The Relationship Between Health-Promoting Lifestyle and Its Related Factors with Self-Efficacy and Well-Being of Students
Article information
Abstract
Objectives
Unhealthy lifestyles among young people are seriously related to incapacity and health problems in adulthood. The aim of this study was to determine the importance of a health-promoting lifestyle and its association with self-efficacy and well-being.
Methods
In this cross-sectional study, a sample of 500 students from Shahroud University of Medical Sciences (Shahroud, Iran) were randomly selected in 2017. The Persian versions of Health-Promoting Lifestyle Profile, Self-Efficacy Scale, and WHO-5 Well-Being Index were used.
Results
Among the participants, 34% of students had an abnormal imaginable well-being, and 68% of students had high self-efficacy. The mean score of a health-promoting lifestyle was 127.47 ± 19.78, which is interpreted as moderate, and the mean score of physical activity was 14.10 ± 4.95, which is poor. There was a significant relationship between well-being, and self-efficacy with health-promoting lifestyle. Age, gender, educational level, place of residence, student employment, self-efficacy, and well-being were associated with students’ lifestyles.
Conclusion
A health-promoting lifestyle of students in this study was moderate and they did not have an acceptable level of physical activity. The direct effect of well-being, and self-efficacy on lifestyle, revising students’ curriculums to improve their health behaviors, and general health indicators, can all lead to the enhancement of health-promoting lifestyles.
Introduction
University students form a large part of the young population, and as future decision makers, they are of great importance to organizations, communities and the whole country. Studying at colleges is a period in which students increasingly make independent decisions about their lifestyle and health performance [1]. The World Health Organization (WHO) defines lifestyle as distinct and identifiable behavioral patterns which derive from the interaction between personality traits, social relationships, environmental conditions, and socioeconomic status [2], playing a significant role in the health of both the individual and society. Health-promoting lifestyle has 6 dimensions of spiritual growth, health responsibility, interpersonal relationships, stress management, physical activity, and nutrition. This lifestyle, in addition to maintaining and enhancing the level of health and well-being, brings about a sense of satisfaction and self-actualization [3,4]. The lifestyle of individuals is affected by various factors such as gender, family structure, place of residence and socioeconomic conditions [5]. There is evidence that an unhealthy lifestyle among young people is adversely related to incapacity and health problems in adulthood, and if unhealthy behaviors are detected and managed at an early stage, many risk factors for health can be avoided [6–8]. Unfortunately, the prevalence of lifestyle-related conditions such as diabetes, cardiovascular diseases and cancers due to inactivity, obesity, smoking, inappropriate diet, and lack of appropriate lifestyle choices has dramatically grown among young people in recent years [4,9].
Moreover, organizations including healthcare organizations, need to promote employees to have a good general health and self-worth. Self-efficacy is a constructive power by which the cognitive, social, emotional and behavioral skills of an individual are organized efficiently to achieve different goals, and it is an important factor for the successful performance of the individual, and for acquiring the basic skills necessary for accomplishing things [10,11].
Medical students have a great role in educating community members (including patients), and attempts to improve students’ lifestyles aspects will ultimately enhance the health status of the community. In other words, having a good lifestyle and having enough routine physical activity on the part of healthcare workers is likely to encourage patients to take action to improve their health [12–14].
Health-promoting behavior among students at various medical universities, have shown elevated levels of high-risk behaviors among students. Therefore, to improve their health status, more understanding of the influential factors is necessary to promote a healthy lifestyle [3,6,15–21].
In a study conducted in China, few students had a desirable healthy lifestyle [6]. Some studies in Malaysia, Hong Kong, Iran, Jordan and Turkey indicated a moderate level of lifestyle among medical students [12,22–29]. Lifestyle, gender, marital status [22–24], educational level, parental education, family economic status, smoking, and general health [25] may all affect a healthy lifestyle.
Since life at university is a transitional stage when students leave home and become independent some factors such as having a tight schedule, being away from family, skipping meals, using fast foods, dieting, as well as the type and amount of physical activity, may affect the students’ lifestyles. Therefore, being aware of their lifestyle, and modifying it where necessary may alleviate problems in adulthood for themselves and maybe their community. Considering the importance of this issue, the aim of this study was to determine the status of health-promoting lifestyle among university students, and its association with self-efficacy and well-being.
Materials and Methods
In this cross-sectional study performed in 2017, 500 medical students were randomly selected through a multistage stratified sampling method. At the first stage, according to the total number of the students studying in the university, it was decided that 25% of the students in each faculty (school of health, school of medicine, school of nursing and midwifery and school of para-medicine) would be selected as the samples of the study. In the next step, according to the number of semesters and fields of study in each faculty, 25% of them were randomly selected. The response rate was 93%.
This study was approved by the Ethics Review Committee of Shahroud University of Medical Sciences, Shahroud, with the code of IR.SHMU.REC.1396.06. The questionnaire used in the study consisted of 2 parts. Part 1 included 15 items on demographic characteristics of age, gender, field of study, academic level, number of semesters, marital status, native or non-native to the city, current place of residence, economic status of the family, economic activities alongside education, parental place of residence, number of family members, and father’s job. Part 2 included Health-Promoting Lifestyle Profile [9,30], Self-Efficacy Scale [31], and WHO-5 Well-Being Index [32]. The Health-Promoting Lifestyle Profile has 6 dimensions including nutrition (8 items), physical activity (8 items), health responsibility (13 items), stress management (5 items), interpersonal relationships (8 items), and spiritual growth (10 items) on a 4-point Likert scale which ranges from never to always. The score for each item ranges from 1 to 4 and the total score can range from 52 to 208. The scores obtained in each subgroup, as well as the total scores, are divided into 3 categories. Scores of 49% and below indicate a poor health-promoting lifestyle, scores between 50% and 74% indicate a moderate and scores of 75% and above indicate a good health-promoting style. A reliability of 0.82 was reported for this profile in Iran [5]. The Self-Efficacy Scale [31] contains 17 items on a 5-point Likert scale which ranges from strongly disagree to strongly agree and each item is scored from 1 to 5. Items 1, 13, 8, 9, 3 and 15 are scored in reverse. Higher scores indicate a stronger self-efficacy and lower scores reflect a poorer self-efficacy. Questions 1–7 relate to the willingness to initiate behavior, items 8–13 are related to willingness to expend effort, and items 14–17 are on persistence in the face of adversity. This scale has a maximum score of 85 and a minimum score of 17. The score of 58 and above represents a high self-efficacy, and scores less than 58 are indicators of low self-efficacy. WHO-5 Well-Being Index has 5 items, each of which is scored from 0 to 5, and the total score on this scale can range from 0 to 25. Scores less than 13 indicate an abnormal, imaginable well-being, and a score of 13 or over indicates a good well-being status. The reliability of WHO-5 Well-Being Index is reported to be 0.94 among students [32]. The questionnaires were self-administered by the students and after completion they were analyzed using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA) through ANOVA, Chi-square, t-test, backward regression model and Pearson correlation coefficient, at a significant level of 0.05.
All procedures performed in this study involving students were in accordance with the ethical standards of the Shahroud University of Medical Sciences Ethics Review Committee and with the Declaration of Helsinki (and its later amendments).
Results
In this study, 500 (205 males and 295 females) students from Shahroud University of Medical Sciences were assessed. Among them, 34% suffered from abnormal imaginable well-being and 68% had high self-efficacy. The mean age of the participants was 21.79 ± 2.68 years, and the average score of health-promoting lifestyle was 127.47 ± 19.78, (moderate level), and the mean score of physical activity was 14.10 ± 4.95 (poor level). The mean score of general health was 13.97 ± 5.65 and the mean score of self-efficacy was 60.71 ± 8.61 (Table 1).

Mean scores of lifestyle variables among the participants.
The Chi-square test showed no significant relationship between gender, marital status, being native to the city, place of residence, economic status of student’s family, parental place of residence, father’s job, semester and year of studying at university with self-efficacy (p ≤ 0.05). However, the Chi-square test showed a significant relationship between the field of study and self-efficacy (p = 0.033) so that students of public health, occupational health, and medicine showed higher levels of self-efficacy compared to those in other fields. There was also a significant relationship between the educational level and self-efficacy (p = 0.046), and medical doctorate students showed a higher self-efficacy compared to those in bachelor’s and master’s programs. Moreover, the Chi-square test showed a significant relationship between general health and self-efficacy (p = 0.007). The Chi-square test showed no significant relationships between gender, educational level, or program, marital status, field of study, being native to the city, place of residence, economic status of the family, parental place of residence, student’s economic activities, father’s occupation, life and death of the parents, and semesters or years of studying at university with general health status (p ≤ 0.05; Table 2).

Relationship between lifestyle variables with self-efficacy and general health.
Results of the t-test showed a significant relationship between general health, spiritual growth, personal relationships and physical activity with self-efficacy (p ≤ 0.05). Also, there was a significant relationship between self-efficacy, health-promoting lifestyle, spiritual growth, responsibility, personal relationships, stress management, nutrition and physical activity with general health (p ≤ 0.05; Table 3).
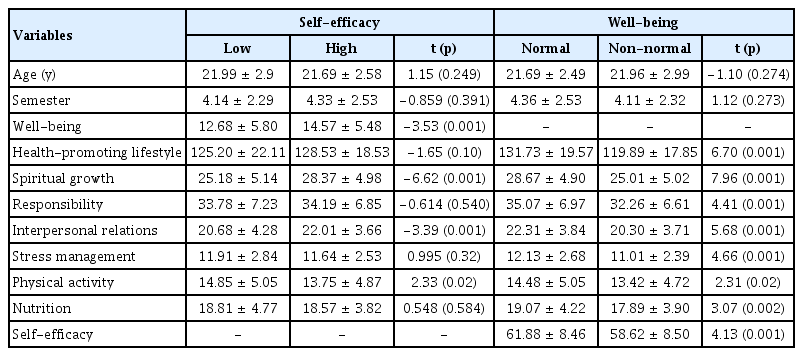
Comparison of mean scores of lifestyle variables in terms of self-efficacy and well-being categories.
Pearson correlation coefficient showed that there was a significant relationship between general health and self-efficacy with health-promoting lifestyle (r = 0.171, p = 0.001). Moreover, a significant association was observed between well-being and health-promoting lifestyle (r = 0.358, p < 0.001) and well-being and self-efficacy (r = 0.210, p < 0.001).
A backward regression model was used to determine the factors affecting the lifestyle of the students. The variables of being native to the city, father’s occupation, age, semester, economic status of the family, field of study, marital status, gender, educational level, place of residence, economic activity during studying, self-efficacy and general health were entered into the model, and it was observed that age, gender, educational level, place of residence, economic activity during studying, self-efficacy and well-being, significantly influenced the health-promoting lifestyle of the students (p ≤ 0.05; Table 4).
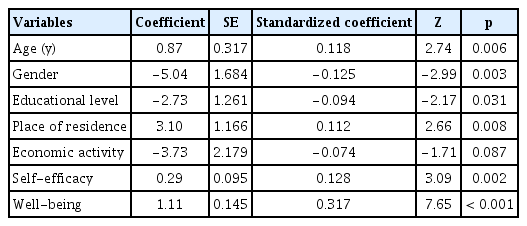
Backward regression model for factors related to students’ lifestyle.
Discussion
The health-promoting lifestyle among the students was moderate according to the mean, which is consistent with some studies [12,22–29]. However, it has been reported that the lifestyle of students of medical sciences is not desirable, which is not consistent with the results of this study. This difference in the scores appears to be due to differences in cultural and social contexts.
The mean score of spiritual growth was 27.35 ± 5.24 which is moderate and consistent with some national and international studies [22,25,27]. A high score and a desirable status of spiritual growth among the students has been reported [26] which can also be interpreted as due to cultural and social and religious differences in other countries.
The mean score of health responsibility was 34.05 ± 6.97, which is interpreted as moderate, and it is in line with another study [27]. Some studies reported lower scores, which are not consistent with the results of the present study [22–26]. This may be related to their studying fields. This current study was conducted in medical students and their responsibilities can be influenced.
The mean score of personal relationships was 21.59 ± 3.91. This indicates a moderate level and is consistent with the results of some studies nationally and internationally [22–24,26,27]. The results of another study indicated a better situation in this dimension among students, contrary to the results of this study [25]. The mean score of stress management was 11.73 ± 2.64, which is moderate, and in line with the results of other studies [22–27]. The mean score of physical activity was 14.10 ± 4.95 which is poor, but consistent with the results of another study [27]. Other studies showed that students had a better score in this dimension [22–26], a finding which is not consistent with the results of the present study. Considering the importance of this issue, it seems possible to improve the scores on this dimension through raising awareness, and creating the required opportunities, and allocating space and sports facilities.
The mean score on the nutrition dimension was 18.65 ± 4.14, which is moderate and consistent with the results of some studies [22–26] but does not conform with another study [27]. It seems the differences in scores obtained in all dimensions of the health-promoting lifestyle are due to differences in cultural and social contexts.
A significant relationship was observed between the health-promoting lifestyle of students and age. Some studies have also reported such a relationship [23–25,27], while some others found no significant relationship between these 2 variables [28,29]. In addition, there was a significant relationship between health-promoting lifestyle and gender, which is consistent with the results of some studies [22–24], but it does not correspond to the findings of some other studies [25,27–29]. Marital status also showed no significant relationship with students’ health-promoting lifestyle contra to some studies [25,28].
There was no significant relationship between the health-promoting lifestyle of the student, and his or her being native to the city, father’s job, semester, economic status of the family, the field of study, and place of residence. Nacar et al [25] pointed out in their studies that there was a correlation between the economic status of the family and the health-promoting lifestyle, which was not consistent with the results of the present study. Abeer et al referred to the lack of relationship between the economic status and the health-promoting lifestyle [26], which was consistent with the results of this study. The results of this study are partly consistent with the results of Babanezhad [29], which showed no relationship between being native to the city and lifestyle. However, the authors found a significant relationship between the field of study and lifestyle [29], which does not align with the findings of the current study.
There was a significant relationship between the health-promoting lifestyle of students and their well-being. Moreover, self-efficacy showed no significant relationship with age, gender, marital status, being native to the city, place of residence, economic status of the family, student’s economic activity, father’s occupation, parent’s place of residence, life or death of the parents, and semester year of studying at university. However, there was a relationship between self-efficacy and the field of study, and educational level. Some studies confirmed the association between self-efficacy, gender, and age, but it does not align with the results of this study [33]. The mean score of self-efficacy in this study (60.71) was higher than that reported by Arshadi et al (49.26) [33]. This is probably due to the difference between the types of universities the students attended. Arshadi et al [33] focused on universities affiliated with the Ministry of Science and Technology, but the universities in this study were affiliated with the Ministry of Health.
No significant relationship was observed between well-being and age, gender, field of study, educational level, marital status, being native to the city, place of residence, economic status of the family, student’s economic activity (employment), parental place of residence, father’s job, life or death of the parents and academic year of the student. However, a significant relationship was observed between general health, spiritual growth, personal relationships, and physical activity with self-efficacy. Moreover, there was a significant relationship between self-efficacy, health-promoting lifestyle, spiritual growth, responsibility, personal relationships, stress management, nutrition and physical activity with general health. The results of this study are not consistent with the findings of the study by Kaldi et al [28] on the relationship between general health and student employment during studying.
This study was a well-designed study with large sample size that used standardized questionnaires. However, this is a cross-sectional study and association in this study must be interpreted cautiously. In addition, a specific group of students (including medical sciences students) were studied, therefore the findings of this study are not general to all students.
Conclusion
Health-promoting lifestyle was moderate among the students in this study and students did not have an acceptable level of physical activity. The direct effect of general health and well- being, and self-efficacy on a health-promoting lifestyle requires planning for improvements such as revising students’ curriculums to improve their health behaviors and taking note of general health indicators.
Acknowledgments
This study was funded by Shahroud University of Medical Sciences.
Notes
Conflicts of Interest
The authors declare that they have no conflicts of interest.