Factors Influencing Self-Rated Oral Health in Elderly People Residing in the Community: Results from the Korea Community Health Survey, 2016
Article information
Abstract
Objectives
The aim of this study was to examine the factors influencing perceived oral health in elderly individuals residing in the community.
Methods
This study used raw data from the Korea community health survey, 2016. Of the 64,223 participants that were elderly (aged ≥ 65 years), 61,280 (95.4%) were included for analysis. Self-rated oral health was the dependent variable and 6 independent variables including age, gender, type of area of residence (metropolitan or provincial), educational level, income, and living status with spouse were assessed. Oral function was studied based on mastication, pronunciation, and use of dentures, and oral health behavior included brushing teeth after breakfast, after lunch, after dinner, and before sleep). The EQ-5D questionnaire measured health-related quality of life (mobility, self-care, usual activities, pain/discomfort and anxiety/depression).
Results
Among the general characteristics, age, gender, educational level, income, and living status with spouse were the factors that affected self-rated oral health. Mastication, pronunciation, use of dentures, and brushing after lunch, dinner, and before sleep were the factors that influenced self-rated oral function. All domains of the EQ-5D (pain/discomfort, mobility, self-care, usual activities, and anxiety/depression) were factors that affected self-rated oral health.
Conclusion
The results of the current investigation suggest that the development of management and education strategies for oral health promotion in the elderly, should focus on improving oral function and oral health behavior, taking into account the socio-economic and demographic characteristics that have been shown to be associated with poor self-rated oral function.
Introduction
The elderly population (≥ 65 years) accounted for 14.8% of the total population in Korea in 2019. Korea is expected to become a “super-aged society” with an elderly population predicted to exceed 20% of the population by 2026 [1]. In this context, the national healthcare burden is expected to significantly increase for the elderly in the future. Elderly individuals are susceptible to disease due to the number of comorbidities that they live with, physical disability, metabolic imbalance, and decreased immunity [2,3].
In the elderly, oral diseases are associated with chronic conditions such as hypertension, hyperlipemia and diabetes. However, the elderly tends to regard oral health problems as a process of aging, maybe because initially these health problems do not directly affect their quality of life [4]. Oral health care is also important for the management of swallowing disorders, which are common in the elderly. In the case of elderly inpatients, mortality increases due to pneumonia in the absence of adequate oral care [5,6]. In addition, secondary symptoms due to oral disease may have a negative effect on chewing, affecting pronunciation thereby affecting interpersonal relationships leading to depression, and thus reduced quality of life [7,8].
The Charter of the World Health Organization defined health as a state of physical, mental, and social well-being, and so it is not simply being disease-free or frail [9]. Since an individual’s current health status can influence their future health, it is necessary to practice health care management starting from a young age.
Lawton et al [10] reported that the quality of life was a highly subjective element. It has been reported that quality of life was strongly related to self-rated health, and depression [11]. In other words, these results are not only an objective measure of health index, but also a result of self-health assessment including self-rated health status.
In the past, self-rated health has been considered as a secondary variable because it is used as an index of psychological well-being, from a medical perspective [12]. However, self-rated health has been used as an objective health index such as mortality, and as a known predictor of objective health [13,14].
Previous oral health studies have focused on self-rated oral health as a secondary variable, including oral health behavior [15], and oral health-related quality of life (HRQOL) [16–18]. Thus, the variables that affect self-rated oral health are unknown [19]. Therefore, the aim of this study was to examine the factors influencing self-rated oral health in elderly people living in the community.
Materials and Methods
1. Participants
This study analyzed the raw data of the 2016 Korea community health survey, which was designed to establish and evaluate regional healthcare plans, and to compare regional health statistics by standardizing the survey execution system. The Korea community health survey is a Korean-approved statistical survey (no: 117,075). The methodology of the Korea community health survey was based on interviews. The data for 228,452 study participants were extracted, which included 64,223 aged ≥ 65 years. Among these 64,223 patients, 61,280 (95.4%) were analyzed in this study after missing values and those without responses were excluded.
2. Variables
In this study, the dependent variable was self-rated oral health, and the independent variables were age, gender, region, educational level, monthly income, and living status. Oral function consisted of mastication, pronunciation, and use of dentures. The oral health behaviors included brushing teeth after breakfast, lunch, and dinner, and before sleeping. The questionnaire used to measure HRQOL was EuroQol-5 Dimension (EQ-5D) which is divided into 5 sub-domains (mobility, self-care, usual activities, pain/discomfort and anxiety/depression). Each dimension has 5 levels of response: no problems, slight problems, moderate problems, severe problems and extreme problems. A total of 18 independent variables were selected. The question about self-rated oral health was as follows: “How is your oral health including the condition of your teeth and gingiva, based on your own perception?” For statistical analysis, coding was set to 1 = good, and 0 = bad. The question regarding mastication to assess the oral function was as follows: “Do you experience chewing difficulty or inconvenience due to oral problems related to teeth, dentures, or gingiva?” The question related to pronunciation was as follows: “Do you experience difficulty or inconvenience with clear pronunciation due to oral issues involving teeth, dentures, and gingiva?” For both questions, the response was scored 1 for discomfort and 0 for comfort. The question related to use of dentures was as follows: “Do you currently use dentures?” The response was scored 1 for use of denture, and 0 for no use. Oral health behavior was evaluated as “4 times during the day, after breakfast, after lunch, after dinner, and before sleep.” The answer was either a “yes” or a “no.” The HRQOL questionnaire used in the study was EQ-5D. A study of the EQ-5D index has been reported for each country for the assessment of HRQOL in various countries [20]. EQ-5D is divided into 5 areas: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. In the current analysis, “normal” was coded as 0 and “limitation” as 1 in each sub-domain.
3. Statistical analysis
The data analysis was performed with SPSS 22 (IBM Corp., Armonk, NY, USA). The participants’ general characteristics, oral function, oral health behaviors, and HRQOL were confirmed via frequency analysis. To determine the factors affecting self-rated oral health of the elderly, we performed adjusted random-effects logistic regression analysis (multivariate analysis). Namely, to discern the odds ratio between good or bad self-rated oral health, the above logistic regression model was applied. Self-rated oral health was based on a dependent variable, 6 general characteristics (age, gender, region, education level, income, living status), 3 measures of oral functions (mastication, pronunciation, use of dentures), 4 parameters of oral health behavior (after breakfast, after lunch, after dinner, before sleeping), and 5 health-related measures of quality of life (mobility, self-care, usual activities, pain/discomfort, anxiety/depression). Statistical significance was set at p < 0.05.
Results
Table 1 shows the general characteristics, oral function, oral health behavior, and HRQOL in the elderly. The participants’ ages ranged from 65 to ≥ 80 years, with the highest proportion of participants being 65 to 69 years (28.0%). Females constituted 58.7% of the total study group. There were 78.7% of study participants who resided in provincial areas. The highest education attainment level in the study group was completing elementary school (43.2%). The monthly income of 500,000–1,000,000 won accounted for the greatest number of participants in this study. Cohabitation with a spouse accounted for 63.2% of the group. In the assessment of oral function, mastication discomfort accounted for 47.0% of participants, there were 20.1% of the study group that had pronunciation difficulties, and there were 48.6% who used dentures. In terms of oral health behavior, the proportion of participants who brushed their teeth after breakfast constituted 89.2%, those who brushed after lunch were 34.3%, after dinner 67%, and before sleeping was 35%. In HRQOL, mobility was limited in 46.3% of participants, self-care was limited in 18.1%, usual activities were limited in 37.1%, pain/discomfort was experienced by 54.4% and anxiety/depression by 20.8% of participants.
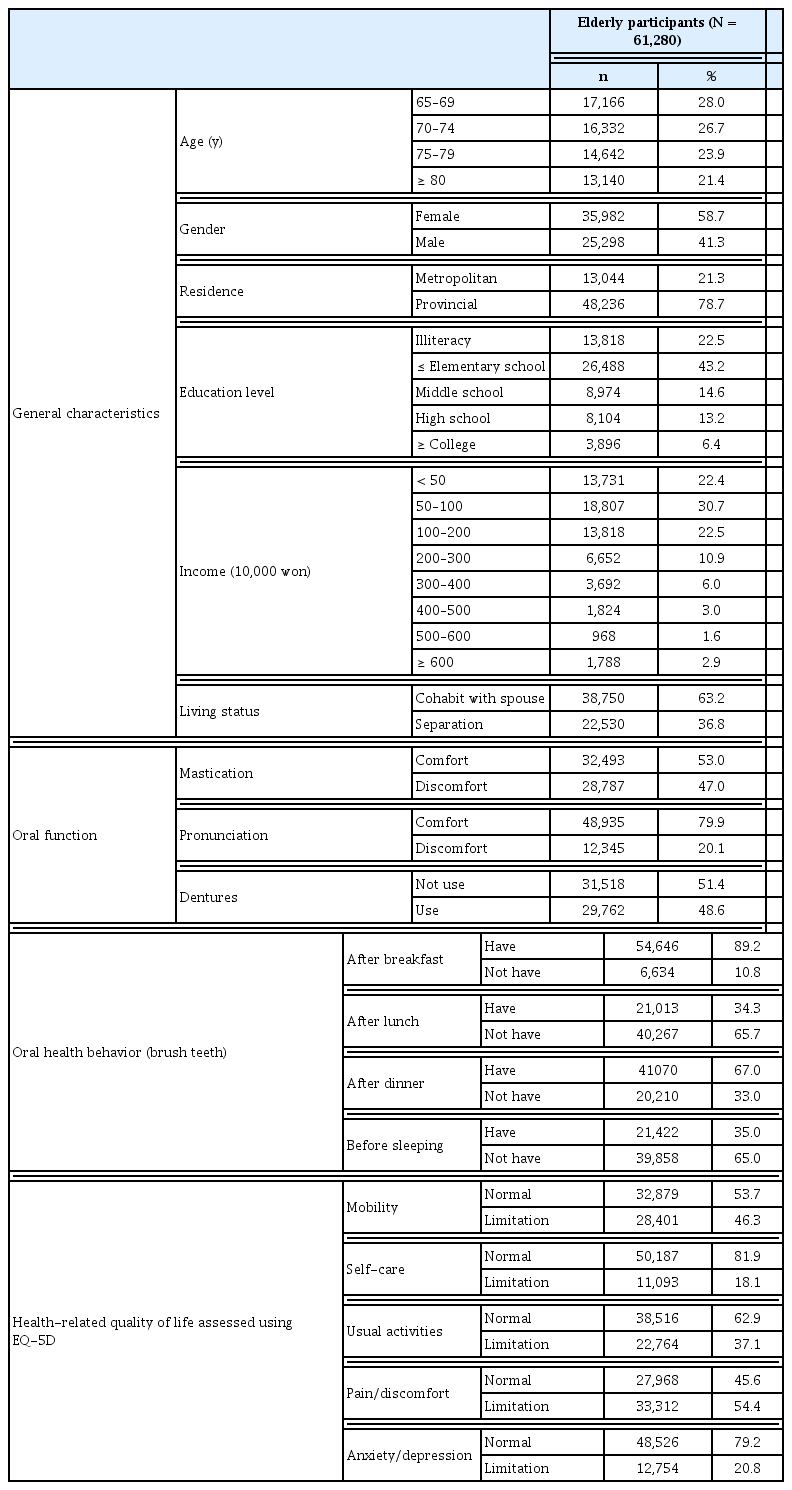
General and socio-economic characteristics, oral function, oral health behavior, and health-related quality of life in the elderly who reside in the community.
Table 2 shows the factors affecting self-rated oral health in the elderly living in the community. The logistic regression analysis revealed that age, gender, education level, income, living status, oral function, oral health behavior and HRQOL were all associated with self-rated oral health. Only the residential area of a participant was not associated with self-rated oral health. In the age group of 65–69 years, 70–74 years (OR = 0.877, 95% CI 0.831–0.926, p < 0.001), 75–79 years (OR = 0.787, 95% CI 0.742–0.835, p < 0.001), and 80 years (OR = 0.725, 95% CI 0.678–0.776, p < 0.001), the increased levels of self-rated oral health were associated with better outcomes. Males were more likely to report a lower level of self-rated oral health than females (OR = 1.233, 95% CI 1.173–1.295, p < 0.001). There was no significant difference according to the residential area (OR = 0.976, 95% CI 0.928–1.027, p = 0.353). Educational level was more likely to be associated with self-rated oral health, which increased in the following order: illiteracy, elementary school (OR = 0.919, 95% CI 0.868–0.974, p = 0.004), middle school (OR = 0.918, 95% CI 0.851–0.990, p = 0.026), high school (OR = 0.831, 95% CI 0.768–0.901, p < 0.001), college or higher level (OR = 0.748, 95% CI 0.677–0.827, p < 0.001). Elderly individuals with a monthly income of more than 6,000,000 won, were more likely to have better self-rated oral health than elderly participants with a monthly income of less than 500,000 won (OR = 0.865, 95% CI 0.763–0.980, p = 0.023). Living with a spouse was rated as healthy compared with those who were separated (OR = 1.073, 95% CI 1.021–1.128, p = 0.006). Lower oral function self-rated oral health scores were observed in participants who showed discomfort during mastication (OR = 8.501, 95% CI 8.111–8.911, p < 0.001) and pronunciation (OR = 2.117, 95% CI 1.966–2.280, p < 0.001), and those using dentures (OR = 3.527, 95% CI 3.377–3.683, p < 0.001). In oral health behavior, brushing after lunch (OR = 1.071, 95% CI 1.023–1.122, p = 0.004), after dinner (OR = 1.052, 95% CI 1.002–1.105, p = 0.043), and before sleep (OR = 1.055, 95% CI 1.008–1.104, p = 021) had a positive impact on self-rated oral health. HRQOL including pain/discomfort (OR = 1.197, 95% CI 1.137–1.260, p < 0.001), mobility (OR = 1.166, 95% CI 1.097–1.240, p < 0.001), self-care (OR = 1.096, 95% CI 1.022–1.176, p < 0.001), usual activities (OR = 1.099, 95% CI 1.028–1.174, p = 0.005), and anxiety/depression (OR = 1.162, 95% CI 1.098–1.231, p < 0.001) affected self-rated oral health.

Factors influencing self-rated oral health in elderly participants residing in the community.
Discussion
Factors that influence self-rated oral health have been identified in the elderly that live in the community. The independent variables that affected oral health were socio-economic and general characteristics, oral function, oral health behavior, and HRQOL.
General and socio-economic characteristics such as age, gender, educational level, monthly income, and living status were factors affecting self-rated oral health. In the study of Oh and Kim [19], the variables that differed according to the self-rated health of the elderly were occupation, and medical care, and the influencing factors were 1.65 times stronger compared with those without an occupation. Yang and Seo [15] reported a significant difference in oral health behavior in the elderly according to income and educational level. This current study was inconsistent with the results of Oh and Kim [19], but was similar to Yang and Seo [15]. Self-rated oral health was more likely to be better in the oldest individuals in the study, educational level, and in males than in females, with a monthly income of more than 6,000,000 won compared with elderly people with a monthly income of 500,000 won. The elderly who were separated reported a worse self-rated oral health than those who cohabited with their spouse.
Interestingly, the lower the age of the elderly participants, the worse the self-rated oral health. Objective health assessments often result in a decreased overall health due to aging. However, considering that self-rated health is based on several psychological factors, the impact of using dentures earlier in old age has a negative effect on self-rated oral health [10].
Factors such as mastication, pronunciation, use of dentures, brushing teeth after breakfast, lunch, dinner, and before sleep affected self-rated oral health. These results suggest that our findings were similar to the results of Lee and Park [21] in that the higher the frequency of brushing, the higher the score for happiness. In this study, the odds ratios of mastication, pronunciation, and use of dentures were high. In the study of Koshino et al [22], mastication and use of dentures affected the quality of life of residents in the community. The current study yielded similar results.
All domains of HRQOL influenced self-rated oral health. The odds ratios showed similar values for pain/discomfort (1.19), mobility (1.166), anxiety/depression (1.162), self-care (1.096), and usual activities (1.099). These findings suggest that self-rated health is a psychological factor [13,14].
This study used the 2016 Korea community health survey to identify the factors that influenced self-rated oral health among 61,280 elderly participants. However, since this study was based on a cross-sectional design, the odds ratios cannot show a causal relationship, and therefore, the comparison or relevance of the study requires interpretation.
The results of this study suggest that the self-rated oral health of the elderly population is based not only on psychological factors, but also on demographic and sociological aspects, oral function, oral health behavior, and physical function. Health education and health promotion programs should be developed specifically for elderly participants living in the community.
Acknowledgments
This research was supported by Kyungdong University Research Fund, 2020.
Notes
Conflicts of Interest
There was no conflict of interest to declare.