Factors associated with the combination of general and abdominal obesity in middle-aged and older Korean women: a cross-sectional study
Article information

Abstract
Objectives
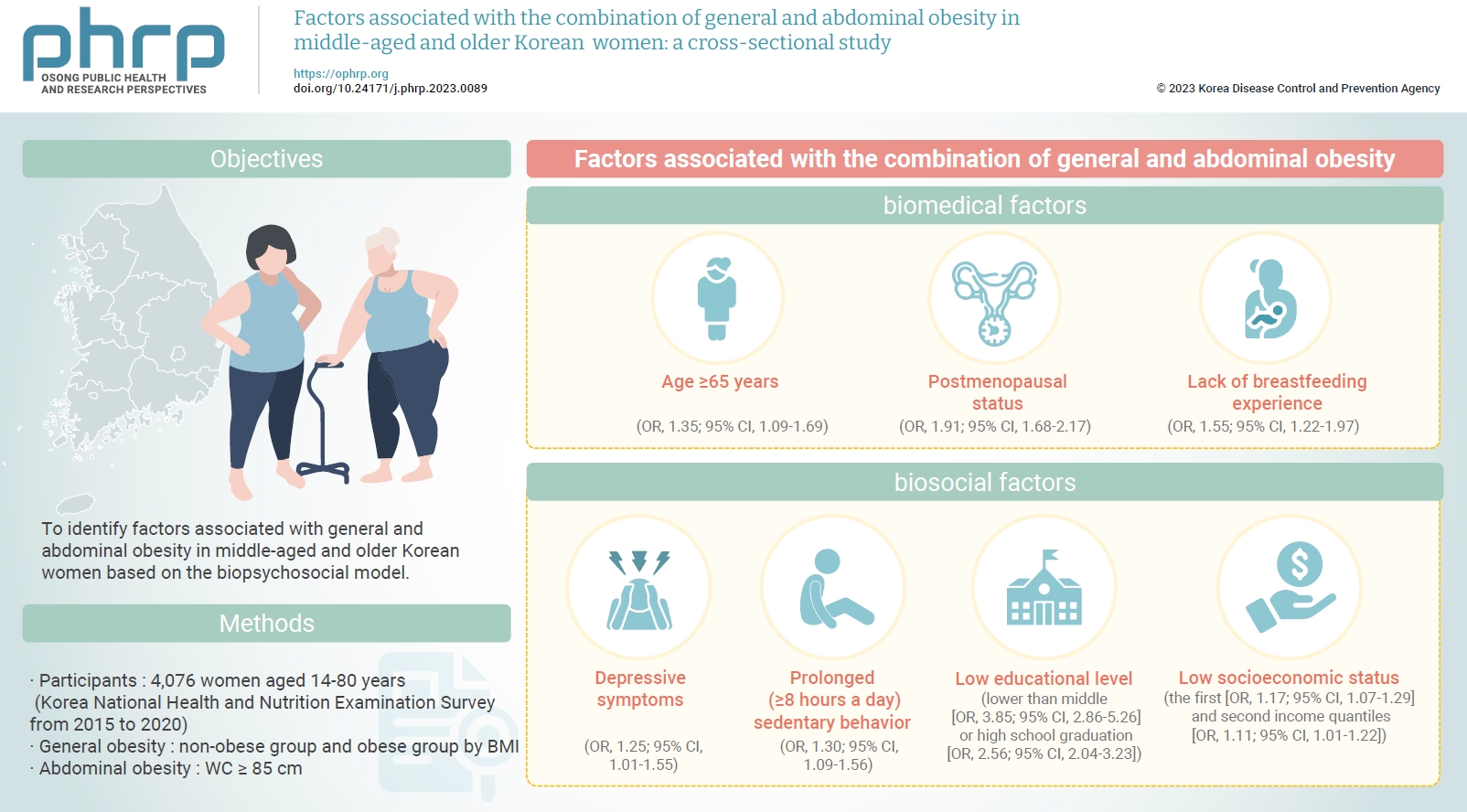
To identify factors associated with general and abdominal obesity in middle-aged and older Korean women based on the biopsychosocial model.
Methods
Data from 4,076 women aged ≥45 years who participated in the Korea National Health and Nutrition Examination Survey from 2015 to 2020 were analyzed. Complex sampling analysis was performed using IBM SPSS ver. 26.0.
Results
The combination of general and abdominal obesity was positively associated with age ≥65 years, postmenopausal status, and without breastfeeding experience among biomedical factors; depressive symptoms and prolonged (≥8 hours a day) sedentary behavior among psychosocial factors; and an educational level lower than middle or high school graduation and the first and second income quantiles among biosocial factors.
Conclusion
Healthcare providers in communities and public societies should screen for risk factors for the combination of general and abdominal obesity while considering non-modifiable biomedical (e.g., age) and biosocial factors (e.g., educational level). In addition, intervention strategies should be developed by considering modifiable psychosocial factors such as sedentary behavior.
Introduction
Obesity is a major health problem. The prevalence rates of general obesity based on body mass index (BMI) and abdominal obesity based on waist circumference (WC) have steadily increased over time [1]. According to a report on Korean national trends, the prevalence of general obesity in adults increased from 29.7% in 2009 to 36.3% in 2019, and that of abdominal obesity in adults increased from 19.0% in 2009 to 23.9% in 2019 [2]. Furthermore, middle-aged and older women aged >50 years may have higher risks than men of developing general and abdominal obesity, owing to menopause with decreased ovarian function and related aging processes [2]. According to previous studies, in middle-aged and older Korean women aged >45 years, 37.3% of those aged between 45 and 80 years were obese (BMI ≥25 kg/m2) [3], and 28.9% of those aged between 45 and 65 years had abdominal obesity with (WC ≥85 cm) [4]. Additionally, a study of Brazilian middle-aged women aged 45 to 64 years reported the prevalence rates of general obesity and abdominal obesity as 68.2% to 73.8% and 56.4% to 63.1%, respectively [5]. Thus, general and abdominal obesity may present major health problems for middle-aged and older women.
General obesity is independently associated with metabolic syndrome, cardiovascular disease (CVD), and cancer in adults, including middle-aged and older women [6,7]. Abdominal obesity is also strongly associated with a high risk of developing metabolic abnormalities (e.g., dyslipidemia, hypertension, and diabetes), CVD, cancer, and all-cause mortality [6–10]. However, previous studies have reported that the development of diabetes and CVD was associated with the combination of general and abdominal obesity [11,12]. Considering their individual effects, this combination might have synergetic effects on health, such as the development of diabetes [12]. Additionally, the risk of developing diabetes increased significantly only with the combination of general and abdominal obesity, but not with other patterns such as general obesity without abdominal obesity and vice versa [12]. Individuals with both general and abdominal obesity have a higher risk of cancer and stroke than those with other obesity patterns [7,13]. Particularly in women, the combination of general and abdominal obesity, and not other patterns of obesity alone, is significantly associated with an elevated risk of stroke [13]. Furthermore, in individuals aged >50 years, the combination of general and abdominal obesity is associated with a high risk of CVD [13]. Similarly, postmenopausal women with the combination of general and abdominal obesity have a notably higher risk of cancer (e.g., breast and endometrial cancer) than postmenopausal women with other patterns of obesity (general obesity without abdominal obesity) and premenopausal women with the combination of general and abdominal obesity [7]. Thus, the combination of general and abdominal obesity is considered a better predictor of CVD and cancer in middle-aged women [7,13]. Considering that this combination is the most common pattern of obesity in adults [13], preventing it may be important for promoting good health in middle-aged and older women. To prevent this combination, the identification of associated factors at multiple levels may be the first step in the development of health promotion strategies. However, awareness of the factors associated with the combination of general and abdominal obesity is limited, although they differ according to obesity patterns [12]. Middle-aged and older Korean women grew up in a Confucian culture that imposed stricter social norms on women than men and attributes superiority to men [14]. Thus, these women might have lower smoking and alcohol consumption than same-aged Korean men [14]. They might also be less educated than same-aged Korean men, resulting in low information about how to engage in a healthy lifestyle [15]. Therefore, the factors associated with the combination of general and abdominal obesity in middle-aged and older Korean women are different from those in same-aged Korean men and same-aged women in other countries with different cultural norms.
Several factors contribute to the development of obesity, with various underlying mechanisms. Straub [16] proposed that obesity as a complex phenomenon is influenced by biological, social, and psychological factors. According to Hoffman and Driscoll [17], the biopsychosocial model might be an appropriate framework to evaluate the effects of multivariate factors on metabolic health (e.g., abdominal obesity). Thus, the biopsychosocial model can provide a framework for a comprehensive understanding of distinctive individual characteristics associated with health status, including obesity [18].
According to the biopsychosocial model, biomedical (e.g., age and sex), psychosocial (e.g., mood and health-related behaviors), and biosocial factors (e.g., educational level and socioeconomic household status) interact to influence people’s health. Biomedical factors associated with general and abdominal obesity include age [10,19], postmenopausal status, and breastfeeding experience [20]. Psychosocial factors include depressive symptoms [21], skipping breakfast [22], eating out [22], sedentary behavior [22], physical activity (days of walking per week) [22–24], current and past smoking [10,19], and current alcohol consumption [19,25]. Among biosocial factors, educational level [10], employment [26], and household socioeconomic status [10] have been associated with abdominal obesity. Therefore, this study aimed to identify factors associated with the combination of general and abdominal obesity in middle-aged and older Korean women based on the biopsychosocial model.
Materials and Methods
Study Design and Samples
Using a cross-sectional design, secondary data analysis was conducted using the Korea National Health and Nutrition Examination Survey (KNHANES) data of 44,951 Korean individuals (20,473 men and 24,478 women) 1 to 80 years old who participated in the survey from 2015 to 2020. Of 20,176 Korean women aged ≥20 years old, 13,725 middle-aged and older women aged 45 to 80 years were selected. Finally, after excluding individuals who did not complete the questionnaires and physical examinations (height, body weight, and WC), data from 4,076 women aged 45 to 80 years old were analyzed (Figure 1).

Sampling process. KNHANES, Korea National Health and Nutrition Examination Survey.
Measurements
Dependent variables
To evaluate the combination of general and abdominal obesity, BMI and WC were measured. Obesity patterns were categorized into 4 groups: combination of general and abdominal obesity, general obesity without abdominal obesity, abdominal obesity without general obesity, and neither general nor abdominal obesity.
General obesity
To evaluate adiposity, BMI was calculated by dividing weight (kg) by height squared (m2). BMI was classified into the following categories: underweight (<18.5 kg/m2), normal weight (≥18.5 kg/m2 and <23 kg/m2), overweight (≥23 kg/m2 and <25 kg/m2), or obese (≥25 kg/m2) [27]. Regarding adiposity, participants were classified into non-obese (underweight and normal weight) and obese (overweight and obese) groups.
Abdominal obesity
Abdominal obesity was assessed using WC. A WC ≥85 cm in women indicates abdominal obesity [28].

Data Analyses
Following the guidelines for the statistical analysis of the KNHANES data, a complex sampling analysis was applied using IBM SPSS ver. 26.0 (IBM Corp.). The prevalence of obesity according to the patterns and variables of biomedical, psychosocial, and biosocial factors was analyzed using frequencies and percentages. Logistic regression analysis was applied for identification of the factors associated with the combination of general and abdominal obesity.
IRB/IACUC Approval
Since this study used the KNHANES results for secondary data analysis, the institutional review board of Chungnam National University approved the exemption of review (202210-SB-147-01). It was performed in accordance with the principles of the Declaration of Helsinki.
Results
Prevalence of Obesity by Patterns and Biomedical, Psychosocial, and Biosocial Factors
Table 2 shows that 33.1% of the participants had the combination of general and abdominal obesity. Regarding biomedical factors, 71.7% of the participants were aged 45 to 64 years old, 76.7% were postmenopausal, and 83.5% had breastfeeding experience. Regarding psychological factors, 14.7% had depressive symptoms; 75.2% and 9.1% skipped breakfast <2 days a week and 7 days a week (daily), respectively; 51.2% and 10.9% ate out 1 to 6 times a week and >1 time a day; 49.8% had prolonged (>8 hours a day) sedentary behavior, 45.4% walked >10 minutes 5 to 7 days a week, and 17.6% did not walk at all in a week; 4.9% and 4.2% were current and past smokers, respectively; and 57.5% currently consumed alcohol <1 time a month. Regarding biosocial factors, 41.6% of the participants graduated from middle school, and 51.5% were employed; regarding socioeconomic status, 22.3% reported that their monthly income was in the first quantile (lowest).

Characteristics of obesity by patterns and biomedical, psychosocial, and biosocial factors among participants (n=4,076)
Factors Associated with the Combination of General and Abdominal Obesity
The associated factors included age and postmenopausal status, depressive symptoms and sedentary behavior, educational level, and household socioeconomic status (Table 3).

Factors associated with the combination of general and abdominal obesity
Regarding biomedical factors, participants aged ≥65 years had a 1.35-fold higher likelihood of developing the combination of general and abdominal obesity than 45- to 64-year-olds (95% confidence interval [CI], 1.09–1.69; p=0.01). In addition, women aged >65 years had a higher likelihood of developing general obesity without abdominal obesity and vice versa than women aged 45 to 64 years. Postmenopausal status was associated with a 1.91-fold increased likelihood of developing the combination of general and abdominal obesity, compared with premenopausal status (95% CI, 1.68–2.17; p<0.001). A lack of breastfeeding experience was associated with a 1.55-fold increased likelihood of developing the combination of general and abdominal obesity, compared with having breastfed (95% CI, 1.22–1.97; p<0.001) (Table 3).
Regarding psychosocial factors, depressive symptoms were associated with a 1.25-fold increased likelihood of developing the combination of general and abdominal obesity, compared with the absence of depressive symptoms (95% CI, 1.01–1.55; p=0.04). In addition, prolonged (≥8 hours a day) sedentary behavior was associated with a 1.30-fold increased likelihood of developing the combination of general and abdominal obesity, compared with appropriate (<8 hours a day) sedentary behavior (95% CI, 1.09–1.56; p=0.003) (Table 3).
Regarding biosocial factors, having an educational level lower than middle school and high school graduation was associated, respectively, with 3.85-fold (95% CI, 2.86–5.26, p<0.001) and 2.56-fold (95% CI, 2.04–3.23; p<0.001) increased likelihoods of developing the combination of general and abdominal obesity, compared with college graduation. Regarding household socioeconomic status, the first and second quantiles of monthly income were associated with 1.17-fold (95% CI, 1.07–1.29; p=0.001) and 1.11-fold (95% CI, 1.01–1.22; p=0.03) increased likelihoods of developing the combination of general and abdominal obesity, respectively, compared with the fourth quantile (Table 3).
Discussion
This study was conducted to identify factors associated with the combination of general and abdominal obesity among middle-aged and older Korean women. According to the results of this study, age, postmenopausal status, and breastfeeding experience were positively associated with the combination of general and abdominal obesity. A previous study on Norwegian and Russian individuals aged 40 to 69 years showed that older women had a higher likelihood of developing general and abdominal obesity [19]. This may be linked to metabolic changes associated with aging and hormonal changes during menopause in women [31,32]. During normal aging, white adipose tissue in the abdominal cavity and fat deposition in skeletal muscle increase [33,34]. In addition, middle-aged and older women gain weight with decreased energy expenditure via increased sedentary behavior and decreased physical activity due to reduced muscle strength and physical endurance [31,35]. Lower postmenopausal estrogen levels also result in increased accumulation of adipose tissue in the abdominal cavity [32]. Thus, middle-aged and older women may be at risk of increased weight gain and WC.
In addition, middle-aged women who experienced 1–6 months of breastfeeding have shown lower general and abdominal obesity rates [36,37]. A total breastfeeding duration >3 months has been associated with a lower abdominal obesity rate in postmenopausal Korean women aged >40 years [38]. Bobrow et al. [39] reported that every 6 months of breastfeeding was associated with a 1% decrease in the mean BMI. Furthermore, a longer duration of breastfeeding was associated with a lower BMI among women with obesity 6 years postpartum [40]. In a previous study on Filipino, Caucasian, and African-American women aged 55 to 80 years [41], breastfeeding duration >3 months was associated with less visceral fat than in women with no history of breastfeeding. Since breastfeeding improves lipid metabolism [42], adipose tissue deposition in the visceral cavity during pregnancy decreases when breastmilk containing high-calorie fat is generated [43]. Thus, a longer duration of breastfeeding is associated with a greater decrease in general and abdominal obesity rates [36,44].
According to a meta-analysis, depressive symptoms are associated with general obesity in women [45,46]. Another study reported that depressive symptoms were associated among middle-aged women, though not among middle-aged men, with an increased likelihood of developing general and central obesity [21]. Furthermore, depressive symptoms have been associated with general obesity in adults who have abdominal obesity [47]. However, a previous study on middle-aged and older Chinese participants reported that obesity was not associated with depressive symptoms in women [48]. Since obesity and depressive symptoms are interrelated, they cause emotional problems (e.g., depression), resulting in an increase in emotion-driven eating (eating in response to negative emotions rather than a physical need). An increase in energy intake promotes obesity with decreased energy expenditure via low physical activity levels, due to reduced self-efficacy [49]. In particular, since middle-aged women seem vulnerable to depressive symptoms [49], they may experience increased weight and WC.
A sedentary lifestyle is associated with general and abdominal obesity in middle-aged women [50]. According to a national study, watching television and videos for 2 hours or more per day is associated with a 1.66-fold increase in general and abdominal obesity among women [22]. In addition, sitting for 8 hours or more per day has been associated with a 1.38-fold increase in the prevalence of obesity and a 1.05-fold increase in the prevalence of abdominal obesity in a population-based study [51]. Sedentary behavior is defined as participation in minimal activities requiring a resting level of energy expenditure (1.0–1.5 times the basal metabolic rate), such as watching television [52]. Thus, prolonged sedentary behavior might be associated with an overall decrease in energy expenditure, which may result in a positive energy balance, even when energy intake does not increase by eating. Therefore, interventions should be developed to decrease sedentary behavior in middle-aged and older women.
Educational level and socioeconomic status are crucial factors associated with obesity [53]. According to KNHANES data gathered from 1998 to 2018, among women, a high educational level and socioeconomic class were inversely associated with increased general and abdominal obesity rates [54]. Educational level is positively associated with access to resources to assist in a healthy lifestyle. Thus, individuals with higher educational levels have greater access to health-related resources that provide information and assistance for following healthy lifestyles [15]. A previous study reported that women with low educational levels did not follow recommendations for obesity prevention [15]. In addition, individuals currently spend more money to maintain a healthy lifestyle, including the consumption of foods without junk calories (e.g., fresh fruits and vegetables), which is beneficial for preventing excessive weight gain [55]. Thus, it may be easier for individuals with a high socioeconomic status to maintain a healthy lifestyle, which costs more. In particular, Korean women who experience social pressure to be slender (culturally ideal body weight) may try to maintain a normal weight and slender body shape with a healthy lifestyle [54]. Thus, women with a high socioeconomic status can actively maintain a healthy lifestyle, which contributes to the prevention of general and abdominal obesity, while those with low socioeconomic status and educational levels may need public support to maintain healthy lifestyles and prevent general and abdominal obesity.
In a secondary analysis of Korean national data, this study identified factors associated with the combination of general and abdominal obesity in middle-aged and older Korean women. In particular, although Lu et al. [13] reported a few factors associated with the combination of general and abdominal obesity, such as age, smoking, and alcohol consumption, the current study identified multiple factors (biomedical, psychosocial, and biosocial) associated with the combination of general and abdominal obesity based on the biopsychosocial model. The results showed that comprehensive intervention strategies should be developed to prevent and manage the combination of general and abdominal obesity in middle-aged and older Korean women. In addition, cohort studies could be proposed to identify the cumulative effects of aging with associated factors on developing the combination of general and abdominal obesity.
However, this study had some limitations. First, a cross-sectional study design was applied, which limited the verification of causal relationships among the potential factors associated with the combination of general and abdominal obesity. Further cohort studies are needed to identify causal associations. Second, the factors associated with the combination of general and abdominal obesity may differ according to sex and ethnicity. Thus, sex-based and ethnic differences need to be identified in factors associated with general and abdominal obesity. Finally, this study focused on identifying factors associated with general and abdominal obesity. Since other obesity patterns (e.g., abdominal obesity without general obesity) are also associated with obesity-related complications, further studies are needed to identify and compare the factors associated with obesity patterns.
Conclusion
According to the results of this study, women older than 65 years, with postmenopausal status, without breastfeeding experience, with a low educational level, and/or with a low socioeconomic household status may be at risk for the combination of general and abdominal obesity. Prevention and early management of depressive symptoms and decreased sedentary behavior may be important to prevent general and abdominal obesity in middle-aged and older women. Thus, healthcare providers in communities and public health clinics should screen for risk factors for the combination of general and abdominal obesity with non-modifiable biomedical (e.g., age) and biosocial factors (e.g., educational level). In addition, prevention strategies for obesity (the combination of general and abdominal obesity) should be developed with a focus on modifiable psychosocial factors (e.g., sedentary behavior).
HIGHLIGHTS
• Age >65 years, postmenopausal status, and without breastfeeding experience were positively correlated with the combination of general and abdominal obesity.
• Depressive symptoms and prolonged sedentary behavior were positively correlated with the combination of general and abdominal obesity.
• Lower educational level and lower income were positively correlated with the combination of general and abdominal obesity.
Notes
Ethics Approval
This study was approved by the institutional review board of Chungnam National University and was exempted from review because it was a secondary analysis (202210-SB-147-01). It was performed in accordance with the principles of the Declaration of Helsinki.
Conflicts of Interest
The author has no conflicts of interest to declare.
Funding
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean Ministry of Science and ICT (2021R1A2C100682811).
Availability of Data
The datasets are not publicly available but are available from the corresponding author upon reasonable request.