Global prevalence of enterobiasis in young children over the past 20 years: a systematic review and meta-analysis
Article information

Abstract
Parasitic infections are the most common diseases worldwide, and enterobiasis is a common parasitic infection in children. Various studies have reported on the prevalence of Enterobius vermicularis in different regions of the world. However, no study has gathered and analyzed this data systematically. Our systematic review and meta-analysis investigated the overall prevalence of E. vermicularis among children globally. Data were extracted from 4 available databases for studies published from January 2002 to April 2022. The quality of the included studies was scored based on the standard Strengthening the Reporting of Observational Studies in Epidemiology. A random-effect model was chosen to calculate the pooled prevalence and corresponding 95% confidence interval (CI) according to the degree of heterogeneity in the included studies. Thus, 40 publications (42 data sets) that included 3,279 children with enterobiasis met all criteria and were included in the analysis. The meta-analysis showed that heterogeneity among the included studies was high (Q=4,399.35, I2=99.96%; df=41; p<0.001). The pooled global prevalence of enterobiasis among the studied children was 12.9% (95% CI, 8.2%–17.7%). Our systematic review and meta-analysis estimated that, for the past 20 years, 12.9% of children around the world have been infected with E. vermicularis.

Introduction
Enterobiasis or oxyuriasis, a nematode infection caused by Enterobius vermicularis (E. vermicularis, pinworm, oxyure) is common among children and their family members [1]. E. vermicularis is a cosmopolitan parasite and one of the most common parasitic infections in many countries [2]. The World Health Organization reported that the prevalence of enterobiasis in children is between 4% and 28% [3]. It has been estimated that approximately 200 million people are infected worldwide, and over 30% of cases are children aged 5 to 10 years [4]. The prevalence of oxyuriasis among children has been reported as 2.5% to 45% in Latin America [5,6], 18% in Norway [7], 18.5% in the Republic of Korea [8], 17.2% in Iran [9], and 2.9% in north-central Ethiopia [10].
Some patients with enterobiasis are asymptomatic, while others, especially children, may show symptoms such as perianal pruritus, restlessness, loss of appetite, malnutrition, anemia, insomnia, and irritability. Ectopic enterobiasis can penetrate the kidneys and fallopian tubes, leading to severe health disorders and even death [11,12].
Although there are multiple ways to transmit enterobiasis, including the fecal-oral route, inhalation, auto-infection, and retrograde infection [13], the main route of transmission for E. vermicularis is direct contact between infected and uninfected individuals. Therefore, children in crowded environments such as kindergartens, schools, orphanages, and mental institutions are most susceptible to this infection [14]. The prevalence of this infection is mainly related to public health and personal hygiene [9]. Therefore, surveying enterobiasis infections in children can help us assess personal, familial, and social health status. The identification and prevention of pinworm transmission among children can promote infection control and benefit the health of children and the community [9].
There are many publications regarding the prevalence of E. vermicularis infection among children. However, there are no comprehensive studies describing the status of enterobiasis infection in children globally. In the present systematic review and meta-analysis, we investigated the global pooled prevalence of E. vermicularis among young children.
Materials and Methods
Design
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines [15]. It also followed recommendations from the Cochrane Collaboration Handbook of Systematic Reviews [15] for the systematic, transparent, and reproducible investigation of scientific evidence.
Search Strategy
Two independent investigators (S.D., E.K.L.) searched 4 international databases (PubMed, Scopus, Science Direct, and ProQuest) for published studies that investigated the prevalence of E. vermicularis in children. English language publications between 2002 and 2022, with mesh terms (“Enterobius vermicularis” OR E. vermicularis OR Oxyuris OR pinworm OR roundworm OR seatworm) AND (Prevalence OR Rate) AND (Children OR Preschool OR Kindergarten), were collected. In addition, the reference lists of the identified articles were manually searched. We included studies conducted in the last 2 decades (01 January 2002 to 24 April 2022), published in English, and relevant to the aim of the study.
Eligibility Criteria
The eligibility criteria for the study were determined using the population, intervention, comparison, outcome, and study classification design (Table 1). The inclusion criteria were (1) cross-sectional studies that estimated the positive rate of E. vermicularis in children, (2) studies published online between January 2002 and April 2022, (3) original research papers, (4) studies published in English, (5) articles with full text, (6) studies that provided the total sample size and positive samples, and (7) studies that had a clear test method. Articles that did not meet these criteria were excluded. In addition, we contacted the corresponding authors to obtain more information if the data was incomplete. Reviews, case reports, letters to editors, and commentaries were not included in the study, but were used to enhance the search sensitivity to include any missed studies.

Eligibility criteria for a systematic review and meta-analysis of the global prevalence of enterobiasis in children
Study Selection
The 2-step study selection process included a title/abstract reading phase and a full-text reading phase. All search records were imported to EndNote software ver. X7.0.1 (Clarivate). All duplicates and irrelevant papers were excluded after the screening of titles/abstracts by 2 independent reviewers (S.D., E.K.L.). Any discrepancies were resolved by a third reviewer (S.A.H.). In the second phase, the full-text articles were downloaded and meticulously evaluated and discussed with 2 other reviewers and, if necessary, a third reviewer was consulted. Study selection was performed in accordance with the PRISMA flowchart.
Data Extraction
The data in each study were extracted independently by 2 reviewers (S.D., E.K.), using Microsoft Excel ver. 16.39 (Microsoft Corp.). Discrepancies were resolved by a third reviewer (A.M.). We included information on title, first author, year of publication, continent and country, sample size, number of positive samples, subject age and gender, and diagnostic method.
Quality Assessment
The quality of the included studies was scored using the standard Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). A STROBE score of 25.6 to 34 indicated a high-quality study, and studies with scores of 16.6 to 25.5 and ≤16.5 were considered moderate and low quality, respectively. The articles included in our meta-analysis were deemed to have acceptable quality.
Data Analysis
We used Stata ver. 15.0 (Stata Corp.) for all statistical analyses. The heterogeneity among studies was calculated using both the Cochran Q test and the I2 statistic, with a cutoff at 50% to define a statistically significant degree of heterogeneity. The random-effect model was chosen according to the degree of heterogeneity in the included studies to calculate the pooled prevalence and corresponding 95% confidence interval (CI). To investigate the effect of different variables on heterogeneity, we did a subgroup analysis stratifying participants based on continent, age group, and publication decade. In addition, a funnel plot and an Egger test were used to assess the publication bias of selected studies.
Ethics Approval
This study received approval from the Qazvin University of Medical Sciences Ethical Committee Iran under the contract no. IR.QUMS.REC.1401.291.
Results
A flow chart of the study search and selection process for inclusion is shown in Figure 1. In our study, a total of 3,508 publications were searched. After removing duplicate articles, the titles and abstracts of the remaining 3,097 publications were screened. Finally, a total of 117 articles were selected for full paper review, of which 40 publications (42 data sets) fulfilled all criteria and were suitable for inclusion in the analysis. Among 60,176 children surveyed in these 40 publications, 3,279 children had enterobiasis.
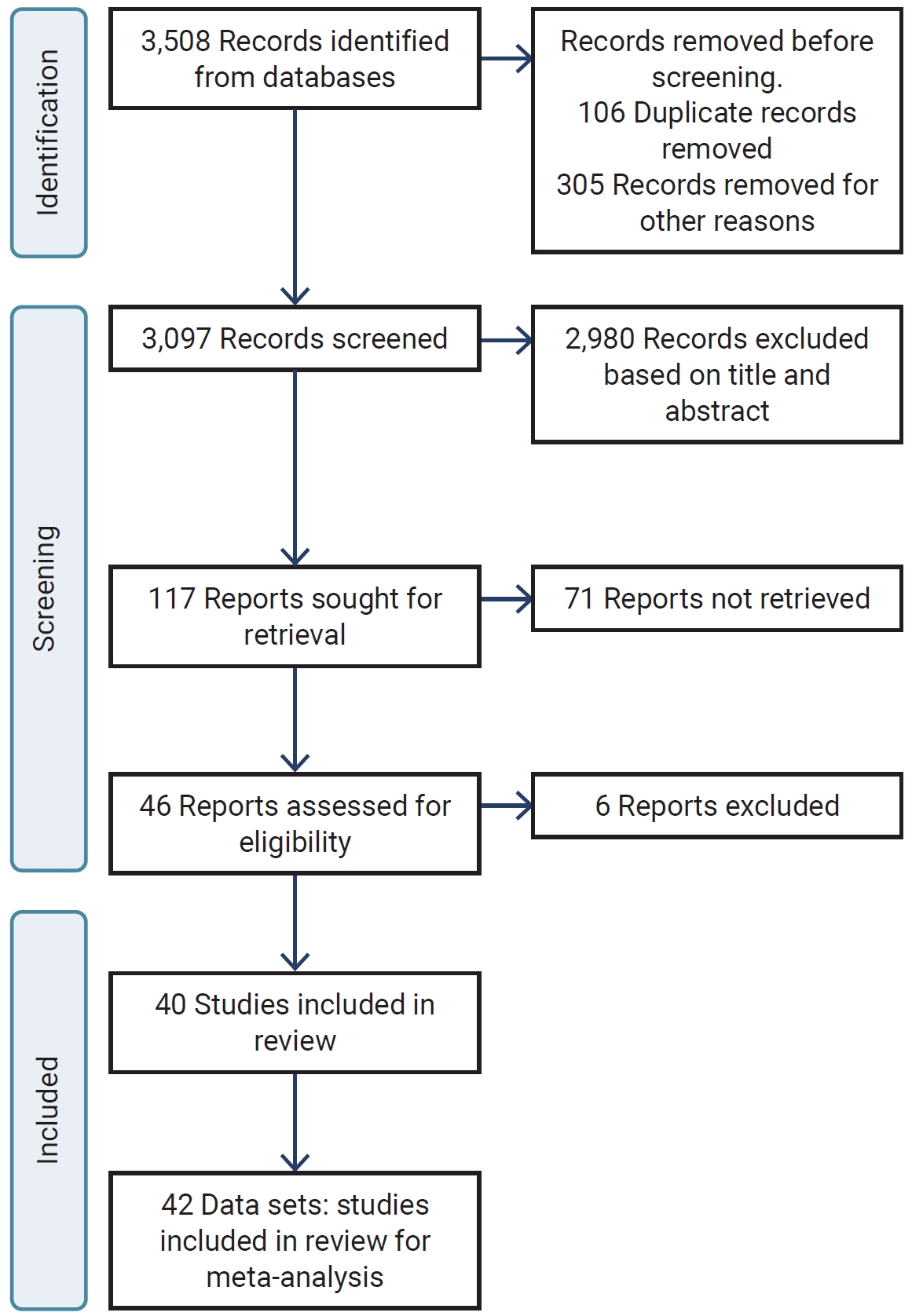
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flowchart of literature selection to analyze the worldwide prevalence of enterobiasis in children.
Most of the included publications originated in Asia (32 out of 42, 76.2%). Five were from South America (11.9%), 2 from Africa (4.8%), 2 from Europe (4.8%), and 1 from North America (2.4%). Among the countries, Iran and The Republic of Korea had the most studies with 8 (19.0%) and 7 (16.7%) studies, respectively. The main characteristics of the included studies are summarized in Table 2 [8,11,16–53].

Characteristics of studies investigating the prevalence of enterobiasis in children
Among the included studies, 14 investigated oxyuriasis in kindergarten children, 14 investigated preschool populations, and the remaining 7 studies investigated oxyuriasis in general child populations. Four were studies of children referred to medical clinics. Two studies were based on primary school children, and 1 studied child in a random population.
The diagnostic methods used to detect E. vermicularis infection across studies were: cellophane tape swab (33 articles), cellophane anal swab (1 article), formalin-ethyl acetate concentration (3 articles), cellophane tape and formalin-ether concentration (1 article), microscopic formalin-ether concentration (1 article), the Lutz method (1 article), the Kato-Katz-direct smears (1 article), and the Kato-Katz method (1 article).
The meta-analysis showed that heterogeneity among the included studies was very high (Q=4,399.35; I2=99.96%; df=41; p<0.001). Since the heterogeneity was significant, a random-effects model was used to estimate the pooled prevalence of enterobiasis among kindergarten and preschool children globally. In addition, the funnel plot and bias coefficient diagram did not show the presence of publication bias (b=–1.25; 95% CI, –0.0002 to 4.69; p=0.21) (Figure 2).
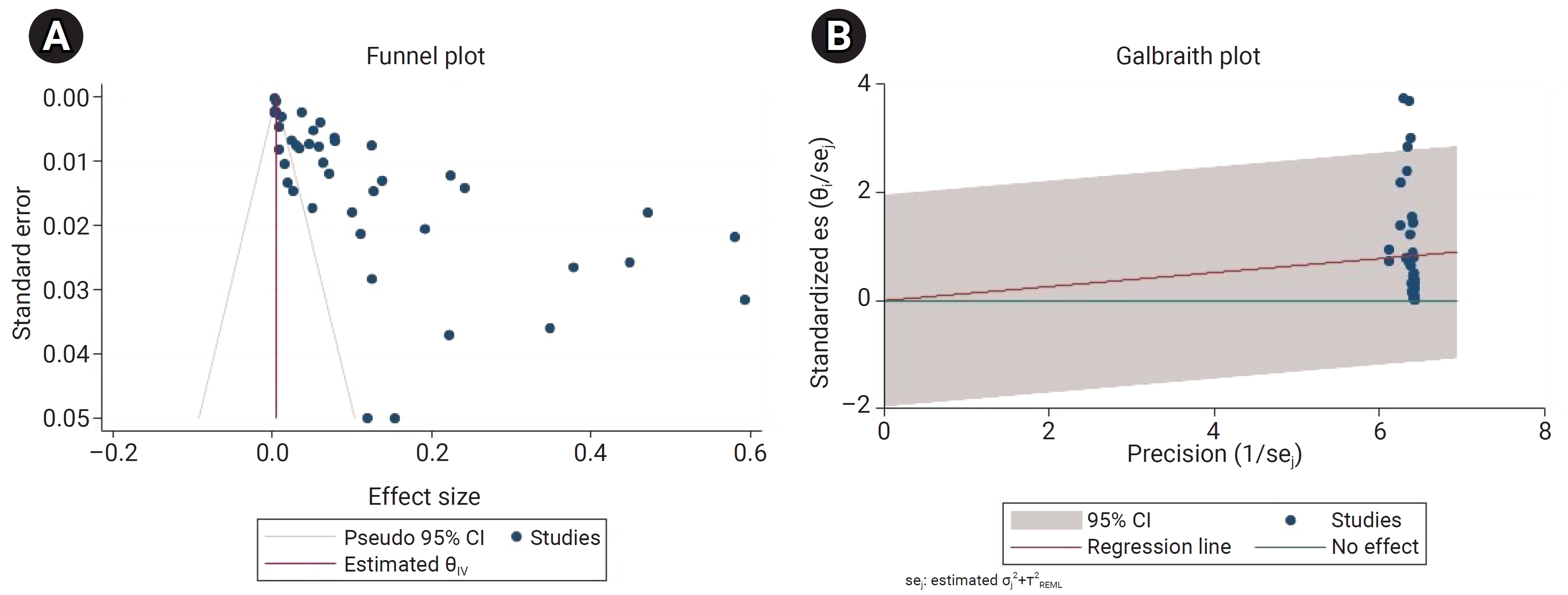
Bias assessment plots for the global prevalence of enterobiasis among the subjects studied. (A) Funnel plot for detecting publication bias. (B) Galbraith plot for detecting publication bias. CI, confidence interval.
Using the random effect method, the pooled global prevalence of enterobiasis among the children studied was 12.9% (95% CI, 8.2%–17.7%). The global pooled and weighted prevalence of enterobiasis among children based on geographic location was as follows (Figure 3): Europe 24.9% (95% CI, 0%–64%), South America 14.3% (95% CI, 0%–36.4%), Asia 13% (95% CI, 8.1%–17.9%), Africa 2% (95% CI, 0%–4.5%), and North America 1.9% (95% CI, 0%–4.6%).

Forest plot of the global prevalence of enterobiasis among the subjects studied using the random effects method.
CI, confidence interval; REML, residual or restricted maximum likelihood.
According to our meta-analysis, the primary school group exhibited the highest pooled prevalence of E. vermicularis infection, with a prevalence rate of 34.7% (95% CI, 10.5%–59%), followed by 20.2% (95% CI, 4.9%–35.5%) in the general child population group, 14.1% (95% CI, 0%–34.7%) in children referred to medical clinics, 11.2% (95% CI, 5.9%–16.5%) in kindergarten children, 8.2% (95% CI, 0.6%–15.8%) in preschool children, and 2.6% (95% CI, 0%–5.5%) in the random population group.
Discussion
To the best of our knowledge, this is the first systematic review and meta-analysis to pool the global prevalence of enterobiasis in children. The current review included studies published between 2002 and 2022 that reported on the epidemiology of E. vermicularis infection in children worldwide. According to our review results, the global pooled estimated of children infected with enterobiasis was 12.9 %.
Several regional studies on the prevalence of Enterobius infection have been conducted [4], showing enterobiasis prevalence among school children as follows: approximately 55% in China, 8.8% in Thailand, 47.2% in Myanmar, 4.4% in the Republic of Korea, and 19.3% in Kyrgyzstan (Asia); 26.3% in Tanzania, 1.7% in Angola, and 11.7% in Nigeria (Africa); 35% in Chile and 19% in Argentina (South America); and 17.4% in Germany.
Pinworm infection is transmitted through direct contact with infected persons or objects. The worm is transmitted through ingestion of eggs, from the anus to the finger, fingernails, or hands when a patient scratches the perianal area where the gravid female worms emerge and deposit eggs [54]. Indirect aerosol transmission has also occurred in humans; the microscopic eggs can be released in the air and inhaled with dust [55]. Socioeconomic status, personal hygiene habits, and the environment are also important factors in the spread or prevention of E. vermicularis infection [56], contributing to its significance as a public health problem.
Our data revealed a higher prevalence of E. vermicularis in younger children who lacked knowledge and understanding of this infection, its risk factors, and prevention. The major risk factors for enterobiasis include the personal hygiene habits of children, such as thumb-sucking and putting toys into their mouths; the overcrowded conditions in schools, kindergartens, and childcare centers; and inadequate sanitation. The risk factors for pinworm infection may vary in different countries [9,54]. According to a study conducted in Yemen, war led to increased pollution in the water and food supplies and worsened sanitary disposal systems and housing. These circumstances, along with a lack of heath awareness by the majority of parents and affected children were the main risk factors for disease [4].
The diagnosis of enterobiasis is based on finding adult worms or eggs using the scotch tape technique or by stool examination, which is less sensitive. The scotch tape technique is the gold standard method for detection of enterobiasis in children because it is practical, easy, and inexpensive [13,57]. The fact that the worm’s eggs are sticky and adhere to the perianal skin [4] is consistent with the lower prevalence rates we found in studies that detected eggs in stool samples rather than using the scotch tape technique.
For effective infection control and health promotion in children, it is important to identify the factors that help identify parasite transmission as well as aid in its prevention [9]. Although Enterobius is susceptible to some anthelminthic drugs including mebendazole and albendazole, these drugs only kill the adult worm and are not effective against eggs and larvae. The main point is that medical treatment is not sufficient to cure and control enterobiasis and does not prevent re-infection [13].
To reduce prevalence rates, effective health promotion includes increasing the awareness of the child and family. Because of the high prevalence of re-infection with enterobiasis, health education and screening programs must be provided for the children, teachers, and parents who gather in crowded places like schools, kindergartens, and daycare centers [9]. One of the most effective control strategies for Enterobius infection is to promote knowledge among families, especially mothers and children, and change their hygiene behaviors [56].
Various studies have confirmed that increasing knowledge and the hygiene practice levels of families is a suitable control strategy. In Egypt, the Republic of Korea, and Cameroon, decreasing prevalence rates have been reported as a result of health education provided to mothers, the distribution of educational brochures to the children and their families, and visual educational cards, respectively [16,56,58]. As a result of control and screening programs, a decreasing trend in the prevalence rate of E. vermicularis infection has been reported in some countries [9]. In the Republic of Korea and Greece, the prevalence rates dropped from 17.1% to 7.9% and 22.1% to 5.2%, respectively. In Turkey, another study reported the infection rate from 1985 to 2000 was 45.9%, while it was 16% from 2000 to 2008, similar to our findings [16,59–61].
Our systematic review and meta-analysis had certain limitations: (1) lack of uniform sample size, (2) differing diagnostic methods with varied sensitivity and specificity, and (3) heterogeneity in our review results due to the heterogeneity of different articles. These factors may have biased the prevalence of E. vermicularis infection in the study population.
Conclusion
Although there were many country-specific studies on the prevalence of enterobiasis in children, there were no comprehensive studies describing the status of enterobiasis infection in children globally. Our systematic review and meta-analysis estimated that 12.9% of children around the world are infected with E. vermicularis. Health education for children and their families is a cost-effective and safe control strategy that can decrease the burden of enterobiasis infection. Infection, especially enterobiasis, increases the financial burden of preventative medicine programs, part of which must be paid by the government. Therefore, it is necessary that health policymakers establish effective screening and training programs to eliminate enterobiasis.
HIGHLIGHTS
• We analyzed data on 60,167,000 children from 42 data sets
• The global prevalence of Enterobius vermicularis among the children studied was 12.9%.
• The highest prevalence rate of E. vermicularis infection (34.7%) was observed in the primary school group.
Notes
Ethics Approval
This study received approval from the Qazvin University of Medical Sciences Ethical Committee Iran under the contract no. IR.QUMS.REC.1401.291.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
None.
Availability of Data
All data generated or analyzed during this study are included in this published article.
Authors’ Contributions
Conceptualization: SD, EKL; Data curation: BH, KT; Software: SAH, AJ; Interpretation of data: AM, AT; Writing–original draft: SAH, BH, KT, AJ; Writing–review & editing: AM, SD, EKL, AT. All authors read and approved the final manuscript.
Additional Contributions
We are grateful to engineer Mr. Mostafa Sargol for his help.