Association between the empirical dietary inflammatory index and musculoskeletal pain in community-dwelling older adults: a cross-sectional study
Article information

Abstract
Objectives
Inflammation has been proposed to be one of the main causes of musculoskeletal pain. Diet is a lifestyle factor that plays an important role in managing inflammation; thus, we assessed the inflammatory potential of diets using the empirical dietary inflammatory index (EDII) to investigate the relationship between diet and musculoskeletal pain.
Methods
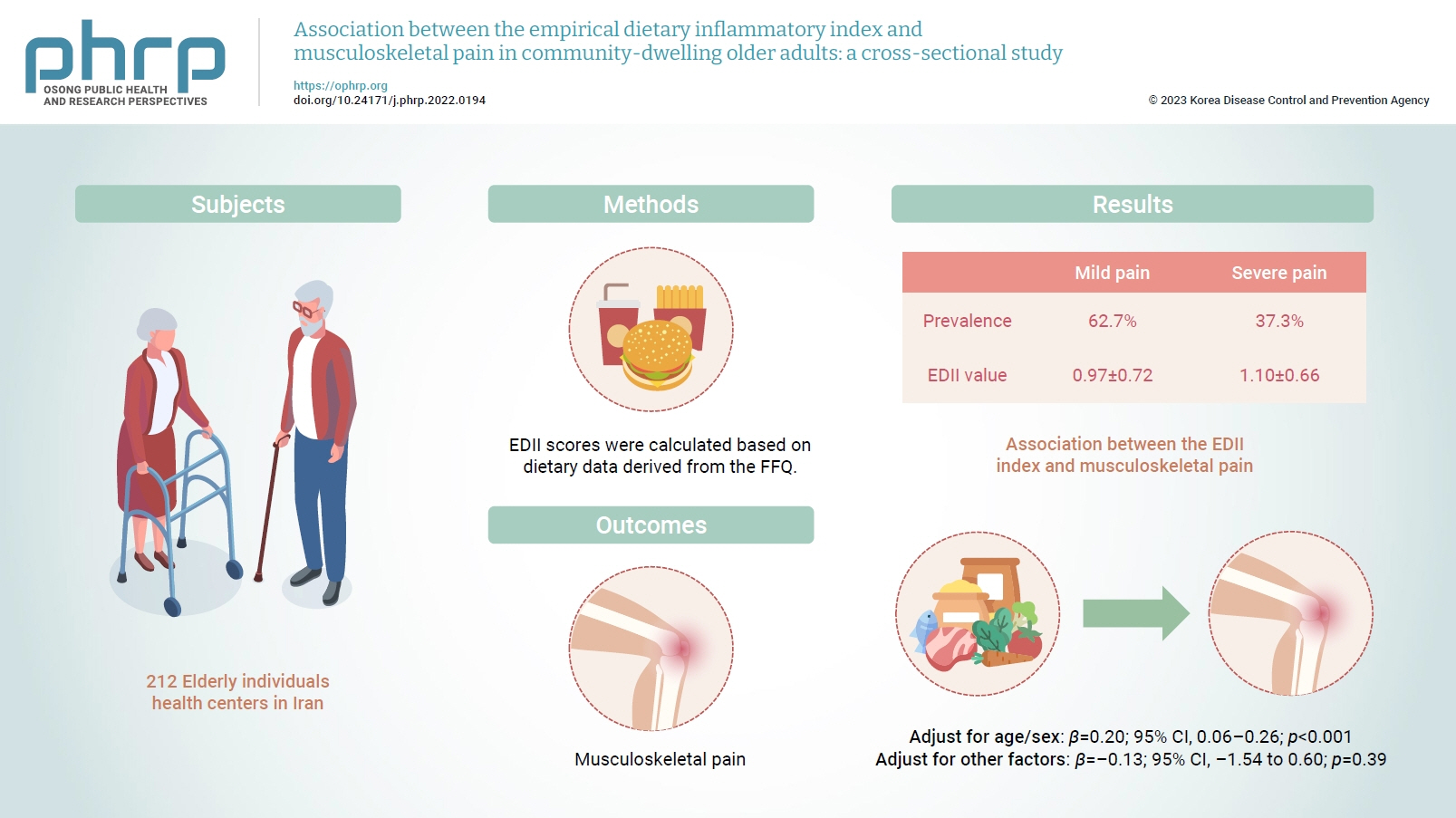
This cross-sectional study included 212 elderly individuals who were selected from health centers in Tehran, Iran. Dietary intake was evaluated using a valid and reliable 147-item food frequency questionnaire. To measure the intensity of pain, a visual analogue scale was used. Multiple linear regression was applied to assess the association between the EDII and musculoskeletal pain.
Results
In total, 62.7% and 37.3% of participants had mild and severe pain, respectively. The EDII values were 0.97±0.72 and 1.10±0.66, respectively, in those with mild and severe pain. A higher EDII score was associated with more intense musculoskeletal pain after adjusting for age and sex (β=0.20; 95% confidence interval [CI], 0.06–0.26; p<0.001), but not after adjustment for other confounders (β=–0.13; 95% CI, –1.54 to 0.60; p=0.39).
Conclusion
Our findings indicated that higher dietary inflammation might not be associated with musculoskeletal pain in older adults. However, further investigations are required to confirm these findings.
Introduction
Musculoskeletal conditions affect the soft tissues, joints, and bones, are common in the elderly [1,2], and could lead to pain, a weakened locomotor system, and disability [3,4]. These conditions could also impose a heavy economic burden on society [5]. Although the exact mechanism is still not fully understood, evidence abounds associating these conditions with inflammatory diseases such as rheumatoid arthritis and osteoarthritis [6]. It has also been shown that an excessive amount of reactive oxygen species is present in individuals experiencing musculoskeletal conditions [7], along with other inflammatory markers such as tumor necrosis factor-alpha and interleukin-6 [8]. Therefore, it is reasonable to assume that managing inflammation could be an important step in mitigating musculoskeletal conditions [9]. Chronic inflammation can be significantly tackled by making lifestyle changes such as dietary interventions [10,11].
Some dietary components such as fruits, vegetables, whole grains, and spices, have been shown to demonstrate anti-inflammatory effects due to their high antioxidant and polyphenol content [12]. Conversely, high consumption of animal proteins and fats has been indicated to induce inflammation [13,14]. However, due to the synergistic or antagonistic effects that foods have on each other, evaluating the overall dietary pattern could provide more comprehensive insights into the diet-disease association [15]. The empirical dietary inflammatory index (EDII) can be used for this purpose [16]. The EDII is a hypothesis-driven index that has been recently proposed to assess the potential pro- or anti-inflammatory effect of the diet based on the intake of various food groups [17]. Several studies have investigated associations between the EDII and chronic diseases and have shown that a higher EDII was associated with an increased risk of diabetes, metabolic syndrome, and fatty liver disease [18,19]. However, to our knowledge, the association of this dietary index with musculoskeletal pain has not been investigated yet. Given the importance of improving the quality of life in the elderly, we conducted this study to determine whether there is an association between musculoskeletal pain and the EDII in the elderly.
Materials and Methods
Study Design
This cross-sectional study was conducted among a total of 213 elderly individuals who were enrolled in our study from September 2019 to August 2020 at health centers in Tehran, Iran. We divided the city of Tehran into 5 regions (north, south, east, west, and center). Then, 20 health centers that individuals attended routinely for check-ups were selected. We tried to enroll a certain amount of people from each region to attenuate the likelihood of financial gaps among our participants. The sample size was determined employing the following formula: N=[(Z1–α/2)2 P(1–P)]/d2, using P=29, d=4.06, and α=0.05 [20]. The main inclusion criterion was being elderly (≥60 years old). The remaining inclusion criteria were as follows: having a history of musculoskeletal pain for at least 2 months, having no change in the usual dietary pattern over the previous year, being able to ambulate, not having a history of trauma or injury-related accidents, and not having cancer, acute diseases, and cognitive impairment. Participants following a special diet or those whose energy intake fell outside the normal range of 800 to 4,200 kcal were excluded from our study.
Participants’ Characteristics
After the first screening, some participants did not meet our inclusion criteria, missed the first interview, or declined to participate; eventually, 212 older adults were enrolled in the study. Socio-demographic data, including age, sex, marital status, economic status (very bad, bad, average, good, and very good) [21], educational level (up to diploma and upper diploma), exercise, sleep duration, supplement intake, history of diseases (cardiovascular diseases, diabetes, digestive diseases, psychological diseases, and skeletal disorders) and medication use, were gathered by trained researchers.
Dietary Assessment
Participants’ usual dietary intake was evaluated using a validated and reliable 147-item semi-quantitative food frequency questionnaire (FFQ) that elicited information on diet during the past 12 months on a daily, weekly, and monthly basis [22]. An expert nutritionist gathered dietary data through face-to-face interviews and converted portion sizes to intake (in grams) of each food item and nutrient. The Nutritionist IV software (First Databank Division, the Hearst Corporation; modified for Iranian foods) was used.
EDII scores were calculated based on dietary data derived from the FFQ, which has been used in previous studies [17,23]. The EDII includes 18 food groups. However, due to religious considerations, beer and wine were not included in the dietary score. Moreover, high- and low-energy beverages were considered a single food item in the FFQ. Therefore, we calculated the EDII score based on 15 food groups and 2 categorizations of inflammatory potential. The anti-inflammatory food group consisted of tea, coffee, dark yellow vegetables, leafy green vegetables, snacks, fruit juice, and pizza. Meanwhile, the pro-inflammatory group includes processed meat, red meat, organ meat, other fish (fish, or canned tuna), other vegetables (mixed vegetables, cooked mushrooms, green peppers, zucchini, eggplant, or cucumbers), refined grains, high-energy and low-energy drinks, and tomatoes. Regression coefficients were used to weigh the mean daily intake of the food groups. The obtained values were then summed and divided by 1,000. Positive scores of the EDII are an index of pro-inflammatory diets, while negative scores correspond to anti-inflammatory diets.
Pain Evaluation
A visual analogue scale, a valid, reliable, and responsive tool [24] with 0 to 10-cm lines, was used to measure the pain intensity of participants during the previous 3 months. Its score ranges from 0 to 10, with 0 indicating no pain, <3 denoting mild pain, and ≥3 corresponding to severe pain [25]. Participants were asked to draw a vertical mark on the lines to indicate their pain level.
Assessment of Other Variables
Anthropometric measurements (height, body weight, body mass index [BMI], waist circumference [WC], and hip circumference) were assessed for all participants. Height was measured in the standing shoeless position by a standard stadiometer to the nearest 0.1 cm. Body weight was assessed by a digital scale (SECA) to the nearest 0.1 kg while participants wore light clothing. BMI was calculated as weight divided by height squared (kg/m2) [26]. WC was assessed with an accuracy of 0.1 cm, at the level of the iliac crest [27], and hip circumference was recorded at the anterior superior iliac spine level [26]. Physical activity was evaluated by asking participants about their daily average time spent jogging, exercising, or engaging in other sports. The activity level was ranked into 4 categories (light, moderate, strong, and intense). Participants’ physical activity level was calculated as metabolic equivalent-hours/day [28].
Statistical Analysis
The characteristics of the study population are expressed as mean±standard deviation (for normally distributed data) or median (for data with a skewed distribution). The normality of the distribution of variables was assessed using the Kolmogorov-Smirnov test. The independent sample t-test and the chi-square test were used to evaluate the qualitative and quantitative variables, respectively.
The dietary intake of study participants across animal and plant protein tertiles was compared using analysis of covariance. All values were adjusted for energy intake. We used multiple linear regression analysis to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for musculoskeletal pain across EDII tertiles in crude and multivariable-adjusted models. Age, sex, education, economic status, physical activity, BMI, energy intake, and economic status were adjusted in the control model. IBM SPSS ver. 24.0 (IBM Corp.) was used to perform the statistical analysis. A p-value <0.05 was considered to indicate statistical significance.
Ethics Statement
All patients were informed about the characteristics of the study and signed a written informed consent form. The study protocol was reviewed and approved by the local ethical committee of Islamic Azad University, Tehran, Iran (Code: 1397.174.IR.IAU.SRB.REC).
Results
The demographics, lifestyle, work-related, and health characteristics of the participants are described in Tables 1 and 2, according to the intensity of pain. We evaluated 212 participants, of whom 48 were men (22.6%) and 164 were women (77.4%), with an average age of 66 years. The pain assessment showed that 62.7% and 37.3% of the participants experienced mild and severe pain, respectively. The BMI was 28.43±3.76 kg/m2 and 29.15±4.22 kg/m2 in those with mild and severe pain, respectively. The EDII values were 0.97±0.72 and 1.10±0.66 in participants with mild and severe pain, respectively; this difference was not statistically significant. Furthermore, 67.5% and 32.5% of participants with mild and severe pain were married. A comparison between the 2 pain groups indicated remarkable differences between them in terms of the head of the family, educational level, economic status, and psychological disorders (p=0.01, p=0.01, p=0.001, p=0.004, and p=0.003, respectively). Additionally, gastrointestinal, cardiovascular, and psychological medication intake, and vitamin D supplement usage were significantly different between the mild and severe pain groups (p=0.01, p=0.02, p=0.002, and p=0.03, respectively).

Demographic, lifestyle, work-related, and health characteristics of the study’s participants

Association of subjects characteristics, by pain severity
The dietary intake of participants by tertile of EDII scores is presented in Table 3. People in the third tertile of the EDII consumed higher amounts of total energy, protein, total fat, saturated fat, monounsaturated fat, polyunsaturated fat, fiber, processed meat, red meat, other fish, other vegetables, refined grains, and tomatoes (p<0.05). The intake of other dietary components such as carbohydrates, tea, coffee, dark yellow vegetables, leafy green vegetables, snacks, fruit juice, pizza, organ meat, and beverages did not differ according to the tertile of the EDII score.

Nutrients and food group intake of the study population across tertiles of the EDII score
Table 4 demonstrates the association between the EDII and musculoskeletal pain shown by multiple linear regression (Table 5). In the crude model, the EDII did not have a significant association with musculoskeletal pain (β=0.07; 95% CI, –1.40 to 4.17; p=0.32). After adjusting for covariates including age and sex, the association became significant (β=0.20; 95% CI, 0.06–0.26; p<0.001). However, the fully adjusted model did not show statistical significance (β=–0.13; 95% CI, –1.54 to 0.60; p=0.39).

Association between pain intensity and tertiles of the EDII

Multiple linear regression for the association of the pain score with the EDII
Discussion
The present study investigated the association between the EDII and musculoskeletal pain in older adults. A higher EDII was significantly associated with differences in nutrient and food intake Furthermore, there was a significant positive association between EDII and musculoskeletal pain after adjusting for age and sex.
Our study showed a significant association between the EDII and intake of total energy, protein, total fat, saturated fat, monounsaturated fat, polyunsaturated fat, fiber, processed meat, red meat, other fish and vegetables, refined grains, and tomatoes. As Phillips et al. [29] indicated in their study, the consumption of red and processed meats and refined cereals/grains was higher and the intake of whole grains, fish, and low-fat dairy products was lower in participants with higher pro-inflammatory scores. Similarly, Bagheri et al. [30] reported that there was a significant association between the food-based inflammatory potential of the diet and greater consumption of refined grains, red meats, high-fat dairy, soft drinks, and potatoes. In addition, different fatty acids can stimulate inflammatory processes, or anti-inflammatory cell function through various mechanisms [31]. For instance, although monounsaturated and polyunsaturated fatty acids have anti-inflammatory properties, the n-6/n-3 ratio has been shown to be associated with the inflammatory response and coagulation [32]. Since the relationship between chronic conditions and inflammation is widely recognized, it is important to pay attention to the content and the inflammation score of individuals’ diets.
Our findings showed no direct association between the EDII and musculoskeletal pain. Although studies on this topic are limited, Enrico [33] examined the relationship between the DII and chronic pain in adults, and the results showed that dietary inflammatory index (DII) scores were significantly related to the presence of neck and back pain. In addition, DII scores have been associated with pain lasting longer than 24 hours and 3 months. Similarly, Toopchizadeh et al. [34] revealed that the DII score was directly linked to pain intensity in knee osteoarthritis patients, and a higher DII score was associated with higher odds of having severe pain. In contrast, Correa-Rodriguez et al. [35] reported no association between the DII score and clinical symptoms in women with fibromyalgia. Nevertheless, they found that the DII score was associated with lower pressure pain thresholds.
Various studies have emphasized the anti-inflammatory properties of foods, which have been reported to reduce chronic pain, osteoarthritis-related pain, and neurogenic pain [36−38]. Anti-inflammatory diets can reduce pain via several putative mechanisms. Anti-inflammatory components such as flavonoids, curcuminoids, omega-3 polyunsaturated fatty acids, trombone, and taurine could have analgesic effects by preventing inflammatory signaling, regulating cyclooxygenase 2 activity, interacting with neuromodulator pathways (including the opiate receptors and the gamma-aminobutyric acid receptor signaling), targeting L-arginine/nitric oxide signaling, and reducing the production of prostaglandin E2 [37,39−41].
Although the present study was relatively novel and could further expand our knowledge of the detrimental effects of a pro-inflammatory diet, there are some limitations that should be considered. Firstly, because of the cross-sectional nature of the study, we could not infer causality. Another limitation was the small sample size. Moreover, when using an FFQ, the risk of recall bias is substantial. Additionally, since our study population only included the elderly, our results cannot be extended to other populations. Finally, due to financial constraints, we were unable to assess inflammatory blood markers, although doing so could have provided better insights into this topic.
Conclusion
In conclusion, our findings indicated no association between a higher EDII and musculoskeletal pain in older adults. However, further investigations with a larger sample size, longitudinal and interventional design, and different populations are required to deepen our knowledge of the association between dietary indices and musculoskeletal pain.
Notes
Ethics Approval
All patients were informed about the characteristics of the study and signed a written informed consent form. The study protocol was reviewed and approved by the local ethical committee of Islamic Azad University, Tehran, Iran (Code: 1397.174.IR.IAU.SRB.REC).
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
None.
Availability of Data
All data generated or analyzed during this study are included in this published article. Other data may be requested from the corresponding author.
Authors’ Contributions
Conceptualization: MaR, ADM, AD; Formal Analysis: MaR, ZT; Investigation: MaR, ZT, ZE, SD, AE, MMD, MoR; Methodology: MaR, ADM, AD; Resources: MaR, ZT, ZE, SD, AE; Project administration: ADM, AD; Supervision: ADM, AD; Writing–original draft: MaR; Writing–review & editing: all authors. All authors read and approved the final manuscript.