COVID-19 Pandemic in Hong Kong and Gaza Strip: Lessons Learned from Two Densely Populated Locations in the World
Article information
Abstract
The emergence of the coronavirus pandemic led to the implementation of several precautionary measures across the globe. For densely populated regions in the world, this may have been challenging given the proximity of people to one other. Thus, this brief report sought to compare the measures across 2 densely populated locations, Hong Kong and Gaza. Epidemiological data was obtained from governmental online repositories and was compared with the data presented by the Johns Hopkins coronavirus map to ensure consistency. Descriptive statistics were used to interpret the data obtained over the period of the study. The data suggested that although Hong Kong and Gaza implemented similar strategies, Gaza recorded marginally higher cases compared with Hong Kong in the same timeframe. The strategies implemented in both settings included border closures, social distancing, proper hand hygiene, and mask usage. Cultural and socio-demographic differences may have played a part in this variation in case numbers, in addition to lessons Hong Kong had previously learned from a similar outbreak. As the pandemic is ongoing it is essential that public sensitization to adherence to precautionary measures at the personal/family level does not occur.
Introduction
Following the emergence of the first case of coronavirus disease 2019 (COVID-19) on 29th December, 2019, in Wuhan, China [1–3], all countries around the world have adopted several precautionary measures to limit the spread of the virus. Most countries closed their borders, stopped flights, and imposed a curfew. Despite all these precautions, the virus has spread rapidly around the globe [4] and brought significant challenges to all aspects of life [5]. In response to the high incidence rates of infection, the World Health Organization declared the disease as a global pandemic in March 2020 [6,7].
Despite the rapid spread of COVID-19, some settings such as mainland China, Hong Kong, and Japan have successfully controlled the pandemic by relying on their previous experience in dealing with infectious diseases, robust healthcare systems, and precautionary measures [8–10]. However, other countries such as USA, Italy, and Spain seem to be battling the pandemic despite their existing well-organized healthcare systems [11,12]. The precautionary measures undertaken by some governments seem not to have had a significant impact on minimizing the spread of the virus [13], particularly in regions with a high-density population [14]. Hong Kong, with a population of 17,311 people per square mile [15], depends on social distance and partial lockdown measures for controlling the spread of the virus. In contrast, the Gaza Strip with a population of 13,064 people per square mile [16] imposed a curfew and other restrictive measures but reported a significant increase of cases. Thus, learning from the experiences of countries that have been successful in controlling the spread of COVID-19 is critical.
Numerous reports have been published presenting lessons from countries that seem to have been successful in managing the pandemic. For instance, Chung et al [17] provided lessons from the Taiwanese perspective. Although the authors observed the awareness and sensitivity of citizens to the COVID-19 pandemic, they also expressed concerns about the adequacy of personnel protective devices such as surgical masks and alcohol hand sanitizers. Wong et al [18] also highlighted the impact of the precautionary measures that were undertaken by the Hong Kong government, such as social distancing and compulsory mask usage. They also noted that personal protective behaviors played a significant role in controlling the spread of the virus within the community. Similarly, Duong et al [19] provided lessons from Vietnam government on controlling COVID-19 which showed that screening and surveillance, guarantees, suspension of flights, borders, and schools’ closures, and transparent risk communication were the most efficient measures for controlling the pandemic. Despite the importance of these findings, there is currently no study comparing the effects of the varied precautionary measures taken by countries that share similar characteristics such as population density, amongst other characteristics.
To this end, the current report focused on comparing the precautionary measures that were implemented by the governments of 2 of the world’s most densely populated settings, that is, Hong Kong and Gaza in responding to a pandemic. This study also estimates the incidence rates of COVID-19 cases in Hong Kong, the Gaza Strip, and worldwide. It also summarizes key lessons that would help in combating the spread of COVID-19. Understanding the processes of precautionary measures from 2 of the most densely populated settings in the world with different economic levels (i.e., Hong Kong with a high level of resources and the Gaza Strip with a low level of resources) would help countries to manage their situations based on the availability of their resources.
Materials and Methods
Epidemiological data regarding COVID-19 were obtained from the respective governmental online repositories (Hong Kong and Gaza) during the period 24th August to 14th September, 2020. These data were reviewed and downloaded into separate Microsoft Excel worksheets. The incidence and mortality rates published on the government websites were monitored daily to update the worksheets and to ascertain the variations. At the end of each day, the reported data was compared with the John Hopkins COVID-19 map to ensure consistency. Following several days of tracking the incoming data daily, descriptive statistics were employed to display the data and draw comparisons across the data set.
Results and Discussion
1. Estimated incidence rates of COVID-19 pandemic in the Hong Kong and Gaza Strip
Hong Kong is a special administrative region located in the southern part of the People’s Republic of China, with a population of 7.50 million [15]. This population density, in addition to its proximity to mainland China, made it more vulnerable to the spread of COVID-19 [18]. A total of 4,972 confirmed cases were recorded between 22nd January, 2020 and 14th September, 2020 (Table 1), of whom 101 people died; the case fatality rate was 0.02, and the mortality rate per 100,00 head of population was 1.34 [20].

Estimated incidence rates of COVID-19 in Hong Kong, the Gaza Strip, and worldwide (24th August to 14th September, 2020).
The Gaza Strip is a part of Palestine located on the eastern coast of the Mediterranean Sea, with a population of 1.99 million [16]. The population density makes it more at risk for COVID-19. On the 21st March, 2020, Gaza Strip announced its first confirmed imported COVID-19 case. While the first local confirmed case was recorded on the 24th August, 2020, since that time, the number of confirmed cases increased sharply to 1,927 cases by the 14th September, 2020 [21]. Fifteen people out of the total confirmed cases died; the case fatality rate was 0.01, and the mortality rate per 100,00 was 0.75 (Table 1).
2. Measures undertaken by Hong Kong and Gaza Strip authorities
Hong Kong applied precautionary measures quickly and decisively to control the spread of COVID-19. The experience gained from the severe acute respiratory syndrome (SARS) outbreak in 2003 [22,23] enabled this prompt action. There were 1,755 cases of SARS in Hong Kong which resulted in 299 deaths; hard lessons were learned [8]. After the SARS outbreak, Hong Kong’s government revised its laws, regulations, guidelines, and established institutions for the control of infectious diseases and epidemics. Establishing these steps prior to the COVID-19 outbreak enabled Hong Kong to manage the epidemic and apply precautionary measures such as mandatory guarantees, social distancing, wearing masks, and screening, prior to COVID-19 becoming a pandemic.
Gaza did not have prior experience related to the control/management of a pandemic and had never been confronted with such a risk. However, Gaza learned from other countries and issued restrictive precautionary measures to control the pandemic. The protective measures by the governments of Hong Kong and the Gaza Strip are presented below:
2.1. Mandatory quarantine
According to the “Compulsory Quarantine of Certain Persons Arriving at Hong Kong Regulation,” Hong Kong imposed a compulsory home and governmental quarantine of 14 days for all inbound travelers to Hong Kong [24]. Upon arrival at Hong Kong international airport, deep throat saliva samples from passengers were collected at the designated areas of the airport. Within 6–8 hours, the results were released. Positive cases were sent to nearby hospitals for medical treatment. People who were in close contact with a positive case were sent to government quarantine centers. During compulsory quarantine, a wristband was fastened by the staff of the Health Department at the airport. In addition, inbound travelers filled out a health declaration form and installed a “StayHomeSafe” application (app) on their smart phones. The app recognized communication signals and recorded the location of the dwellings. If a person left the place of quarantine without permission, it was detected by the app. Further actions and spots checks were then conducted by government staff. Prosecution or a wanted warrant was issued to people who violated the rules of compulsory quarantine in Hong Kong [25].
In the Gaza Strip, all arriving citizens were detained in governmental buildings for a 21-day quarantine period, irrespective of the results of the reverse transcription-polymerase chain reaction (RT-PCR) COVID-19 test [21,26]. Positive COVID-19 cases were treated at hospitals while negative cases were detained in schools, hotels, or health centers. Recently, 3 quarantine buildings with a bed capacity of 2,500 have been built. All people under quarantine were tested prior to discharge to confirm that they were free from the virus. The confirmed cases at this point were referred to the hospital for treatment and follow-up, while negative cases were permitted to go home. For community confirmed cases, there was a 21-day governmental quarantine. People who were in close contact with COVID-19 infected cases were also tested, and positive cases were sent to the hospital [21,26].
2.2. Control of borders/partial and complete lockdown
From the 25th March, 2020, all non-Hong Kong residents travelling from overseas countries were denied entry [24]. However, residents of Hong Kong were permitted to enter the city. As for ferry terminals, passenger clearance services were suspended. In the Gaza Strip, the government closed both border control points:- the Rafah border crossing and the Erez Crossing. The government opened borders only 4 times between March and August to help citizens outside Gaza to return. All Palestinian citizens who were not native underwent a medical examination [noncontact temperature screening (using thermal imaging) and clinical assessment (lab investigation)] at border checkpoints, followed by quarantine for 21 days.
2.3. Screening and surveillance
The Hong Kong government launched the Universal Community Testing Program from the 1st September, 2020 to break the chain of COVID-19 transmissions. There were 141 community testing centers set up, and this was a free service provided to the public [27]. In the Gaza Strip, since the 24th August, all patients visiting Accident and Emergency departments underwent clinical examination and were asked if they had a fever or respiratory symptoms. All suspicious cases of COVID-19 were tested using RT-PCR. Healthcare professionals who were working at Gaza hospitals also underwent the RT-PCR test [21].
2.4. Communication with the public
Transparency and an information campaign were the other strategies that helped Hong Kong to combat the spread of COVID-19. The key strategies implemented earned the trust, cohesion, and collaboration of the community. Since January 2020, the Hong Kong government set up an online dashboard website aimed at disseminating detailed reporting and information about COVID-19. The online dashboard website presents the latest COVID-19 situation covering the number of confirmed cases, discharged cases, and number of deaths with location details across Hong Kong.
A daily press conference was launched by the Palestinian Ministry of Health and Ministry of Interior to update the latest situation about COVID-19 in Gaza governments. A daily report of information was also displayed on the Gaza’s Ministry of Health website, which covers the number of swab tests performed, the number of confirmed cases, the number of deaths, and the overall cumulative number of COVID-19 cases.
2.5. Availability of protective equipment
Quick, mass production of masks, hand sanitizer, and personal protective equipment (PPE) were another contributory factor to Hong Kong’s success in handling the spread of the virus. For instance, in February 2020, the Hong Kong Polytechnic University students designed reusable face shields for all Hong Kong hospitals to ease the urgent demand for protective equipment among frontline healthcare providers. In February 2020, reusable face shields were available to those who were in need in the community [28]. The University also provided 1 free reusable face shield for students upon request. The availability of different types of face masks and hand sanitizers with a reasonable price in the stores enabled the citizens to adhere to the government rules and regulations.
In the Gaza Strip, at the start of the epidemic, there was a severe shortage of PPE in Gaza health facilities and consequently access to PPE to the public was scarce. By April, Gaza started to produce high-quality devices and export this equipment. Now masks are available to the public at a low price (50 masks for 2.5 US dollars).
3. Responsibilities of the public
Although Hong Kong has experienced a third wave of COVID-19, it has reported a low incidence of COVID-19 cases during the period 24th August to 14th September, 2020 (Figure 1), and this is likely to be attributable to its citizens’ discipline at adopting stringent levels of personal infection control measures [18]. A recent survey revealed that the majority of Hong Kong citizens practiced safe self-care measures (95% of participants washed their hands thoroughly, and 99% began wearing a mask when the first few cases of COVID-19 were reported [29]. Hong Kong citizens have cultivated the norm to don a surgical mask in public places, thereby preventing a surge of infections in the community. Adherence and awareness of social distancing measures were emphasized in Hong Kong communities. The Hong Kong government adopted the “suppress and lift” approach [30]. Citizens were advised to keep 1-meter distance away from others. Group gatherings were minimized and crowded places were avoided. Under the Prevention and Control of Disease Ordinance regulation (Cap. 599), group gathering of more than 2 people was strictly prohibited (4th September, 2020 to 10th September, 2020) [31].
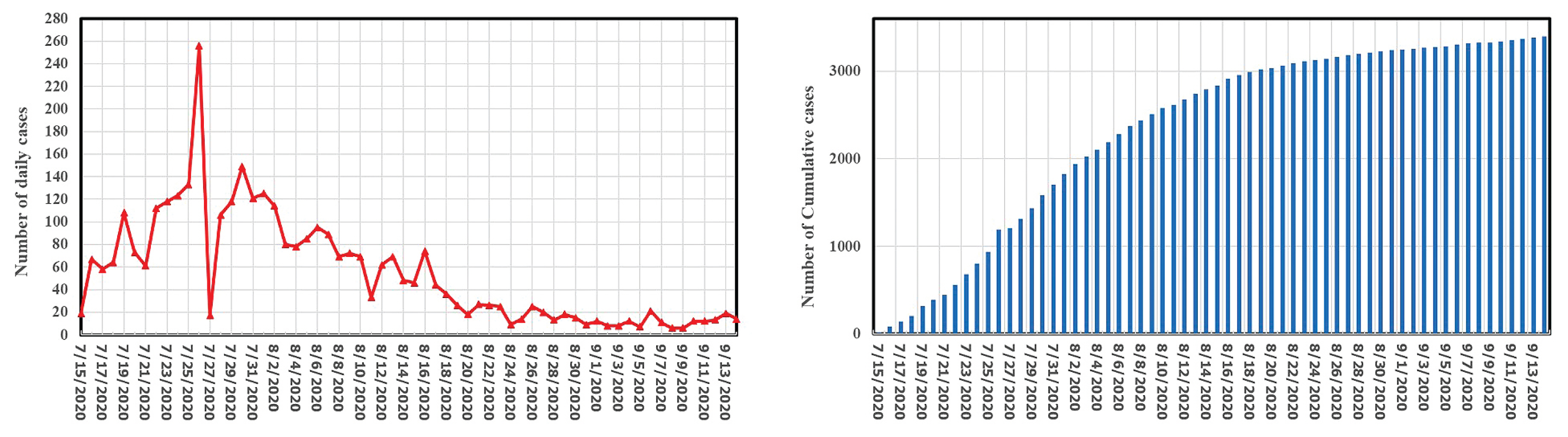
The number of recorded cases of Covid-19 in Hong Kong from 15.07.2020 to 13.09.2020 on daily basis (left) and the cumulative number of cases (right).
Although the Palestinian government ran educational programs about the importance of wearing a mask and hand washing to minimize the risk of spread of COVID-19, only a minority of citizens adopted a high level of personal infection-control measures [32]. A lack of awareness of Gazan people and ignorance of the risks and potential fatalities which the virus may cause, led to an increase in the incidence rate of COVID-19 (Figure 2). Since the public have a false sense of safety and a feeling that the virus is not in the community and is contained in quarantine departments, they did not respond to governmental instructions. Arabic social habits and behaviors such as shaking hands and kissing also played a key role in increasing the spread of the virus. In addition, water was unavailable for washing due to challenges with water refill during the period of the 24th August to 14th September, 2020 which may have led to poor hygiene, and the supply of electricity in the home being cut off for more than 20 hours per day which will have led to citizens not following the curfew as requested. In the last 2 weeks of the study period (24th August to 14th September, 2020), there was a marked improvement in the responsibility of the public.

The number of recorded cases of Covid-19 in the Gaza Strip from 23.08.2020 to 14.09.2020 on daily basis (left) and the cumulative number of cases (right).
4. Lessons to learn from Hong Kong and Gaza Strip on control of pandemic
The governments of Hong Kong and Gaza Strip, adopted similar approaches to reduce community transmissions of COVID-19 (Table 2). For instance, both locations had compulsory quarantine for its residents, screening, and surveillance to detect COVID-19, and the governments convened an online dashboard, and daily press conferences to inform the citizens to help prevent increasing rates of infectious. One interesting point to note is that, although all borders were closed in the Gaza Strip, and Hong Kong permitted entry to its residents the number of COVID-19 cases in Gaza steeply increased from August-September 2020 compared with Hong Kong (Figure 2).

Comparison of different management strategies to minimize COVID-19 transmission in the community.
Despite the efforts of the Gaza government, the majority of people did not adhere to the government’s measures which required them to stay at home during curfew. Moreover, people did not wear masks whilst out walking or when mixing in crowds, and this was in addition to public negligence towards the government and other expert advice about reducing the spread of COVID-19. Furthermore, a lack of social responsibility combined with risky social habits such as hand shaking, and kissing may have further increased the spread of the virus. Other factors such as large families and the extended family brought large numbers of people together to communicate and share in social events and played a role in increasing the spread of the virus.
In Hong Kong, people have drawn from past experiences and learnt from the SARS outbreak in 2013. Therefore, since the first reports of COVID-19 it became a “cultural norm” for Hong Kong residents to wear mask and practice strict hand hygiene [18].
In a study by Moustafa [33], it was reported that scientific and medical knowledge must be emphasized in the Arab world to fight rumors and fake news related to COVID-19 transmission. Therefore, the Gaza government’s efforts to convey information about COVID-19 through a daily press conference may not be sufficient. However, at a community level, religious leaders, and teachers may further inform the public on minimizing the spread of COVID-19, and this may be deemed useful to combat fake news. Further effort to inform the public on COVID-19 will be essential in minimizing the human and social costs of the disease.
Hong Kong, as a developed Special Administrative Region, is self-sufficient in terms of funding for PPE (such as surgical masks, ventilators, gloves, goggles, respirators), and COVID-19 testing kits. However, in the Gaza Strip, infection rates and deaths are high because people do not have sufficient money to purchase a mask and hand sanitizer. In addition, water was unavailable for washing during the period of study which may have led to poor hygiene, and the supply of electricity in the home was cut off for 20 hours or more every day which prevented people from complying with hand hygiene practices due to challenges with water refill. These restrictions contribute to a lapse in strict hand hygiene practice, together with the lack of funding for essential PPE (masks, gowns, ventilators), puts Gaza at risk of increased transmission of COVID-19. It is therefore crucial for aid and relief packages to reach Gaza in a timely manner to ease the COVID-19 related health crisis.
Conclusion
The study sought to highlight lessons learned from 2 densely populated areas in the world regarding the management of the COVID-19 pandemic. The findings suggest that despite the similarities in precautionary measures across the 2 locations, Gaza appeared to be experiencing marginal increases in case rates compared with Hong Kong. Although several factors may explain this occurrence, including the socio-demographic, and cultural context of the 2 settings which seems to have played significant roles. As it stands now, the COVID-19 pandemic has set out a new, normal way of life, for an unspecified period. Thus, precautionary measures such as hand hygiene, use of masks, and quarantine amongst others measures need to be strengthened.
Notes
Conflicts of Interest
The authors have no conflicts of interest to declare for this report.