Factors Affecting Activity Limitation in the Elderly: Data Processed from the Korea National Health and Nutrition Examination Survey, 2016
Article information
Abstract
Objectives
The aim of this study was to compare the sociodemographic characteristics, depression, and the health-related quality of life outcome, among the Korean elderly population, with and without activity limitation.
Methods
The data used was drawn from the raw data of the seventh Korea National Health and Nutrition Examination Survey (N = 8,150). There were 1,632 records for individuals aged 65 or older extracted from the seventh Korea National Health and Nutrition Examination Survey database, 199 of those had missing responses (n = 1,433). Differences within the sociodemographic characteristic, the Patient Health Questionnaire-9, and the EuroQol-5 Dimension were analyzed using logistic regression analysis according to the presence or absence of activity limitation.
Results
The prevalence of activity limitation among the elderly individuals surveyed was 19.9%. In the unadjusted regression analysis, the odds ratios of all independent variables (age, gender, education level, type of region, family income, the Patient Health Questionnaire-9, all 5 domains of the EuroQol-5 Dimension) between the elderly individuals with and without activity limitation, were significant. Although, in the adjusted logistic regression analysis, it was observed that the only factors that were significantly associated with activity limitation were the Patient Health Questionnaire-9, EuroQol-5 Dimension, type of region, and family income.
Conclusion
These findings demonstrated that activity limitation in elderly individuals is associated with the sociodemographic characteristics of family income and type of region of residence, as well as depression and the health-related quality of life outcome.
Introduction
Extrapolating from the statistics reported in 2018, about 14.3% (7.4 million) of the total Korean population of 51,635,256, are elderly, and it is estimated that this percentage will increase to 47.7% by 2045 [1]. The physical abilities of elderly individuals in terms of balance, muscle strength, and circulatory and respiratory functions, have been shown to diminish with age due to the decrease in the size and number of muscle fibers [2]. Middle-aged people also experience a loss of social role as they become older, and consequently suffer from lower self-esteem, and increased alienation and loneliness [3,4].
Quality of life is defined as “the state of subjective well-being of the physical, mental, and socio-economic aspects associated with purpose, expectations, interests of the individual in their culture, and values in which the individual lives” [5]. Relative to the general population, the elderly have a higher incidence of psychological disorders such as depression, and these disorders lead to a lower quality of life [6]. These psychosocial factors have been shown to be related to “the elderly poverty problem” [7]. Although the elderly population in Korea had rapidly increased between 2000 and 2019, life expectancy is now on the decline [8]. The decline in the health of the elderly population is leading to increased social and economic costs.
Activity limitation is defined as “a dimension of disability” or “health capturing long-lasting limitation in performing general activities” (due to health problems) [9–14]. Activity limitation is one of the important health indexes for the elderly [9]. In Japan, research has shown that while activity limitation is known to occur at all ages due to impairment, the elderly was significantly more likely to have activity limitation than the middle-aged, and young people [10]. Campbell et al [11] and Gerbi et al [12] have studied factors that related to activity limitation in the elderly in the United States, and found that aspects of mental health and socio-demographic factors need to be considered when gathering health-related information. Livingston et al [13] suggested that the increase in the numbers of cases of depression and reduced cognitive functioning in the elderly in the United Kingdom, was due to the onset of activity limitation.
Recently in 2018, Kim [14] reported the factors affecting activity limitation in the elderly of Korea were due to sociodemographic characteristics such as age and education level, as well as musculoskeletal pain and other diseases. However, depression and quality of life were not specifically considered in this report. There have been only a few studies that included quality of life and depression in the quantitative analysis of factors influencing activity limitation in the Korean elderly population [9–14]. Thus, the aim of this study was to compare the sociodemographic characteristics, depression, and the health-related quality of life (HRQOL) outcome among the Korean elderly population, with and without activity limitation. The observations from the present study may provide significant information to aid in the improvement of regional and national healthcare policy design.
Materials and Methods
1. Participants
This study used raw data from the seventh Korea National Health and Nutrition Examination Survey (KNHANES). The data provided by the KNHANES are government-designated statistics as defined in Article 17 of the Statistics Act. The seventh KNHANES was approved by the Institutional Review Board in Korea, Centers for Disease Control and Prevention. There were 1,632 participants in this study (among the 8,150 total participants of the KNHANES) who were aged 65 years or older. Of the 1,632 participants, 199 had missing values and were excluded from the analysis. Therefore, 1,433 individuals were selected for this study.
2. Dependent variables
In the KNHANES, the health interview’s criteria for an activity limitation was that the limitation must be 1 year old or older. The following question was used to determine whether the participant had an activity limitation: “Are you currently restricted in your daily life and social activities due to problems with your health, either physically or mentally?” The answer was given as “yes” or “no”. The author coded yes = 1 and no = 0 for analysis.
3. Independent variables
The independent variables were sociodemographic characteristics, depression, and the HRQOL outcome. The sociodemographic characteristics were age (65–69 = 0, 70–74 = 1, 75–79 = 2, ≥ 80 = 3), gender (male = 0, female = 1), education level (≤ elementary school = 0, middle school = 1, high school = 2, ≥ college = 3), type of region (urban = 0, rural = 1), and family income (converted to dummy variable, quartile, low = 0).
For measuring depression, the KNHANES included the Patient Health Questionnaire-9 (PHQ-9) assessment tool. The PHQ-9 was developed by Spitzer et al [15], and is scored on a scale from 0 to 27 with 0 to 4 for normal levels of depression, 5 to 9 for mild depression, 10 to 19 for moderate depression, and 20 or more for severe depression. For the analysis, the severity of depression according to the PHQ-9 the values were converted into a dummy variable, and the normal level was set to zero (normal = 0, mild depression = 1, moderate depression = 2, severe depression = 3). In this study, a Cronbach’s alpha value for the PHQ-9 was 0.797.
The HRQOL outcome was measured with the EuroQol-5 Dimension (EQ-5D). The EQ-5D is divided into 5 areas: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression [16]. For analysis, all 5 regions were converted to dummy variables, and normal levels were set as references (normal = 0, mild limitation = 1, moderate to severe limitation = 2). In the present study, the value of Cronbach’s alpha for the EQ-5D was 0.794.
4. Statistical analysis
All statistical methods were applied using SPSS version 22.0 (IBM Co., Armonk, NY, USA). The sociodemographic characteristics, depression, and the HRQOL outcome of the participants were analyzed using frequency analysis. To determine a Cronbach’s alpha value for the PHQ-9 and the EQ-5D, reliability analysis was used. Logistic regression analysis was carried out to examine the association between dependent and independent variables. In the initial (unadjusted) pass of this examination, univariate analysis was performed. In the final (adjusted) pass, multivariate analysis was performed. In other words, in order to identify the odds ratio between elderly individuals with and without limitation, adjusted random-effects logistic regression analysis was applied. Statistical significance was set at 0.05.
Results
The sociodemographic characteristics of the individuals are reported in Table 1. The frequency analysis was based on the study population n = 1,433 participants. The oldest participants were 65–69 years old (33.6%) and there were more females (55.5%) than males. The education level of most individuals was elementary school (59.6%). Most participants reported living in a rural area (62.0%). The family income range reported by the most elderly participants was in the lowest income quartile (48.4%). The number of individuals who reported an activity limitation was 19.9%.

Sociodemographic characteristics between elderly Koreans with and without activity limitation.
Table 2 shows the percentage of total individuals with and without limitation relative to the responses for depression and the HRQOL outcome. Out of all the participants, the percentage of those who were observed to have normal levels of depression as determined by the PHQ-9 was 77.0%, mild depression was 13.7%, and moderate depression was 8.4%. The mobility domain of the EQ-5D showed 60.8% of participants within the normal range and 37.8% with a mild limitation. In the other domains (self-care, usual activities, pain/discomfort, and anxiety/depression), the percentage of individuals scoring within the normal range of function was 88.1%, 77.7%, 63.0%, and 83.9%, respectively.
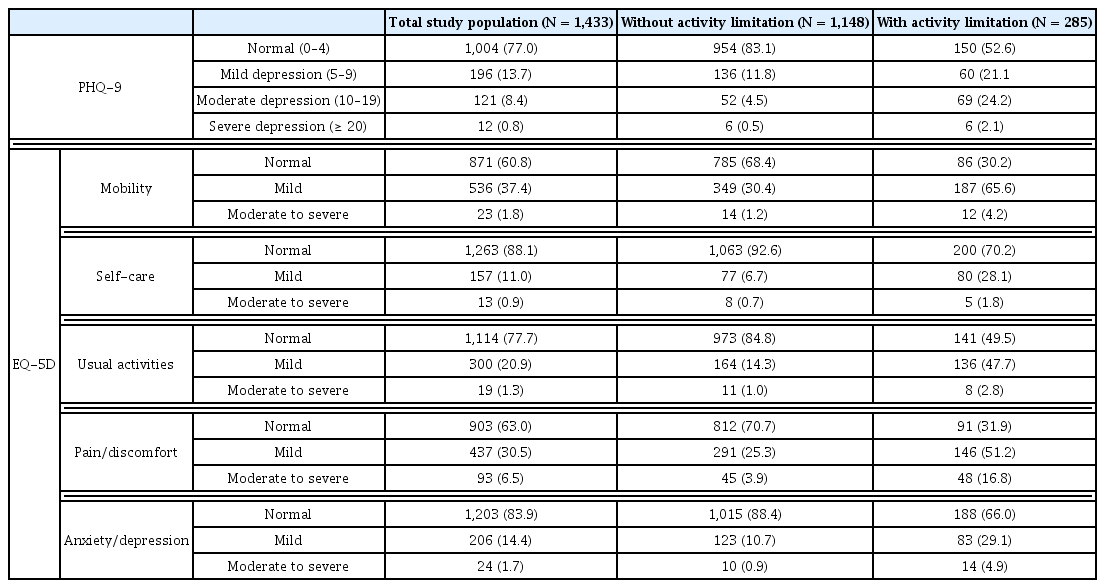
Depression and health-related quality of life experienced by elderly Koreans with and without activity limitation.
Table 3 shows the unadjusted and adjusted values of the logistic regression analysis. In the unadjusted logistic regression model, individuals with activity limitation were significantly higher or had lower odds ratio, for all independent variables (age, gender, education level, type of region, family income, the PHQ-9, and the 5 domains of the EQ-5D), compared with those without activity limitation. However, in the adjusted logistic regression model only the type of region of residence, family income the PHQ-9, and 4 domains of the EQ-5D were shown to be significant factors. Individuals with activity limitation had significantly higher odds (OR = 2.903, 95% CI = 2.042–4.127) of living in an urban area compared with older individuals without activity limitation. In terms of family income, individuals in the low to middle income range had higher odds (OR = 1.815, 95% CI = 1.282–2.913) than those in the low-income range. Individuals with activity limitation had significantly higher odds (mild, OR = 1.932, 95% CI = 1.282–2.913; moderate, OR = 5.056, 95% CI = 3.117–8.201; severe, OR = 4.188, 95% CI = 1.137–15.429) of depression compared with those without activity limitation. In terms of the 5 domains of the EQ-5D, except for anxiety/depression, individuals with activity limitation had significantly higher odds for mobility (mild, OR = 1.873, 95% CI = 1.261–2.780), self-care (mild, OR = 2.067, 95% CI = 1.320–3.238), usual activities (mild, OR = 1.910, 95% CI = 1.266–2.882), and pain/discomfort (mild, OR = 2.178, 95% CI = 1.486–3.191, moderate to severe, OR = 2.221, 95% CI = 1.183–4.171).

Factors affecting activity limitation of the elderly population in Korean.
Discussion
This study showed that there was a difference between the unadjusted and adjusted logistic regression model. Kim [14] reported a statistically significant relationship between activity limitation and age, and education level. Using adjusted logistic regression analysis, the observations of this study showed no statistically significant relationship between activity limitation and age, or education level, but did find statistically significant relationships between activity limitation and income level, and type of region. This was consistent with the observations of previous studies [11,12]. In China, socioeconomic variables were also reported to be a strong predictor of functional status [7].
Among all the independent variables examined in this study, depression showed the highest odds ratio and was identified as the strongest factor associated with activity limitation in the elderly. Monma et al [10] recently reported that mental health was the most important factor that related to activity limitation in the elderly. In their study, socioeconomic variables statistically significantly correlated with activity limitation when analyzed using an unadjusted regression model. However, in the adjusted regression model (which included additional risk factors), there was no statistically significant association [10]. Similar observations were made in the present study. These differences were the result of depression being associated with other independent variables such as gender, and education level [17,18].
Of the 5 domains of the EQ-5D, the domains that were related to activity limitation included mobility, self-care, usual activities, and pain/discomfort. Anxiety/depression of the EQ-5D was not associated with activity limitation. This was because the PHQ-9 was highly related to activity limitations. Therefore, the HRQOL outcome and activity limitation were highly related. Similar observations were reported by other studies regarding the HRQOL outcome and activity limitation [11,19,20]. The pain/discomfort domain of the EQ-5D showed a higher association with activity limitation than the other domains. Kim [14] reported that the cause of activity limitation was related to thoracic and neck pain, arthritis, and rheumatism. Studies examining significant associations between activity limitation and musculoskeletal pain have been reported [10,14,21,22].
This study has identified the factors affecting activity limitation, but it has limitations. Firstly, the study sample size was small. Secondly, the number of elderly people with and without activity limitations was not balanced. Thirdly, because this study was a cross-sectional study, causation was not clearly established.
The findings of this study imply that for the elderly population income level, type of region of residence, depression, and quality of life can predict activity limitation. In order to help prevent activity limitation in the elderly population, the gap in healthcare service use (in urban and rural areas) should be minimized [23–25], and the accessibility of healthcare services should be maximized for low-income elderly population. In addition, local communities and government agencies need to provide long-term health care programs designed specifically to prevent activity limitation in the elderly.
Notes
Conflicts of Interest
None.