm birth, cesarean delivery, and delivery complications; the infant outcomes were low birth weight, high birth weight, neonatal intensive care unit (NICU) admission, and congenital anomalies. HDP was defined as any of the following: gestational hypertension, preeclampsia, eclampsia, or superimposed preeclampsia. Gestational hypertension was diagnosed as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg without proteinuria, developing after 20 weeks of gestation. Preeclampsia was diagnosed as gestational hypertension with either proteinuria (≥0.3 g of protein in a 24-hour urine collection or ≥1+ on a semi-quantitative dipstick test) or signs of end-organ dysfunction after 20 weeks of gestation, with one of the following: (1) platelet count >100,000/mm3, (2) creatinine level >1.1 mg/dL, (3) elevated serum transaminase, (4) pulmonary edema, or (5) neurologic symptoms. Eclampsia was diagnosed as seizures unrelated to other cerebral conditions in pregnant women with preeclampsia, and superimposed preeclampsia was diagnosed as the development of preeclampsia symptoms in pregnant women with chronic hypertension [13]. Preterm birth was defined as a gestational age <37 weeks at birth. Delivery complications were defined as any of the following: shoulder dystocia, premature rupture of membranes, placental abruption, parturient canal, or uterine rupture at delivery. Low birth weight was defined as <2,500 g at birth; high birth weight was defined as ≥4,000 g.
Socioeconomic, Behavioral, Mental Health, and Reproductive Factors
Socioeconomic factors included maternal age at visit 1 (year), educational status, and household income. Educational status was categorized as ≤ high school, college or university, or ≥ graduate school. Household income was categorized as <3, 3–5, or ≥5 million Korean won (KRW)/month. Behavioral factors included BMI (continuous [kg/m2] or categorical), smoking status, and physical activity. BMI was classified as nonobese (underweight and normal weight) or obese, because the proportion of prepregnancy underweight was too small for separate inclusion in the analysis (4.7%). Participants were classified by smoking status as nonsmokers or former/current smokers. Physical activity was categorized as low, moderate, or high using the International Physical Activity Questionnaire [14]. Mental health factors included stress and depressive symptoms. Stress was investigated using a visual analog scale (score, 0–10). Depressive symptoms were defined using the Edinburgh postnatal depression scale [15] and categorized as no (<10) or yes (≥10). Reproductive factors included parity (<1 or ≥1 times) and history of GDM (no or yes).
Statistical Analysis
The baseline characteristics of participants and adverse pregnancy outcomes according to GWG from the second to the third trimester or total GWG, were compared using one-way analysis of variance (ANOVA) followed by the Scheffé test for multiple comparisons of continuous variables and the chi-square test for categorical variables. Data are presented as mean±standard deviation (SD) and frequency (%). The odds ratios (ORs) and 95% confidence intervals (CIs) of adverse pregnancy outcomes, associated with GWG from the second to the third trimester or total GWG, were evaluated using multivariable logistic regression. All statistical analyses were conducted using SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA), and a two-sided p-value <0.05 was considered to indicate statistical significance.
Results
The values for GWG from prepregnancy to delivery in pregnant women with GDM are presented in Figure 1. The cumulative mean GWG is shown in Figure 1A. The mean±SD of GWG per week from the second to the third trimester was 0.29±0.22 kg/wk , which was lower than the corresponding value of 0.36±0.26 kg/wk from the first to the second trimester (Figure 1B).
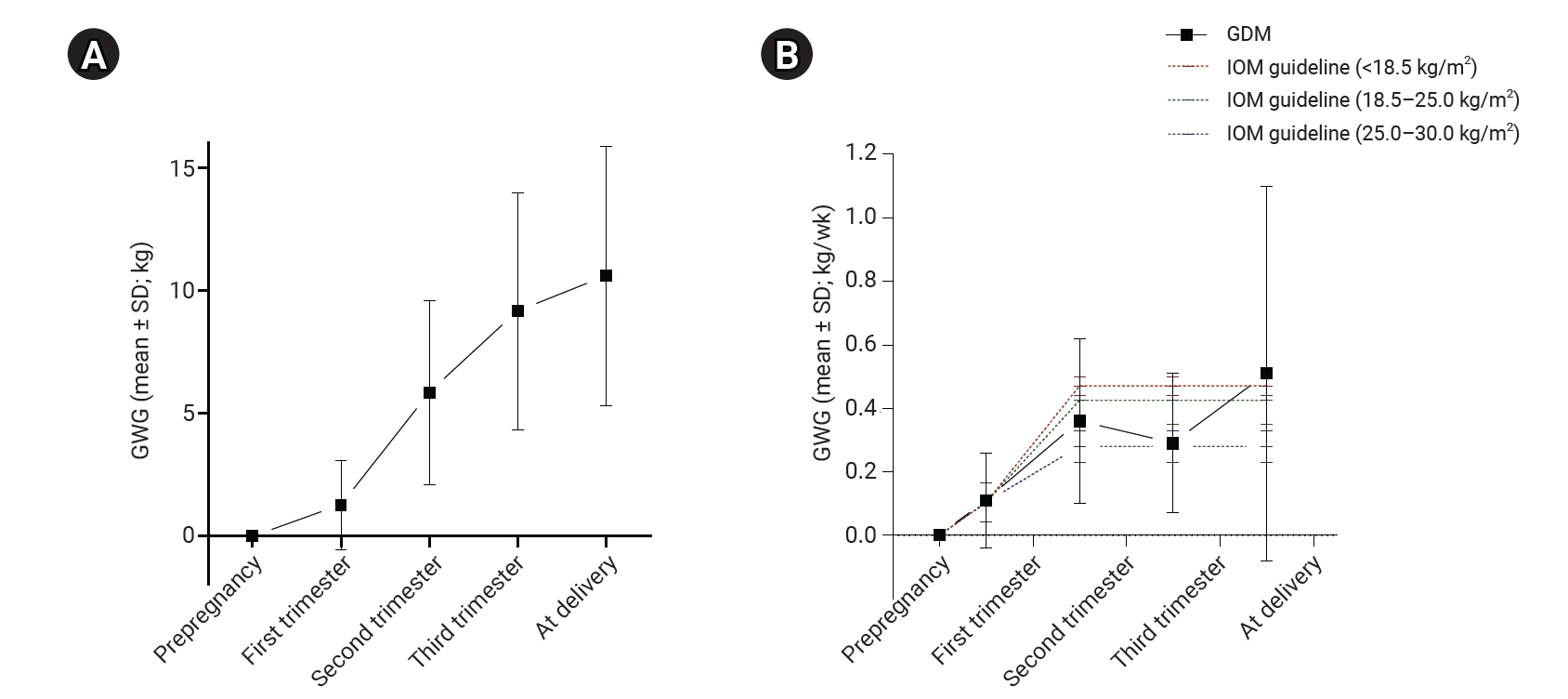
Gestational weight gain from prepregnancy to delivery in pregnant women with gestational diabetes mellitus. (A) Cumulative mean of gestational weight gain (kg). (B) Rates of gestational weight gain (kg/wk).
GDM, gestational diabetes mellitus; IOM, Institute of Medicine; GWG, gestational weight gain; SD, standard deviation.
The baseline (at visit 1) characteristics of pregnant women with GDM, according to GWG from the second to the third trimester, are presented in Table 1. The GWG was insufficient in 52.3% (n=123), appropriate in 28.9% (n=68), and excessive in 18.7% (n=44). The proportion of individuals with household income <3 million KRW per month was highest among pregnant women with excessive GWG, but this relationship was not statistically significant (p=0.072). The total GWG (kg) became significantly higher as GWG changed from insufficient to excessive. The baseline characteristics according to total GWG are presented in Table S1. The proportions of nonobese and depressive symptoms were significantly higher among pregnant women with insufficient GWG. The proportion of former or current smokers became significantly higher as total GWG changed from insufficient to excessive.

Baseline characteristics of participants according to gestational weight gain from the second to the third trimester in pregnant women with gestational diabetes mellitus
GWG from the second to the third trimester and total GWG according to prepregnancy BMI are presented in Figure 2. The proportion of women with insufficient GWG from the second to third trimester was higher than that of women with appropriate or excessive GWG among both prepregnancy BMI groups (nonobese and obese: 55.4% and 44.9%, respectively). The proportions of women with total insufficient GWG were 54.8% and 31.9% in the prepregnancy nonobese and obese groups, respectively.
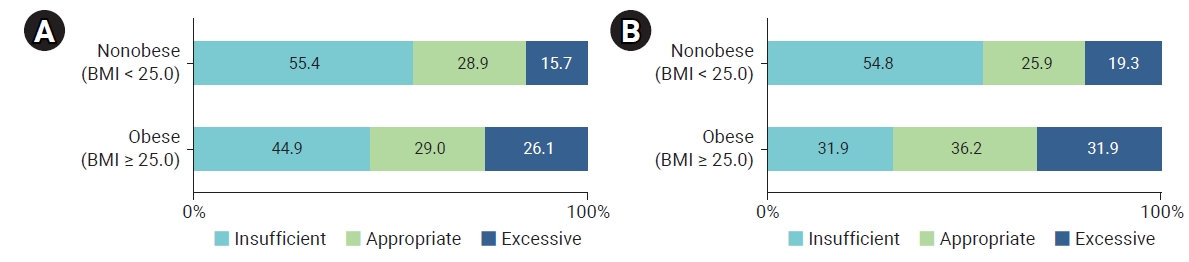
Gestational weight gain according to the prepregnancy body mass index (BMI; kg/m2) in pregnant women with gestational diabetes mellitus. (A) Gestational weight gain from second to third trimester. (B) Total gestational weight gain.
The adverse pregnancy outcomes according to GWG from the second to the third trimester are presented in Table 2. The proportion of any adverse maternal outcomes, cesarean delivery, and high birth weight gradually increased as GWG changed from insufficient to excessive, but these relationships were not statistically significant (p=0.051, p=0.058, and p=0.098, respectively). In pregnant women who were nonobese before pregnancy (Table S2), the proportion of HDP and cesarean delivery gradually increased as GWG changed from insufficient to excessive (p=0.018 and p=0.029, respectively). However, no statistically significant difference was found in pregnant women who were obese before pregnancy (Table S3).

Adverse pregnancy outcomes according to gestational weight gain from the second to the third trimester in pregnant women with gestational diabetes mellitus
Adverse pregnancy outcomes according to total GWG are presented in Table 3. The proportion of HDP significantly increased as GWG changed from insufficient to excessive, but there were too few cases for a statistically meaningful analysis. The proportion of preterm birth was significantly higher in the appropriate GWG group, and the proportion of high birth weight was significantly lower in the insufficient GWG group. Although not statistically significant, the proportion of delivery complications was higher in women with insufficient and excessive GWG than in those with appropriate GWG. The results of the stratified analysis by prepregnancy BMI are presented in Tables S4 and S5. The proportion of HDP and high birth weight gradually increased as GWG changed from insufficient to excessive (p=0.015 and p=0.029, respectively) in pregnant women who were nonobese before pregnancy (Table S4).

Adverse pregnancy outcomes according to total gestational weight gain in pregnant women with gestational diabetes mellitus
The risk of adverse pregnancy outcomes according to GWG from the second to the third trimester is presented in Table 4. There were no significant associations between insufficient GWG and any adverse pregnancy outcomes. Excessive GWG was positively associated with all adverse pregnancy outcomes, except for any adverse infant outcomes and NICU admission (vs. appropriate GWG; all ORs >1.00), but these associations were not statistically significant. Low birth weight and congenital anomalies were excluded from the analysis because there were no cases in the excessive GWG group,.

ORs (95% CIs) for adverse pregnancy outcomes according to gestational weight gain from the second to the third trimester in pregnant women with gestational diabetes mellitus
The risk of adverse pregnancy outcomes according to total GWG is presented in Table 5. The ORs for preterm birth and high birth weight in the insufficient GWG, compared to appropriate GWG, were 0.17 (95% CI, 0.05–0.60) and 0.23 (95% CI, 0.07–0.80), respectively. There were no significant associations between excessive GWG and all adverse pregnancy outcomes. HDP, low birth weight, and congenital anomalies were excluded from the analysis because there were no HDP cases in the insufficient GWG groups, no low birth weight cases in the appropriate GWG group, and no congenital anomalies in the excessive GWG group.

ORs (95% CIs) for adverse pregnancy outcomes according to total gestational weight gain in pregnant women with gestational diabetes mellitus
Discussion
Although weight management in pregnant women with GDM is very important to improve pregnancy outcomes, our study showed that the proportion of participants with insufficient GWG was higher than that of participants with appropriate or excessive GWG. In particular, more than 50.0% of pregnant women who were nonobese before pregnancy had insufficient GWG. Furthermore, we found that insufficient GWG from the second to the third trimester may not reduce or increase the risk of adverse pregnancy outcomes, but total insufficient GWG may reduce the risk of preterm birth and high birth weight.
GDM is defined as the presence of impaired glucose metabolism first recognized during pregnancy [16]. Many previous studies have reported that sociodemographic factors, such as late-age pregnancy and family history of diabetes, and reproductive factors, including a history of GDM, parity, and polycystic ovary syndrome, are risk factors that increase the risk of GDM [1,3,17]. In addition, obesity and excess GWG are critical risk factors for GDM. A meta-analysis found that obese pregnant women had a significantly higher risk of GDM than those of normal weight (OR, 3.56; 95% CI, 3.05–4.21) [6], and a Chinese study found that excessive GWG increased the risk of GDM in all categories of BMI [18].
GDM is one of the main risk factors for adverse pregnancy outcomes, including cesarean delivery, macrosomia, and hyperbilirubinemia, and it is also a risk factor for maternal diabetes after delivery [2–4]. It has also been reported that excessive GWG in pregnant women with GDM leads to markedly negative outcomes for both mothers and their offspring. A retrospective cohort study suggested that total GWG above the IOM cut-off in pregnant women with GDM might increase the risk of cesarean delivery (OR, 1.34; 95% CI, 1.04–1.72), HDP (OR, 2.00; 95% CI, 1.28–3.12), and other adverse outcomes, including preeclampsia and macrosomia; furthermore, GWG above the IOM cut-off in the third trimester could increase the risk of HDP (OR, 1.93; 95% CI, 1.08–2.98) [7]. This is consistent with our results: a high proportion of adverse outcomes, such as HDP, cesarean delivery, and high birth weight, was noted in pregnant women with GDM who had excessive GWG. However, we found no significant association between excessive GWG and adverse pregnancy outcomes.
To date, few studies have investigated the effects of insufficient GWG because most have focused on the health effects of excessive weight gain in pregnant women with GDM. Therefore, it is hypothesized that pregnant women with GDM avoid weight gain after being diagnosed with GDM. In our study, we examined whether weight management in pregnant women with GDM participating in the cohort was conducted appropriately, according to the IOM guidelines. As expected, most women did not manage their weight according to the guidelines. Comparing pregnant women with GDM to those without GDM (n=2,997), GWG was similar (slightly higher in women with GDM) until the first trimester, but this pattern changed from the first to the second trimester and GWG was significantly lower in both the second (before or after the diagnosis of GDM) and third trimesters (p<0.001 for both; data not shown). In addition, the proportion of participants with insufficient GWG was higher in pregnant women with GDM than in those without GDM (data not shown). In our study, the rate of total insufficient GWG was 48.1%, which was higher than the 26.2% reported in a Chinese study [19] and lower than the 50.3% reported in a Spanish study [9]; the rate of total insufficient GWG in obese women was 31.9%, which was lower than the 34.5% reported in a Portuguese study [20].
When comparing adverse pregnancy outcomes according to GWG from the second to the third trimester, the proportion of any adverse maternal outcomes, cesarean delivery, and high birth weight gradually increased from insufficient to excessive GWG; nonetheless, these differences were only marginally significant (p<0.1 for all). In an analysis stratified by prepregnancy BMI, the proportion of HDP and cesarean delivery significantly increased from insufficient to excessive GWG in pregnant women who were nonobese before pregnancy. However, there were no statistically significant differences in those who were obese before pregnancy. When comparing adverse pregnancy outcomes according to total GWG, significant differences were found in the proportions of HDP, preterm birth, and high birth weight. However, the proportions of HDP and high birth weight were significantly different only in pregnant women who were nonobese before pregnancy. Because the effect of GWG on adverse pregnancy outcomes may vary with prepregnancy BMI, further large-scale studies, stratified by prepregnancy BMI, will be needed.
We also examined the associations between insufficient GWG in pregnant women with GDM and adverse pregnancy outcomes. In the analysis of associations between GWG from the second to the third trimester and adverse pregnancy outcomes, we did not find that insufficient GWG reduced or increased the risk of adverse pregnancy outcomes. Similarly, although all adverse pregnancy outcomes, except for any adverse infant outcomes and NICU admission, showed positive trends with excessive GWG (vs. appropriate GWG), none of the associations were statistically significant. Nevertheless, this is consistent with a previous Chinese study’s results showing that insufficient GWG after a GDM diagnosis had no beneficial or adverse effects on adverse perinatal outcomes [19]. In the analysis of the associations between total GWG and adverse pregnancy outcomes, we found that insufficient GWG may reduce the risk of preterm birth and high birth weight. Excessive GWG showed no significant associations with adverse pregnancy outcomes. However, our study population was too small for the results to be reliable. Contrary to our results, a Chinese study reported that insufficient GWG was associated with an increased risk of preterm birth (OR, 1.52; 95% CI, 1.12–2.05) and small for gestational age infants (OR, 1.21; 95% CI, 1.10–1.69) [7]. Similarly, a retrospective cohort study also suggested that total insufficient GWG was associated with neonatal hypocalcemia (adjusted OR, 4.56; 95% CI, 1.04–20.00), in addition to preterm birth (unadjusted OR, 2.03; 95% CI, 1.55–2.83) [9]. A study in Hong Kong found that insufficient GWG was associated with insulin resistance and hypertension in offspring (7 years of age) [21].
Another matter of debate is the application of the IOM guidelines to pregnant women with GDM. Previous studies have reported that new GWG guidelines should be applied to pregnant women with GDM. A cohort study in Australia evaluated a new standard by subtracting 2 kg from the upper/lower limits of the IOM guidelines [22], and another cohort study in China evaluated new targets using receiver operating characteristic curves [23]. Therefore, to determine the short- and long-term effects of insufficient GWG on mothers and their offspring and to provide correct GWG guidelines for pregnant women with GDM, further longitudinal cohort or interventional studies of pregnant women with GDM are needed.
This study has some limitations. First, the small sample size of our study may not have provided sufficient statistical power to investigate associations between GWG and adverse pregnancy outcomes in pregnant women with GDM. In addition, our study population consisted of only Korean making it difficult to generalize the results. Therefore, large-scale studies of the general population that include various races/ethnicities with sufficient statistical power are needed. Second, there was a possibility of bias because the prepregnancy weight was self-reported. However, since it was measured in the first trimester, when the weight change was small, the bias was not expected to be large. In addition, although most of the weight measurements in the second trimester were made at or after the diagnosis of GDM, some participants’ measurements obtained before the diagnosis of GDM were also included. Since the screening for GDM was performed between 24 and 28 weeks, and the weight in the third trimester was measured around 36 weeks (at visit 3), the timing of measurements most likely was able to sufficiently reflect the weight change after the diagnosis of GDM. Finally, we used the IOM guidelines for GWG. Since the IOM guidelines are mainly intended for use among Caucasians, their appropriateness for Asian women is debatable. As the GWG guidelines for pregnant women have not been established for Asians, research on GWG guidelines suitable for Asians is needed in the future. Nevertheless, an important strength of the present study is that it is the first to investigate the current status of weight control and the associations of GWG after diagnosis of GDM and total GWG with adverse pregnancy outcomes in Korean pregnant women with GDM.
Conclusion
In this study, we found that the majority of pregnant women with GDM had GWG below the IOM guideline criteria either from the second to the third trimester or during the full pregnancy. Furthermore, we found that total insufficient GWG may reduce the risk of preterm birth and high birth weight, but insufficient GWG from the second to the third trimester (mostly after diagnosis of GDM) may not have a beneficial or adverse association with adverse pregnancy outcomes. Our findings suggest the need for GWG guidelines and appropriate weight management for pregnant women with GDM.
Supplementary Material
Figure S1. Detailed criteria and guidelines for gestational weight gain; Table S1. Baseline characteristics of participants according to total gestational weight gain in pregnant women with gestational diabetes mellitus; Table S2. Adverse pregnancy outcomes according to gestational weight gain from second to third trimester in pregnant women who were prepregnancy nonobese; Table S3. Adverse pregnancy outcomes according to gestational weight gain from second to third trimester in pregnant women who were prepregnancy obese; Table S4. Adverse pregnancy outcomes according to total gestational weight gain in pregnant women who were prepregnancy nonobese; Table S5. Adverse pregnancy outcomes according to total gestational weight gain in pregnant women who were prepregnancy obese. Supplementary data are available at https://doi.org/10.24171/j.phrp.2022.0182.
Detailed criteria and guidelines for gestational weight gain.
GWG, gestational weight gain; BMI, body mass index.
Baseline characteristics of participants according to total gestational weight gain in pregnant women with gestational diabetes mellitus
Adverse pregnancy outcomes according to gestational weight gain from second to third trimester in pregnant women who were prepregnancy nonobese
Adverse pregnancy outcomes according to gestational weight gain from second to third trimester in pregnant women who were prepregnancy obese
Adverse pregnancy outcomes according to total gestational weight gain in pregnant women who were prepregnancy nonobese
Adverse pregnancy outcomes according to total gestational weight gain in pregnant women who were prepregnancy obese
Notes
Ethics Approval
The study protocol was approved by the IRB of Cheil General Hospital (IRB No: CGH-IRB-2013-10), CHA Gangnam Medical Center (IRB No: 2013-14-KNC13018), and the Korea National Institute of Health, Korea Disease Control and Prevention Agency (KDCA) (IRB No: 2021-04-02-1C-A). All participants provided written informed consent, and it was confirmed by the IRB.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
This study was supported by the Korea National Institute of Health, KDCA (grant number: 2021-NI-015-01).
Availability of Data
The Korean Pregnancy Outcome Study (KPOS) data are available from the Korea National Institute of Health, KDCA.
Authors’ Contributions
Conceptualization: all authors; Data curation: KH, HYP; Formal analysis: KH; Investigation: KH, HYP; Methodology: KH, DWK, HMR, HYP; Project administration: KH, HYP; Resources: all authors; Software: KH; Supervision: HYP; Validation: KH, HYP; Visualization: KH, HYP; Writing-original draft: KH; Writing-review & editing: all authors.
Additional Contributions
We sincerely thank Cheil General Hospital & Women’s Healthcare Center and CHA Gangnam Medical Center for participating in the KPOS study.