Analysis of pregnant women with critically severe COVID-19 in Korea from February 2020 and December 2021
Article information

Abstract
Objectives
This study aimed to describe the characteristics and risk factors for severe disease in pregnant women infected with coronavirus disease 2019 (COVID-19) from the early days of the COVID-19 epidemic in Korea to the predominant period of the Delta variant.
Methods
A retrospective cohort study was conducted among pregnant women diagnosed with COVID-19 between February 2020 and December 2021. Logistic regression analysis was performed to compare severe and mild cases after adjusting for pregnant women’s age, nationality, infection route, outbreak area, infection period, symptoms, underlying disease, smoking status, trimester, and COVID-19 vaccination status.
Results
In total, 2,233 pregnant women were diagnosed with COVID-19 by December 2021. Among these, 96.7% had mild symptoms, 3.3% had severe symptoms, and 0.04% died. The risk factors for severe disease in pregnant women with confirmed COVID-19 were being in the age group of 35 to 45 years, having hyperlipidemia, being in the second or third trimester of pregnancy at the time of COVID-19 diagnosis, being infected during the Delta-predominant period, and having a fever (≥38 °C) at diagnosis. Furthermore, 47.1% of patients in the mild group and 84.9% of patients in the severe group had 3 or more risk factors.
Conclusion
Pregnant women with COVID-19 mainly experienced mild symptoms, but those with risk factors were at a higher risk of developing severe symptoms. Therefore, treatment and follow-up management should be thoroughly implemented.

Introduction
The first case of coronavirus disease 2019 (COVID-19) was confirmed in Hubei Province, China, in December 2019. By December 31, 2021, more than 286 million people worldwide had been infected with COVID-19, which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and more than 5.4 million deaths due to COVID-19 had been recorded [1]. In the early stages of the COVID-19 pandemic, few studies were conducted to elucidate the incidence and fatality rates of COVID-19 in pregnant women, but those studies indicated that pregnant women are vulnerable to COVID-19 infection [2]. According to the United States Centers for Disease Control and Prevention, 31.5% of pregnant women and 5.8% of non-pregnant women with COVID-19 were hospitalized in June 2020. The hospitalization rate for pregnant women was 5.4 times higher than that of non-pregnant women, the rate of intensive care unit (ICU) treatment 1.6 times higher, and the rate of ventilation treatment was 1.9 times higher [3]. The immune system is affected by the physiological changes associated with pregnancy. In particular, the number of immune cells decreases in the second and third trimesters [4,5]. These immunological changes result in a higher susceptibility to infectious diseases during pregnancy due to an increased heart rate and cardiac output, increased oxygen consumption, and decreased lung volume subsequent to anatomical changes [4]. Due to these characteristic changes in pregnancy and the possibility that an infection might cause a cytokine storm, pregnant women may have a higher risk of death and complications than the general population during outbreaks of certain infectious diseases, such as influenza [6–8]. However, in a study that compared non-pregnant and pregnant women of the same age at the beginning of the COVID-19 pandemic, no differences were found in the clinical symptoms and incidence of pneumonia caused by COVID-19 [9]. Furthermore, compared to pregnant women infected with SARS-CoV-2 in the early stage of the pandemic, higher risks for ICU treatment, premature birth, and neonatal hospitalization were identified in pregnant women infected with the Alpha and Delta variants [10]. However, a study comparing pregnant women with confirmed COVID-19 to non-pregnant women in Korea from January 2020 to February 2021 found that the incidence of COVID-19 in pregnant women (0.02%) was lower than the incidence in non-pregnant women of the same age group (0.14%) and non-pregnant women of all age groups (0.15%) [11]. Furthermore, until April 2021, all pregnant women with COVID-19 in Korea were treated in general wards, while 0.87% of non-pregnant women of the same age were treated in the ICU [12]. Previous studies related to COVID-19 in pregnant women in Korea were limited to data retrieved before the period when the Delta variant predominated. Consequently, data on critically severe symptoms in pregnant women with COVID-19 are lacking. Therefore, we described the characteristics of pregnant women diagnosed with COVID-19 in Korea from the early days of the COVID-19 epidemic to the Delta-predominant period and explored the risk factors for severe COVID-19 in pregnant women. This study aimed to present a basis for establishing careful management guidelines for pregnant women, who are considered vulnerable.
Materials and Methods
Study Design and Data Sources
This was a retrospective cohort study of pregnant women with confirmed COVID-19 in Korea. Data on pregnant women diagnosed with COVID-19 between February 2020 and December 2021 were obtained from the COVID-19 Basic Epidemiological Survey System of the Korea Disease Control and Prevention Agency (KDCA). Information on underlying diseases was obtained from the National Health Insurance Service database of the National Health Insurance Corporation from January 2016 to November 2021. Data on COVID-19 vaccination status were obtained from the KDCA COVID-19 vaccination system. The study cohort consisted of pregnant women with confirmed COVID-19 in Korea. The cohort was further divided into severe and mild groups. Pregnant women (i.e., Korean and foreign women who were 20 to 45 years of age) with COVID-19 were defined as those whose COVID-19 report details were confirmed using their resident registration number and name, and who checked the pregnancy status item in the COVID-19 Basic Epidemiological Survey. All COVID-19 cases confirmed during the study period were diagnosed using real-time reverse-transcription polymerase chain reaction. Mild and severe cases were classified according to the 11th edition (February 10, 2022) of the COVID-19 response guidelines. The mild group included patients who experienced no interference with daily life activities during the isolation period (no limitation of activity), had difficulties in daily life but did not require oxygen treatment (limitation of activity but no O2), received oxygen therapy with a nasal prong (O2 with a nasal prong), or received oxygen therapy with an oxygen mask (O2 with a facial mask). The severe group included patients who required non-invasive ventilation/high-flow oxygen therapy, invasive ventilation, extracorporeal membrane oxygenation, or continuous renal replacement therapy. COVID-19 patients who died during pregnancy were defined as those who died within 28 days of infection with SARS-CoV-2 [13].
Study Population
A total of 2,235 pregnant women (i.e., Korean and foreign women who were 20 to 45 years of age) with confirmed COVID-19 based on their resident registration number or alien registration number and name who checked the pregnancy status item in the COVID-19 Basic Epidemiological Survey were selected as the study population. Among them, 2,160 patients had mild symptoms and 73 had critically severe symptoms.
Data Collection
Information on age, nationality, route of infection, period of SARS-CoV-2 infection, reported region, underlying disease, smoking status, trimester during SARS-CoV-2 infection, status of COVID-19 vaccination at the time of SARS-CoV-2 infection, symptoms at the time of diagnosis, and death were collected. Age was categorized into 2 groups: 20 to 34 years and 35 to 45 years. Nationality was classified as Korean and foreign, and infection routes were categorized as domestic outbreaks and foreign inflows. The standard infection period was based on week 31 of 2021, after the Delta variant had begun to spread in Korea and the detection rate of the Delta variant exceeded 50% based on a genetic analysis of confirmed COVID-19 patients in Korea [14]. The period up to week 30 of 2021 was defined as the period preceding the predominance of the Delta variant, and the period from week 31 to week 53 of 2021 was defined as the Delta-predominant period. The regions included Seoul, Busan, Incheon, Gyeonggi Province, and 13 other regions (Daegu, Gwangju, Daejeon, Ulsan, Sejong, Gangwon, Chungcheongbuk-do, Chungcheongnam-do, Jeollabuk-do, Jeollanam-do, Gyeongsangbuk-do, Gyeongsangnam-do, and Jeju Provinces). The underlying diseases included diabetes, hypertension, hyperlipidemia, cardiovascular disease, cerebrovascular disease, cancer, chronic lung disease, pneumonia, renal disease, liver disease, tuberculosis, and asthma. Smoking status was categorized as smoking or nonsmoking. The pregnancy stage was classified as the first trimester if the gestational age was less than 14 weeks at the time of COVID-19 confirmation, the second trimester if the gestational age was 14 to 27 weeks, and the third trimester if the gestational age was 28 weeks or more. Symptoms included fever (≥38 °C), cough, sputum, sore throat, runny nose, myalgia, dyspnea, headache, nausea or vomiting, and diarrhea.
Statistical Analysis
The frequencies (%) of all categorical variables were calculated to describe the general characteristics of the patients. Logistic regression analysis was performed to compare severe and mild cases. The pregnant women’s age, nationality, infection route, outbreak area, infection period, symptoms, underlying disease, smoking status, gestation period at the time of diagnosis, and COVID-19 vaccination status at the time of diagnosis were all adjusted. The adjusted odds ratio (aOR) for each variable is presented with a 95% confidence interval (CI). The analysis was performed after excluding missing values. A p-value <0.05 was considered to indicate statistical significance. All analyses were performed using the R software ver. 4.2.1 (The R Foundation).
Ethics Statement
Data collection was performed in accordance with Article 76-2 of the Infectious Disease Control and Prevention Act and was approved by the Institutional Review Board (IRB) of the KDCA (IRB No: 2022-11-10-PE-A).
Results
General Characteristics
This study analyzed 2,233 pregnant women aged 20 to 45 years who were diagnosed with COVID-19 between February 2020 (when the first confirmed case of COVID-19 in a pregnant woman was recorded) and December 2021. Among these patients, 2,160 (96.7%) had mild symptoms, 73 (3.3%) had severe symptoms, and 1 (0.04%) died. In total, 1,224 patients (54.8%) were aged 20 to 34 years, and 1,009 (45.2%) were aged 35 to 45 years. Furthermore, 1,933 patients (86.6%) were of Korean nationality, while 300 (13.4%) were foreign nationals. A total of 2,189 patients (98.0%) had domestic-acquired infections, and 44 (2.0%) were infected in another country. Additionally, 530 cases (23.7%) were confirmed before the Delta-predominant period, and 1,703 cases (76.3%) were confirmed during the Delta-predominant period. Seoul had the highest number of cases (n=771, 34.5%) among the 17 cities and provinces, followed by Gyeonggi Province (n=751, 33.6%), Incheon (n=135, 6.0%), and Busan (n=79, 3.5%). The remaining 13 regions had 497 cases (22.3%).
A total of 308 patients (13.8%) had at least 1 underlying disease. Among the underlying diseases of pregnant women with confirmed COVID-19, chronic obstructive pulmonary disease was the most common (n=185, 8.3%), followed by asthma (n=83, 3.7%), hyperlipidemia (n=51, 2.3%), and liver disease (n=44, 2.0%). Furthermore, 49 patients (2.2%) were smokers and 2,149 (96.2%) were nonsmokers. At the time of diagnosis, 497 patients (22.3%) were in their first trimester (<14 weeks), 909 (40.7%) were in their second trimester (14 to 27 weeks), and 767 (34.3%) were in their third trimester (>28 weeks). At the time of diagnosis, 1,921 patients (86.0%) had not been vaccinated. Moreover, 101 patients (4.5%) had received a single vaccine dose and 158 (7.1%) had received 2 vaccine doses. Among pregnant women with confirmed COVID-19, 1 death (0.04%) occurred during the Delta-predominant period. The deceased pregnant woman was started on high-flow oxygen therapy on the eighth day after being diagnosed with COVID-19, but she died 13 days later of pneumonia and respiratory failure (Table 1).

General characteristics of women with SARS-CoV-2 infection during pregnancy in Korea between February 1, 2020, and December 31, 2021
Distribution of Symptoms
Among the pregnant women with COVID-19, 321 (14.4%) were asymptomatic. At the time of diagnosis, cough (n=1,064, 47.6%) was the most common symptom, followed by fever (≥38 °C; n=969, 43.4%). Respiratory symptoms included sputum (n=462, 20.7%), runny nose (n=444, 19.9%), and dyspnea (n=75, 3.4%). Other than respiratory symptoms, sore throat (n=865, 38.7%) was the most common symptom, followed by headache (n=558, 25.0%), myalgia (n=507, 22.7%), nausea or vomiting (n=19, 0.9%), and diarrhea (n=16, 0.7%). More than half of the patients with critically severe disease had fever (≥38 °C; n=47, 64.4%) and cough (n=46, 63.0%). No gastrointestinal symptoms such as nausea, vomiting, or diarrhea were reported (Figure 1).
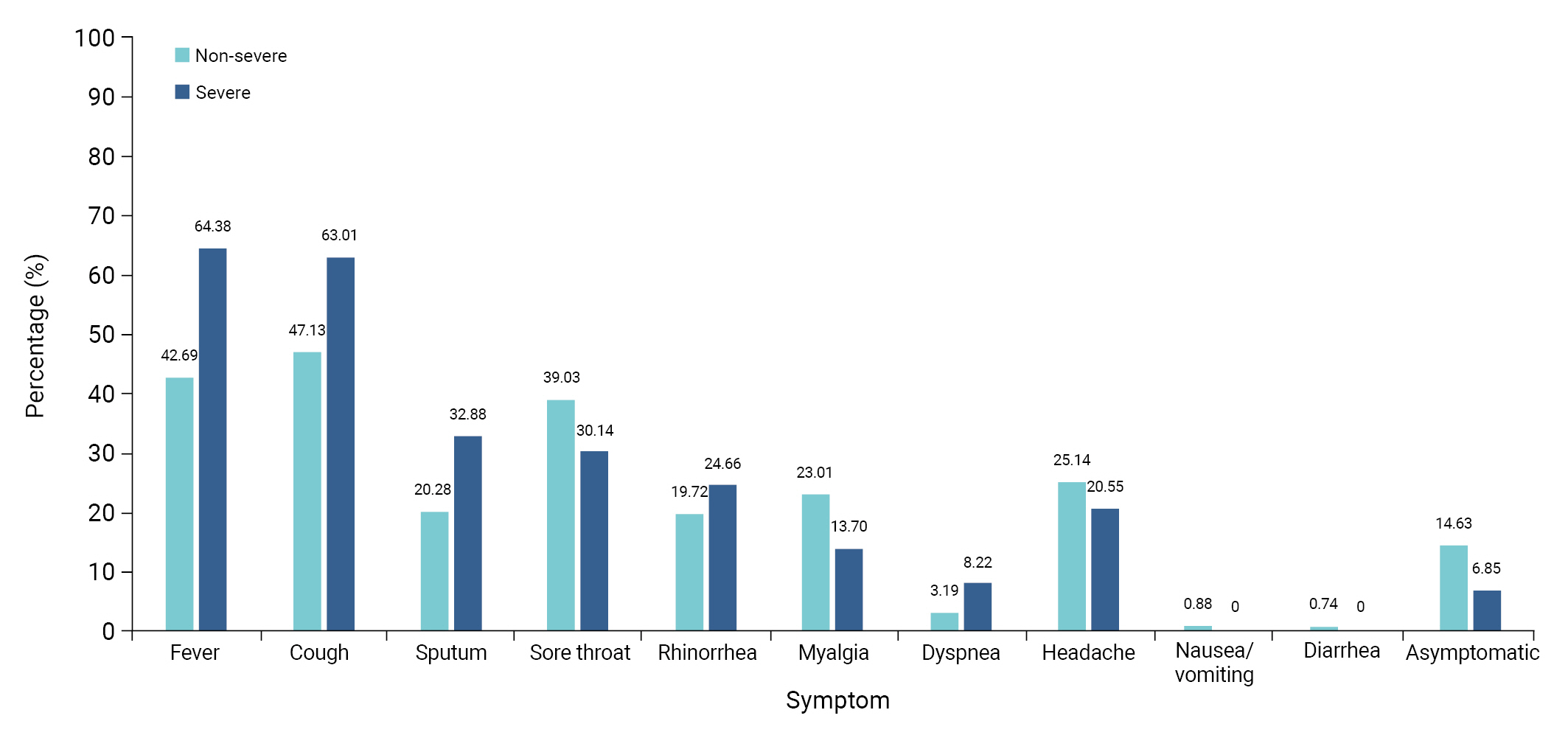
Distribution of the clinical symptoms reported by women with severe acute respiratory syndrome coronavirus 2 infection during pregnancy in Korea between February 1, 2020, and December 31, 2021.
Risk Factors
Based on a multivariate analysis, 5 risk factors were identified for severe symptoms in pregnant women with confirmed COVID-19: being 35 to 45 years of age (aOR, 2.0; 95% CI, 1.19–3.42), hyperlipidemia (aOR, 4.82; 95% CI, 1.04–17.66), being in the second or third trimester at the time of diagnosis (aOR, 11.28; 95% CI, 2.32–203.28 and aOR, 25.09; 95% CI, 5.30–449.29, respectively), being infected during the Delta-predominant period (aOR 3.37; 95% CI, 1.42–9.99), and having fever at diagnosis (≥38 °C; aOR, 2.78; 95% CI, 1.61–4.89). In contrast, myalgia (aOR, 0.34; 95% CI, 0.15–0.69) was identified as a protective factor against severe COVID-19. These significant results were obtained after adjusting for pregnant women’s age, nationality, route of infection, region of infection, period of infection, symptoms, underlying disease, smoking status, trimester at the time of diagnosis, and COVID-19 vaccination status at the time of diagnosis (Table 2).

Crude and adjusted ORs for severe symptoms in pregnant women with confirmed COVID-19
Discussion
This study sought to describe the characteristics of all pregnant women with confirmed SARS-CoV-2 infection from the beginning of the COVID-19 epidemic in Korea through the entire period of the Delta variant predominance. After exploring the risk factors for COVID-19 in pregnant women and dividing them into severe and mild cases, the distribution of risk factors was quantitatively evaluated. The identified risk factors for severe COVID-19 in pregnant women in Korea were older maternal age (35 to 45 years), underlying hyperlipidemia, diagnosis of SARS-CoV-2 infection in the second or third trimester, diagnosis of COVID-19 during the period of Delta variant predominance, and fever symptoms at diagnosis. Patients with critically severe symptoms were likely to have at least 2 of the 5 risk factors. Specifically, the proportion of patients with 3 or more of these risk factors was 47.1% (1,018/2,160) in the mild group and 84.9% (62/73) in the severe group (Figure 2). The odds ratio of critically severe illness in pregnant women with 3 or more of the 5 risk factors for severe COVID-19 (age ≥35 years, hyperlipidemia, diagnosis in the second or third trimester of pregnancy, infection during the Delta-predominant period, and fever symptoms at the time of diagnosis) was higher than that of the group with 2 or fewer risk factors. This result highlights the risk of critically severe symptoms associated with each combination of risk factors. Since the number of cases was low, the 95% CIs were relatively wide around the estimates for certain risk factors (e.g., age ≥35 years, hyperlipidemia, and diagnosis in the second or third trimester) (Table 3).
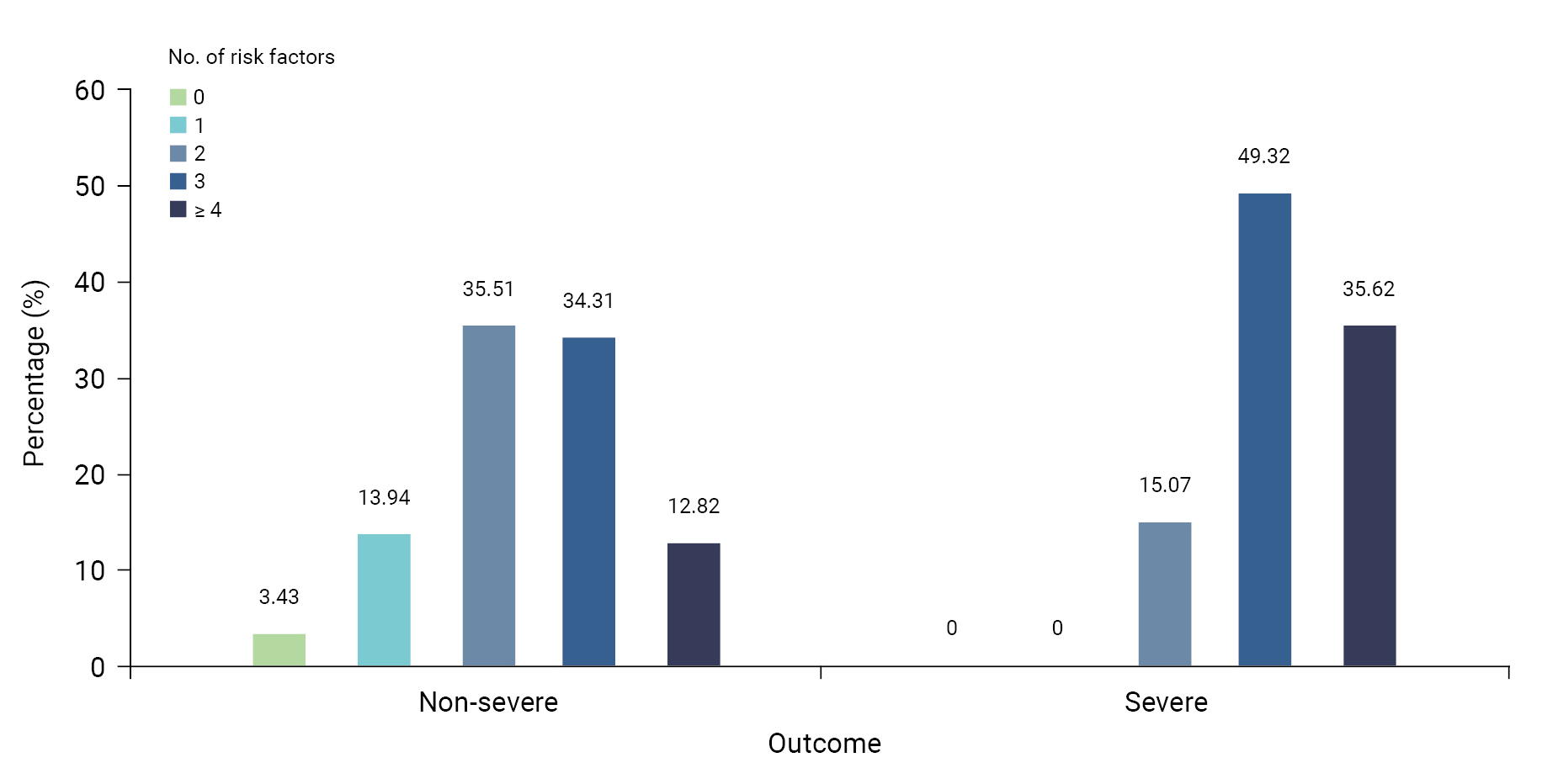
Frequency distribution based on the number of risk factors for women infected with severe acute respiratory syndrome coronavirus 2 during pregnancy in Korea.

Risk of critically severe symptoms by risk factor combinations in women infected with SARS-CoV-2 during pregnancy
This study has some limitations. First, pregnant women with confirmed COVID-19 were identified through interviews during COVID-19 epidemiological investigations. Therefore, women who checked the pregnancy status item in the COVID-19 Basic Epidemiological Survey may have been omitted or incorrectly categorized, and the total number of pregnant women with COVID-19 may have been inaccurate. Second, risk factors according to the type of treatment for each stage of severe symptoms could not be identified because it was not possible to obtain clinical information related to the treatments administered to patients with critically severe symptoms. Third, it was not possible to distinguish between the effects of underlying diseases that existed before pregnancy and those that were caused by pregnancy and perinatal complications due to a lack of relevant information.
According to a recent study of pregnant women infected with COVID-19 at 15 hospitals located in the Republic of Korea between January 2020 and December 2021, the ICU admission rate was 3.5% (9/257 people) [15], which was similar to the proportion of critically severe cases confirmed in the present study. In Korea, the rate of critically severe cases among all ages was 2.98% before the predominance of the Delta variant and 2.14% during the Delta-predominant period. During the same period, the rate of critically severe COVID-19 cases among patients aged 20 to 40 years was less than 1%, whereas pregnant women had a higher rate of critically severe COVID-19 cases [16]. However, the total fatality rate for all age groups was 0.89% (5,625/635,253 people) [17,18], while that for pregnant women was 0.04% (1/2,233 people), which was 22.3 times lower than the total fatality rate. In Scotland, 2% (114/5,653 people) of pregnant women diagnosed with COVID-19 between March 2020 and October 2021 received critical care [19]. Furthermore, early in the pandemic, the risk of ICU treatment for pregnant women in the United States was higher than that for non-pregnant women of the same age; however, the fatality rate was low [3].
According to a study conducted in the United Kingdom from March 2020 to March 2021 among COVID-19 inpatients aged 18 years or older, hyperlipidemia was associated with death (adjusted risk ratio [aRR], 1.07; 95% CI, 1.05–1.09), use of a ventilator (aRR, 1.13; 95% CI, 1.11–1.16), and ICU admission (aRR, 1.07; 95% CI, 1.05–1.09) due to COVID-19 [20]. In the present study, the risk of severe symptoms in pregnant women with hyperlipidemia was approximately 4.8 times higher than that in pregnant women without hyperlipidemia. In the future, comparative studies between the general population with hyperlipidemia and pregnant women are needed to clarify the degree to which various underlying diseases, including hyperlipidemia, increase the risk of severe COVID-19.
Regarding risk factors based on the stage of pregnancy, a study found that SARS-CoV-2 infection in the second and third trimesters may lead to abnormal circulation, placental infection, and negative perinatal outcomes [21]. The risk of critically severe disease was reported to be high in patients diagnosed after 21.5 weeks of pregnancy [15]. As pregnant women diagnosed with COVID-19 in the second or third trimester are at high risk of developing critically severe symptoms, it is necessary to implement careful prevention, promotion, and treatment interventions for pregnant women diagnosed with COVID-19 in the second trimester or beyond.
As the COVID-19 pandemic progressed, the number of confirmed cases increased. As a result, the authorities actively conducted COVID-19 testing during the Delta-predominant period compared to before the spread of the Delta variant. In June 2021, the World Health Organization recommended that women who are planning to become pregnant, are currently pregnant, or are breastfeeding be vaccinated against COVID-19 [22]. In Korea, COVID-19 vaccination for pregnant women began on October 18, 2021 [23]. Therefore, 1,921 (86.0%) pregnant women with confirmed COVID-19 in this survey were unvaccinated, and only 1 person in the severe group had received 2 doses of the vaccine. In previous studies that compared the period when the Delta variant was predominant to the period before its predominance after adjusting for vaccination history, the risk of severe COVID-19 was found to increase during the period of Delta variant predominance (OR, 2.93; 95% CI, 1.18–7.69) [21]. Thus, based on the results of that previous study [21] and the relatively short period during which pregnant women in Korea could be vaccinated during the period covered by this study, it is reasonable to interpret the increase in the number of pregnant women with severe disease during the Delta-predominant period as being associated with the Delta variant itself.
Fever (31% to 41%) and cough (31% to 41%) were the main symptoms of SARS-CoV-2 infection in pregnant women, whereas myalgia (12% to 22%) and diarrhea (4% to 6%) are relatively rare [8]. In this study, the risk of critically severe disease in pregnant women with fever was higher than that in pregnant women without fever. Physiological responses such as temperature control during infection have long-term effects on pregnant women diagnosed with COVID-19 [6], and fever during pregnancy can increase the risk of neurological disorders in the fetus [24]. Therefore, fever symptoms must be closely monitored and treated in pregnant women diagnosed with COVID-19. In the present study, myalgia was identified as a factor inversely associated with severe COVID-19; however, this result may have been due to the small number of critically severe patients who experienced myalgia. Further studies are warranted to clarify this relationship.
Conclusion
In conclusion, most pregnant women with SARS-CoV-2 infection were mildly symptomatic. However, pregnant women older than 35 years of age, those with hyperlipidemia, and those infected in the second or third trimester were significantly more likely to develop severe symptoms. Thus, treatment and follow-up management should be thoroughly implemented, and fever symptoms should be closely monitored and treated. Furthermore, pregnant women should be actively educated about these risk factors through guidelines to prevent infection. To further clarify changing patterns in infection risk as the distribution of variants changed throughout the COVID-19 pandemic, future research should investigate the overall epidemiological characteristics of pregnant women with COVID-19 during the Omicron-predominant period (i.e., in 2022 and beyond).
HIGHLIGHTS
• This study examined the characteristics and risk factors of pregnant women with COVID-19 in Korea.
• Out of 2,233 pregnant women with COVID-19 had 96.7% mild symptoms, 3.3% severe, and 0.04% death.
• Results suggest the importance of closely monitoring and treating pregnant women with COVID-19.
Notes
Ethics Approval
The collection of data in accordance with Article 76-2 of the infectious Disease Control and Prevention Act was approved by the Institutional Review Board of the KDCA (IRB No: 2022-11-10-PE-A).
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
None.
Availability of Data
The datasets are not publicly available, but are available from the corresponding author upon reasonable request.
Authors’ Contributions
Conceptualization: all authors; Data curation: JJL; Formal analysis: JJL; Investigation: JJL; Methodology: SEL, YK, YJP; Project administration: YJP; Resources: JJL; Software: JJL; Supervision: YJP; Validation: SEL, YJP; Visualization: JJL; Writing–original draft: JJL; Writing–review & editing: all authors. All authors read and approved the final manuscript.