Cardiovascular Disease Risk Factors and Obesity Levels in Korean Adults: Results from the Korea National Health and Nutrition Examination Survey, 2007–2015
Article information
Abstract
Objectives
The increase in the obesity rate in adult males in Korea is higher than countries in the Organization for Economic Co-operation and Development and other Asian countries. We examined the trends and prevalence of major risk factors for cardiovascular disease by evaluating the weight status amongst adults from 2007 to 2015.
Methods
The study included 37,402 adults, who participated in the Korea National Health and Nutrition Examination Survey. The prevalence trends of cardiovascular disease risk factors were estimated for each body mass index group.
Results
From 2007 to 2015, significant increases in the prevalence of hypertension, diabetes, and hypercholesterolemia were observed in normal weight adults (0.03 percentage point (%p), 0.06%p, and 0.13%p, respectively). Amongst the overweight and obese adults, a significant increase in the prevalence of hypercholesterolemia was observed, During this period, the prevalence of smoking decreased amongst obese adults and no significant changes in drinking habits and physical activity were noted across all body mass index groups.
Conclusion
The prevalence of obesity in Korean adults is increasing, and it is necessary to implement interventions to prevent further weight gain and obesity-associated cardiovascular disease.
Introduction
Obesity is defined as an abnormal or excessive accumulation of fat that may impair health [1]. Upper-body obesity, especially with increased visceral fat is associated with hypertension, insulin resistance, dyslipidemia, Type 2 diabetes, and premature death resulting from coronary disease [2]. In 2015, around a third (39.6% of males and 28.8% of females) of adults in Korea over the age of 19, were either overweight or obese [body mass index (BMI) ≥ 25 kg/m2 [3]. There is evidence that being overweight and obesity among adults is associated with an increased risk of cardiovascular disease (CVD) [4,5] and diabetes [6], respectively. Obesity not only increases the risk of coronary artery disease by 50%, but it also increases the risk of CVD and coronary artery disease mortality rate by 50% [7–9]. Analyses of National Health and Nutrition Examination Survey III (NHANES III) data from the United States, showed increased prevalence ratios when the severity of obesity and being overweight increased, for example high blood pressure (BP) [10]. It was also reported that higher prevalence ratios for high blood cholesterol were present amongst the overweight and the obese compared with people with a normal weight [10].
The rate of increase in obesity among adult males in Korea is higher than those reported by the Organization for Economic Co-operation and Development (OECD) countries and other Asian countries [11], but it is unknown whether the health risks associated with a higher weight, will continue to rise. Although there have been previous studies examining the relationship between BMI and CVD risk factors, there have been an inadequate number of studies evaluating the changes in the CVD risk factors by weight status in Korean population. Therefore, this study analyzed data from the Korea National Health and Nutrition Examination Survey (KNHANES), 2007–2015, to examine trends in the prevalence of CVD risk factors by weight status amongst adults in Korea.
Materials and Methods
Data from the KNHANES, conducted by the Korea Centers for Disease Control and Prevention (KCDC), was used in this study. The KNHANES data are open-source files released as de-identified data by the KCDC. The KNHANES was designed to provide nationally representative data to estimate the prevalence of major diseases, and nutritional disorders, and their potential risk factors. The sampling plan followed a complex, stratified, multistage, probability cluster design to produce estimates representative of the noninstitutionalized civilian population. The KNHANES collected data through interviews performed in participants’ homes and conducted medical examinations and laboratory assessments in a mobile examination center. Anthropometric data (i.e. height and weight) in the KNHANES were measured by trained nurses, using a standardized procedure. The health interview and health examination were conducted by trained staff members, including physicians, medical technicians and health interviewers, at a mobile examination center, and dieticians’ visits to the homes of the study participants were followed up. Data from the KNHANES between 2007–2015, with participants aged ≥ 19 years whose complete measurements of CVD risk factors and anthropometry data were available (n = 37,402), was used for analysis in this study.
1. BMI group
BMI groups were defined according to the Asia-Pacific World Health Organization classification standard [12]. Participants were categorized based on their BMI and grouped as; normal weight (18.5 to < 23 kg/m2), overweight (23 to < 25 kg/m2), or obese (≥ 25 kg/m2). Participants who were morbidly obese (≥ 30 kg/m2) were included in the obese category. Underweight participants (BMI < 18.5 kg/m2) were excluded [n = 2,145; (100–350 annually)].
2. CVD risk factors
Six CVD risk factors were evaluated in the analysis: hypertension, diabetes, dyslipidemia, smoking, drinking, and physical activity. Hypertension was defined as having a systolic BP ≥ 140 mmHg or diastolic BP ≥ 90 mmHg or use of antihypertensive medications. Diabetes was defined as having a fasting plasma glucose ≥ 126 mg/dL or diagnosis by a doctor. Type 1 and Type 2 diabetes were not distinguished. Dyslipidemia was defined as hypercholesterolemia (fasting total cholesterol ≥ 240 mg/dL or taking cholesterol medication), hypertriglyceridemia (fasting triglyceride > 200 mg/dL), low high-density lipoprotein (HDL) cholesterol (fasting < 40 mg/dL) or having been diagnosed by a physician.
Current smokers were defined as those who had smoked > 5 packs (100 cigarettes) in their lifetime and currently smoke cigarettes. Monthly drinkers were defined as those who drank more than once a month over the previous year. High-risk drinkers were defined as those who drink more than twice a week, with an average of 7 glasses (5 glasses for women) per session. Physical activity was defined as having a mix of high and medium intensity exercise, with more than 2 hours and 30 minutes of medium-intensity physical activity, or 1 hour and 15 minutes of high-intensity physical activity per week.
3. Statistical analysis
Sample design variables and weights were used to produce nationally representative estimates that accounted for the KNHANES complex survey design, including its stratified multistage cluster sampling. All statistical analyses were conducted using SAS 9.4 (SAS Inc., Cary, NC, USA). The level of statistical significance was set at p < 0.05 and the stability of the estimates reflected by 95% confidence intervals (CIs). The prevalence of each risk factor was calculated as the percentage change overall for each BMI group, while the trend analysis of risk factors for each group according to year, was analyzed. The prevalence of adults with 1, 2, or 3 or more risk factors within each BMI group was also calculated. Furthermore, a logistic regression model was used to compare the prevalence of CVD according to BMI group, to determine odds ratios (ORs) with 95% CIs. Adjusted ORs were calculated according to the percentage change after adjusting for gender, age, education, income, smoking status, alcohol consumption, and physical activity (ORs with 95% CIs).
Results
The general characteristics of the participants by year are reported in Table 1. Overall, there was little change in the demographics from 2007 to 2015. The male to female ratio did not vary greatly during the survey period. Regarding educational level, the ratio of elementary school, middle school, and high school decreased, while the ratio of college graduates increased. Overall, BMI group was higher in the order of normal, obese, and overweight during the survey period, and the prevalence of obese adults increased [33.1–35.8% (Table 1)].
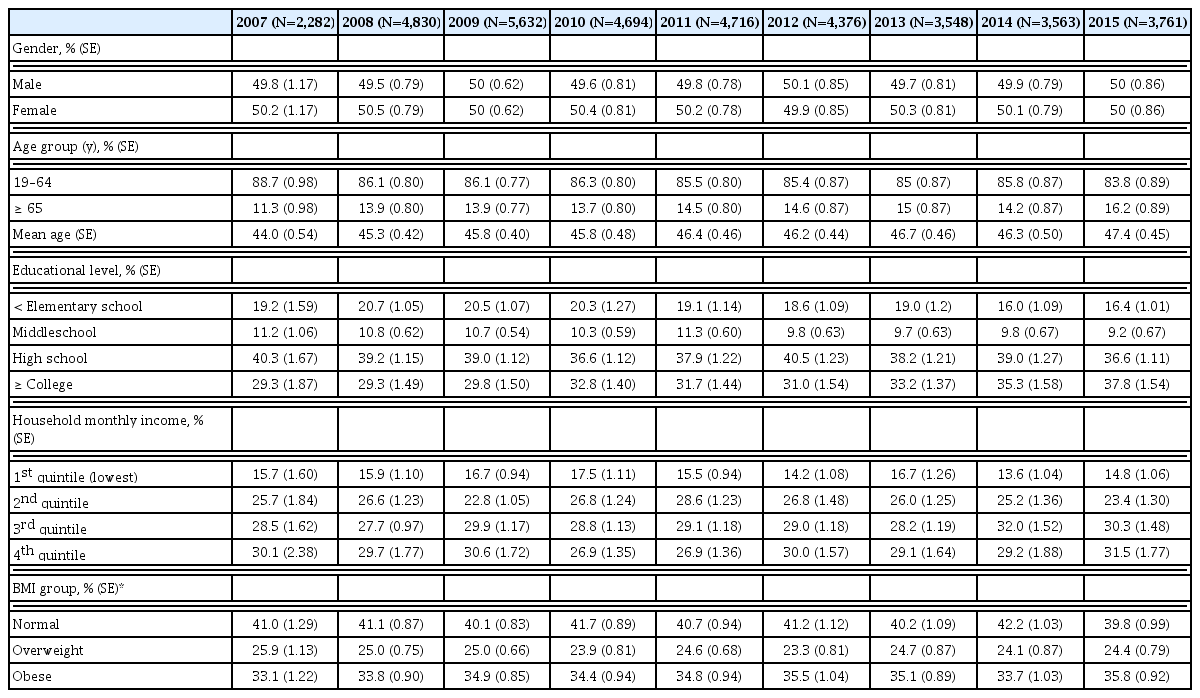
General characteristics of the participants 19 years of age or older, KNHANES 2007–2015.
Table 2 shows trends in the prevalence of CVD risk factors by weight status group. From 2007 to 2015, there were increases in the prevalence of hypertension from 20.3% to 27.5%, diabetes from 8.1% to 9.7%, hypercholesterolemia from 9.0% to 20.4%, whilst low-HDL cholesterol, current smoking, and high-risk drinking were significantly decreased from 2007 to 2015.

In the BMI group analysis, the prevalence of hypertension, diabetes, and hypercholesterolemia were significantly increased in the normal weight group, whilst in the low-HDL cholesterol and currently smoking rate, was significantly decreased (−0.09%p, −0.04%p, respectively). Amongst the overweight adults, the prevalence of each CVD risk factor (except for physical activity), was higher than among normal weight adults. In this group, from 2007 to 2015, there was a significant change showing a decrease in the prevalence of low-HDL cholesterol, currently smoking and high-risk drinking (−0.07%p, −0.03%p, −0.04%p, respectively), whilst hypercholesterolemia and physical activity was significantly increased (0.09%p, 0.02%p, respectively). Amongst the obese adults (except for high-risk drinking), physical activity had an even higher prevalence of CVD risk factor. In this group, there were significant increases in risk factors between 2007 and 2015 for hypercholesterolemia (0.08%p, 95% CI 0.06, 0.10), low-HDL cholesterol. The smoking rate was significantly decreased [−0.05%p, −0.02%p, respectively (Table 2)].
Figure 1 presents the proportion of the number of risk factors for CVD according to BMI status. As the population is categorized according to BMI category, it is evident that in the overweight and obese categories, the number of CVD risk factors becomes more prevalent and delineated compared with the normal population.
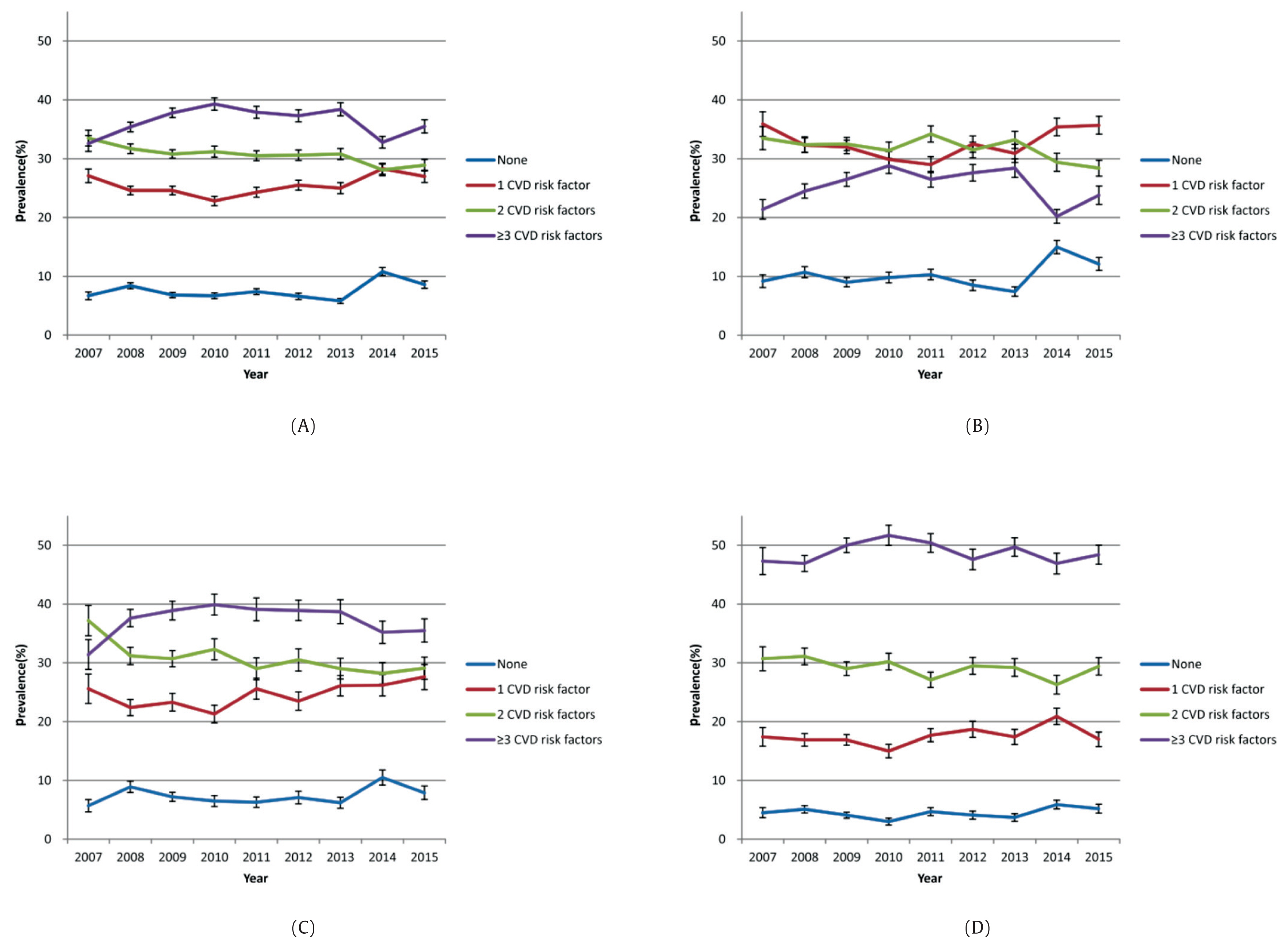
Prevalence of number of risk factors for CVD* by BMI group†. (A) Total population, (B) Normal weight, (C) Overweight, (D) Obese.
*CVD risk factors included: hypertension (systolic BP ≥ 140 mmHg, diastolic BP ≥ 90 mmHg, or use of antihypertensive medications); diabetes (fasting plasma glucose ≥ 126 mg/dL or diagnosed by a doctor); dyslipidemia [at least 1 of the following: hypercholesterolemia (fasting total cholesterol ≥ 240 mg/dL or taking cholesterol medication), hypertriglyceridemia (fasting triglyceride > 200 mg/Dl)], low HDL-cholesterol (fasting < 40 mg/dL), or diagnosed by a physician); self-reported current smoking [more than 5 packs (100 cigarettes) in their lifetime and currently smoking cigarettes]; monthly drinking (drinking more than once a month for the previous year); high-risk drinking [drinking more than twice a week a mean 7 glasses (5 glasses for women) per session]; physical activity [exercise a time equivalent to each activity by mixing physical strength activities (high intensity, 1 minute; medium intensity, 2 minutes) of medium and high intensity for more than 2 hours and 30 minutes of medium-intensity physical activity or 1 hour and 15 minutes of high-intensity physical activity per week].
†BMI group (kg/m2): normal weight, 18.5 to < 23; overweight, 23 to < 25; obese, ≥ 25.
CVD = cardiovascular disease; BMI = body mass index; CI = confidence interval; BP = blood pressure; HDL = high-density lipoprotein.
The number of individuals with 1 risk factor for CVD increased significantly, whereas the number of people with 2 risk factors for CVD decreased significantly (Figure 1).
Table 3 presents the odd ratios of risk factors for CVD by BMI status. Unadjusted, the prevalence of hypertension was 1.9 times higher in the overweight group and 3.3 times higher in the obese group than in the normal weight group, and the prevalence of diabetes was also significantly higher in the overweight and obese groups compared to the normal weight group at 1.6 and 2.4 times, respectively. The prevalence of dyslipidemia was 2.2 times higher in the overweight group and 3.8 times higher in the obese group than in the normal weight group. Adjusted for the prevalence of hypertension, it was 1.7 times higher in the overweight group and 3.4 times higher in the obese group than in the normal weight. The prevalence of diabetes was also significantly higher in the overweight (1.3 times) and obese groups (2.4 times) compared to the normal weight group, and the prevalence of dyslipidemia was 2.1 times higher in the overweight group and 3.6 times higher in the obese group than in the normal weight group (Table 3).

Discussion
Using data from the KNHANES 2007 to 2015, we found significant increases in the prevalence of hypertension, diabetes, hypercholesterolemia and significant decreases in the prevalence of low-HDL cholesterol, and smoking in normal weight adults. In overweight/obese adults, the prevalence of hypercholesterolemia increased, whereas the prevalence of low-HDL cholesterol and smoking significantly decreased.
In recent times, South Korea has experienced lifestyle transitions such as eating a Westernized diet, and decreasing the amount of daily physical activity. It was found that Korean adult food intake has ever-increasing amounts of energy, fat and salt. Sodium daily intake as recommended by the WHO should be < 2,000 mg for adults [13]. A more Westernized diet is leading to an increased risk of high BP and diabetes as most people enjoy food containing more sodium and fat but do less exercise than before. Likewise, higher cholesterol levels due to this diet choice will tend to lead to hypercholesterolemia. Such consequences will be more predominant as obesity rises and the population ages [14]. Moreover, the “health life practicing status” from 2009 to 2013 [15], shows that obese adults do less “health life practice” for weight control generally, even though they have higher rate of chronic disease than those with a healthy, normal weight. This is consistent with the results in this study where the tendency for physical activity by obese people over the years was significantly reduced. This emphasizes the need for effective interventions to bring about lifestyle changes.
In 2007–2015, the prevalence of obesity in Korean adults increased. Furthermore in 2015, > 42% of these obese adults had hypertension, 13% had diabetes, and 64% had dyslipidemia. The increased prevalence of obesity leads to an increase in various obesity-associated diseases and an increased socioeconomic burden for the country.
In the United States, a reported 6%–9% of the national health expenditure was due to obesity versus 2%–3.5% in other countries [16–19]. In Korea in 2007, the prevalence of obesity was low and the related medical expenditures were lower than in Western developed countries. However, this study found that the prevalence of obesity in Korea was 2.7% higher in 2015 than in 2007. According to a study by Kang et al., the total socioeconomic cost of overweight people and obesity in Korea was 1.6 billion USD, which accounts for 3.7% of Korea’s total national health expenditure [20]. Obesity in Korea is continually increasing, and therefore medical expenditure due to obesity is expected to increase. Thus, the burden of disease caused by obesity is not limited to other countries, as it is a serious problem for Korea.
The results of this study showed that the overweight and obese groups had the highest number of people with 3 or more CVD risk factors. The study by Saydah et al [21] also showed that the prevalence of obesity in adults with 3 or more CVD risk factors was significantly increased . The prevalence of CVD risk factors was reported to increase in overweight or obese adults compared to normal-weight adults [22,23]. Large prospective cohort studies have shown associations of adiposity at baseline and incidence of hypertension and dyslipidemia [24–29]. Associations between weight loss and lowering BPs and improving lipid values have been shown in clinical trials [30–33]. Must et al [34] found in the US National Health and Nutrition Survey that obesity-associated diseases in adults such as Type 2 diabetes, gallbladder disease, hypertension, and coronary artery disease increased with increasing BMI. CVD is a multifactorial disease that is not caused by a single risk factor but is caused by the interaction of many risk factors, such as socioeconomic level. Therefore, management to prevent CVD should consider the combination of all major risk factors.
The current smoking rate in Korea had a steadily decreasing trend that dropped sharply from 2007 to 2015. This may reflect new pricing policies that were introduced after 2014 where tobacco tax was placed on cigarettes, with an 80% increase in cigarette prices by 2015, and non-smoking policies were introduced in restaurants from 2014 [35]. The current smoking rate showed a similar trend for each BMI group in this study. However, current smoking rates were still higher in the obese group compared with the normal weight and overweight groups. Previous studies have found that smoking was associated with weight loss and smoking cessation was associated with weight gain [36,37]. In contrast, a study by the International Agency for Research on Cancer (IARC) suggested that obese people were at a higher risk of smoking [38]. In addition, according to the risk factors of CVD, compared to the normal and overweight groups, the obesity group showed more CVD risk factors by smoking. These results have implications for public health interventions that aim to reduce the prevalence of these CVD risk factors.
Physical activity was the 1 risk factor where the prevalence has not changed significantly in any BMI group from 2007 to 2015. However, epidemiological studies suggest that regular aerobic physical activity may be beneficial for both prevention and treatment of hypertension, and to lower CVD risk and mortality. The physical activity should be at least 30 minutes of moderate-intensity dynamic aerobic exercise (walking, jogging, cycling or swimming) of 5–7 days per week [39–41].
Previous studies have also reported that obese adults are at a higher risk for CVD than normal weight adults [42–44]. These results are consistent with the results of odds ratios according to the BMI group as shown in this study. The risk of diabetes, hypertension, and dyslipidemia was 1.4–2.1 times higher in overweight than in normal weight adults, and 2.4–3.6 times higher in obesity. Also, in previous studies, obesity had more than twice the population attributable risk compared with being overweight [20]. This implies that a positive relationship exists between BMI and CVD incidence in overweight and obese adults. Therefore, to prevent CVD caused by obesity, efforts should be made to reduce the proportion of overweight and obese adults in the population. However, in the short term, measures should be taken to prevent overweight and obese adults gaining more weight.
In 2011–2015, amongst the normal weight adults, the number of people who had 1 risk factor for CVD increased significantly. Recently, increases in CVD mortality in South Korea have been documented. It was found that lifestyle choices are insufficiently managed, with a rapid rise in high-risk drinking, diabetes and hypercholesterolemia observed before CVD onset [45]. Many of these increases are likely to aggravate cardiovascular risk factors in the South Korean population. Along with an increase in the obese population, the normal weight population also showed increased risk of high BP and diabetes, which indicates preventive measures against the risk needs to be taken.
CVD is 1 of the major causes of death in Korea and has a large disease burden. CVD and cerebrovascular disease have been the 2nd and 3rd highest causes of death in Korea over the past decade [46]. Moreover, the socioeconomic cost of CVD has been estimated at a cost of 12.2 billion USD [47]. This can only be prevented through sustainable management, and the state must intervene and manage it by considering individual health and socioeconomic benefits. CVD risk factors include obesity, reduced physical activity, smoking, and unhealthy meals, and changing these risk factors can delay or prevent CVD [48–50]. Therefore, preventing or carefully managing obesity can reduce the cost of related diseases as well as the health burden caused by CVD.
The main strength of this study was the use of a nationally representative survey that measured weight and height and assessed CVD risk factors in a standardized method. However, this study has some limitations to consider. Firstly it could not be determined whether the change in prevalence of CVD risk factors was an actual increase or was due to a change in the age structure, because age-standardization for prevalence was not considered. Secondly, this is only representative of the noninstitutionalized civilian population that can attend in-person exations. Finally, we did not estimate at the subnational level to assess implications for particular population subgroups, such as those distinguished between urban and rural regions of South Korea.
In conclusion, the prevalence of obesity in Korean adults is increasing, and it is necessary to implement interventions when considering the influence of obesity on the health of the nation. There is also a strong causal relationship between being overweight and obesity and the occurrence of CVD. Obesity management is very important for reducing the cost of medical treatments due to CVD and reducing the disease and economic burden. Obesity in particular is an important risk factor for hypertension, diabetes, and dyslipidemia, which are likely to progress to CVD. Therefore, it is necessary to focus more resources nationally on managing CVD.
Acknowledgements
This work was supported by the Soonchunhyang University Research Fund.
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.