Coronavirus Disease-19: The First 7,755 Cases in the Republic of Korea
Article information
Abstract
We report the first 7,755 patients with confirmed COVID-19 in Korea as of March 12th, 2020. A total of 66 deaths have been recorded, giving a case fatality proportion of 0.9%. Older people, and those with comorbidities were at a higher risk of a fatal outcome. The highest number of cases of COVID-19 were in Daegu, followed by Gyeongbuk. This summary may help to understand the disease dynamics in the early phase of the COVID-19 outbreaks, and may therefore, guide future public health measures.
Introduction
Only a few weeks after the first case of coronavirus disease 2019 (COVID-19) was reported in Wuhan, China, the first case of COVID-19 was confirmed in the Republic of Korea on January 20th, 2020 [1]. International travel has facilitated the spread of COVID-19 throughout the world. As of March 13th, 2020, 118 countries, territories, and areas have reported COVID-19 cases, however, differences in patterns and intensity of transmission ranges were observed [2]. In February and early March in Korea, a sharp increase in the number of COVID-19 cases were observed, with most infections in specific clusters and geographical regions.
Based on the surveillance data, we report the basic epidemiological characteristics of COVID-19 to examine the early course of the pandemic. Furthermore, factors associated with COVID-19 cases and fatality were investigated to provide information on a vulnerable part of the population to guide public health prioritization.
Materials and Methods
This is a summary of the first 7,755 patients with confirmed COVID-19 in Korea as of March 12th, 2020. To obtain demographic, epidemiological, and early clinical information, COVID-19 reporting and surveillance data were retrieved from Korea Centers for Disease Control and Prevention (KCDC)-operated National Notifiable Disease Surveillance System (NNDSS) [3]. The patient age was provided on the date of diagnosis, and key indicators such as estimated duration of exposure, date of onset of symptoms, and route of transmission were identified by field epidemiological investigators [1]. It must be noted that the data presented in this summary may change depending on the results of further epidemiological investigations.
Results
As of March 12th, 2020, a total of 7,755 laboratory-confirmed cases of COVID-19 and 66 deaths were recorded in Korea, giving a case fatality proportion of 0.9% (Table 1). The female-to-male ratio of confirmed COVID-19 cases was 62:38. The age group 20–29 years accounted for the highest level of all confirmed cases at 28.9%, followed by 50–59 years, and 40–49 years. The case fatality proportion was 0.1% among 30–39 years and 40–49 years age groups, then increased to 0.4% in the 50–59 years, 1.5% in the 60–69 years, 5.0% in the 70–79 years, and 8.5% in the ≥80 years age groups (Table 1).
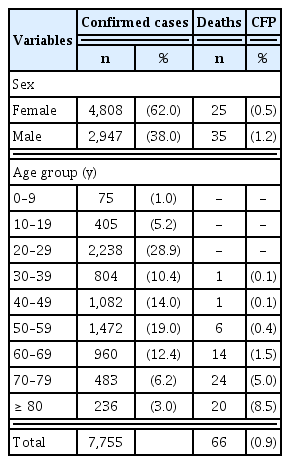
Demographics and case fatality proportion of the first 7,755 laboratory-confirmed COVID-19 cases, as of March 12th 2020, Republic of Korea.
The epidemic curves presented in Figures 1 and 2 were generated using National Notifiable Disease Surveillance System (NNDSS) data. Epidemic curves by date of onset preceded epidemic curves by date of diagnosis, by a few days or a week (Figure 1). It must be noted that the date of symptom onset may change depending on further epidemiological investigation, and delayed reporting of cases. Figure 2 depicts an epidemic curve by different regions of Korea: the nationwide, Daegu, Gyeongbuk, and others (outside Daegu and Gyeongbuk). From mid-February, an increased number of cases were reported with a peak in late February and early March. Figure 3 shows the age distribution and sex ratio among Daegu, Gyeongbuk, and others regions. Note the increased proportion of cases in 20–29 years and in females among cases in Daegu and Gyeongbuk.
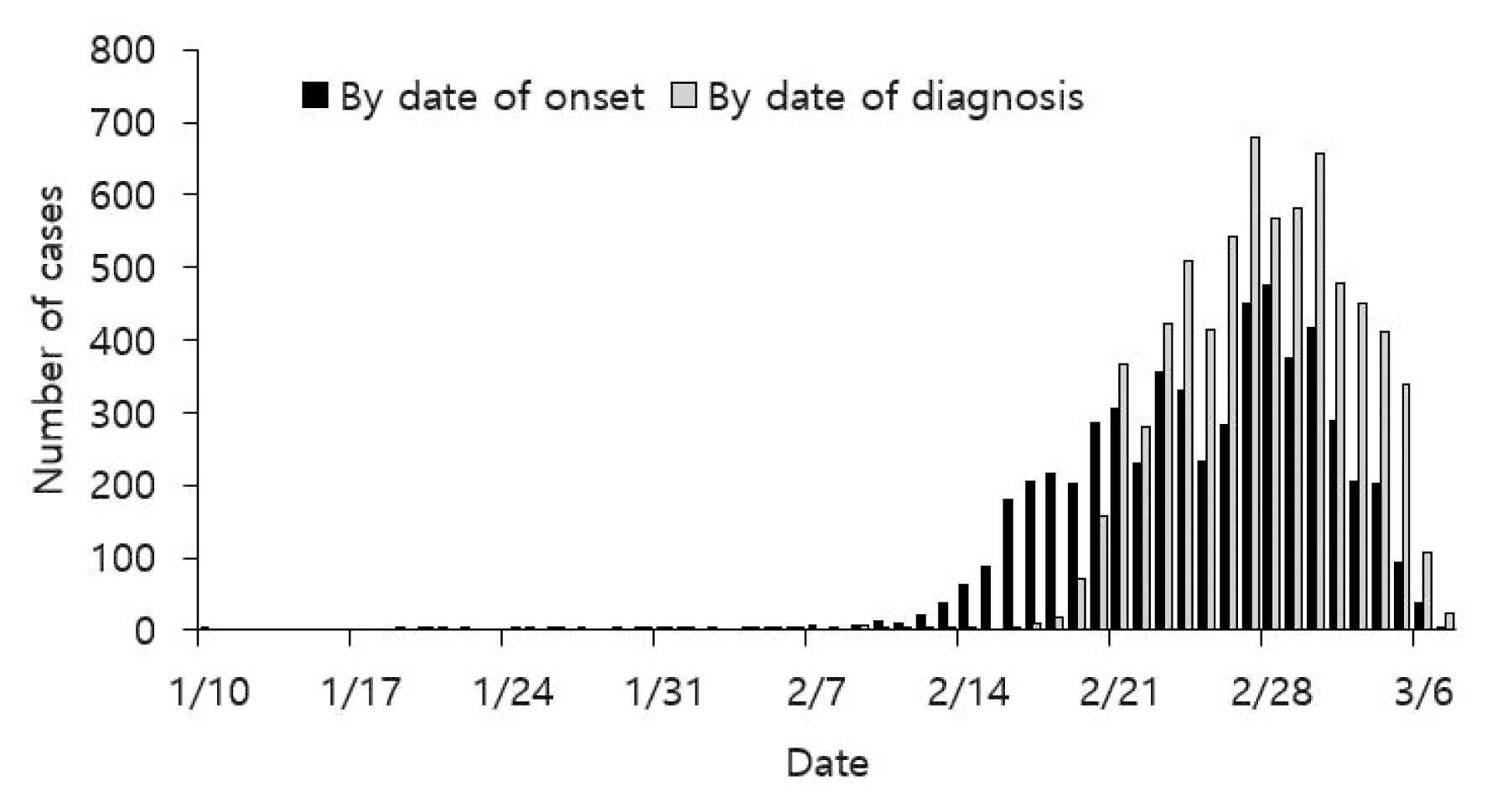
Epidemic curve of laboratory-confirmed coronavirus disease-19 by date of symptom onset and by date of diagnosis, as of March 7, 2020, Republic of Korea.
Provisional data for date of symptom onset.

Epidemic curve of laboratory-confirmed coronavirus disease-19 cases by date of symptom onset, as of March 7, 2020, Republic of Korea.
Provisional data for date of symptom onset.
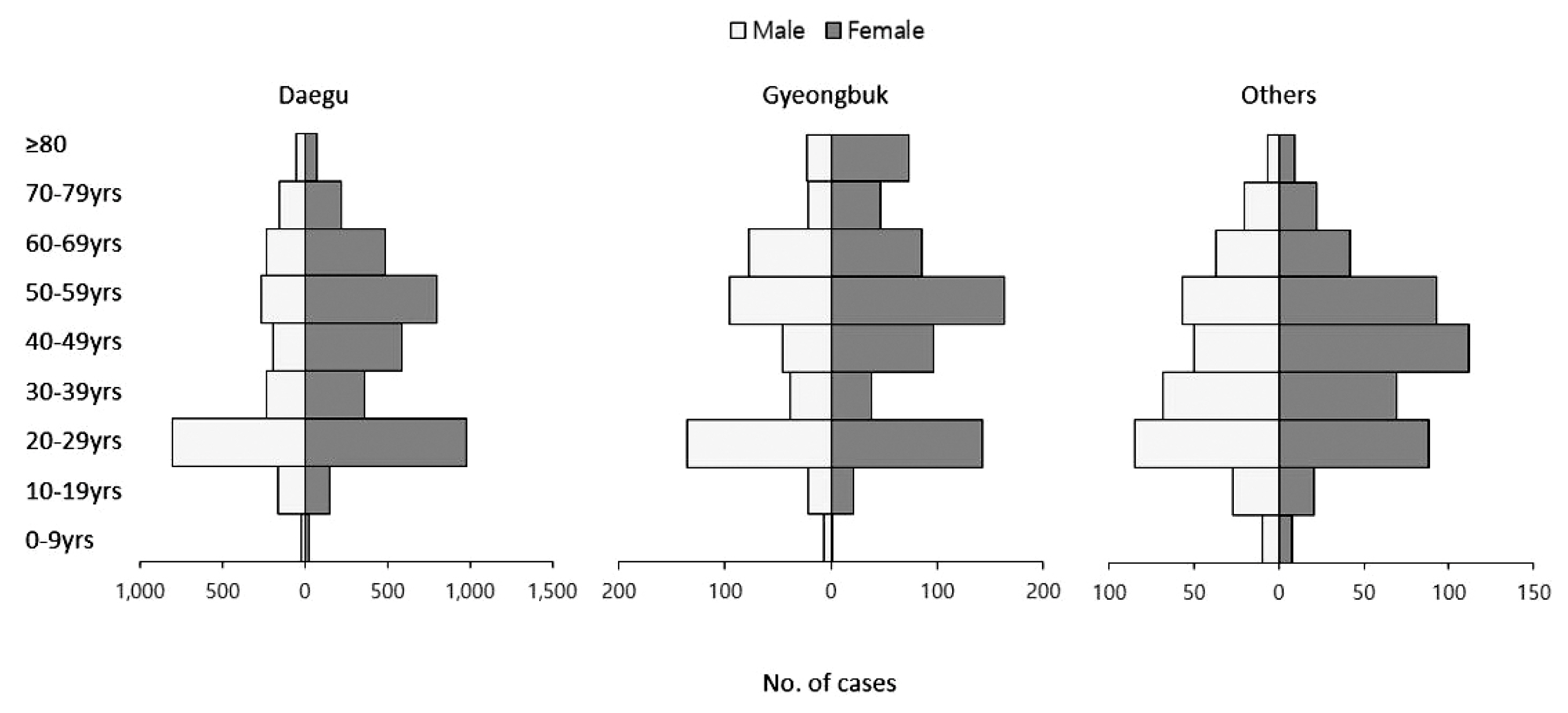
Age distribution and sex ratio of the first 7,755 cases of laboratory-confirmed coronavirus disease-19, as of March 12 2020, Republic of Korea.
Fatal cases of COVID-19 in Korea, as of March 12th, 2020 are shown in Tables 2 and 3. Case fatality proportion was the highest among people aged ≥ 80 years in Daegu, followed by those aged 70–79 years in Daegu, and elderly persons ≥ 80 years old in Gyeongbuk. Overall case fatality proportion in Daegu and Gyeongbuk were 0.8% and 1.4%, which were higher than that in other regions with 0.4%. Figure 4 depicts age-specific epidemic curve stratified as 0–59 years and ≥ 60 years. The outbreak generally began with the younger age group, followed by the elderly population.

Number of deaths and case fatality proportion for laboratory-confirmed COVID-19 cases by geographic region, as of March 12th 2020, Republic of Korea.
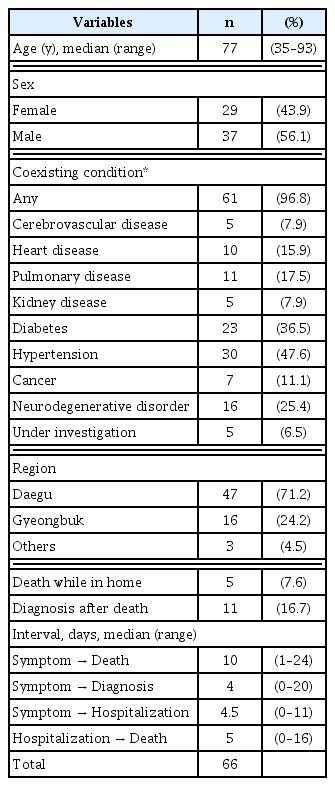
Fatal cases (n = 66) of laboratory-confirmed COVID -19 cases, as of March 12th 2020, Republic of Korea.
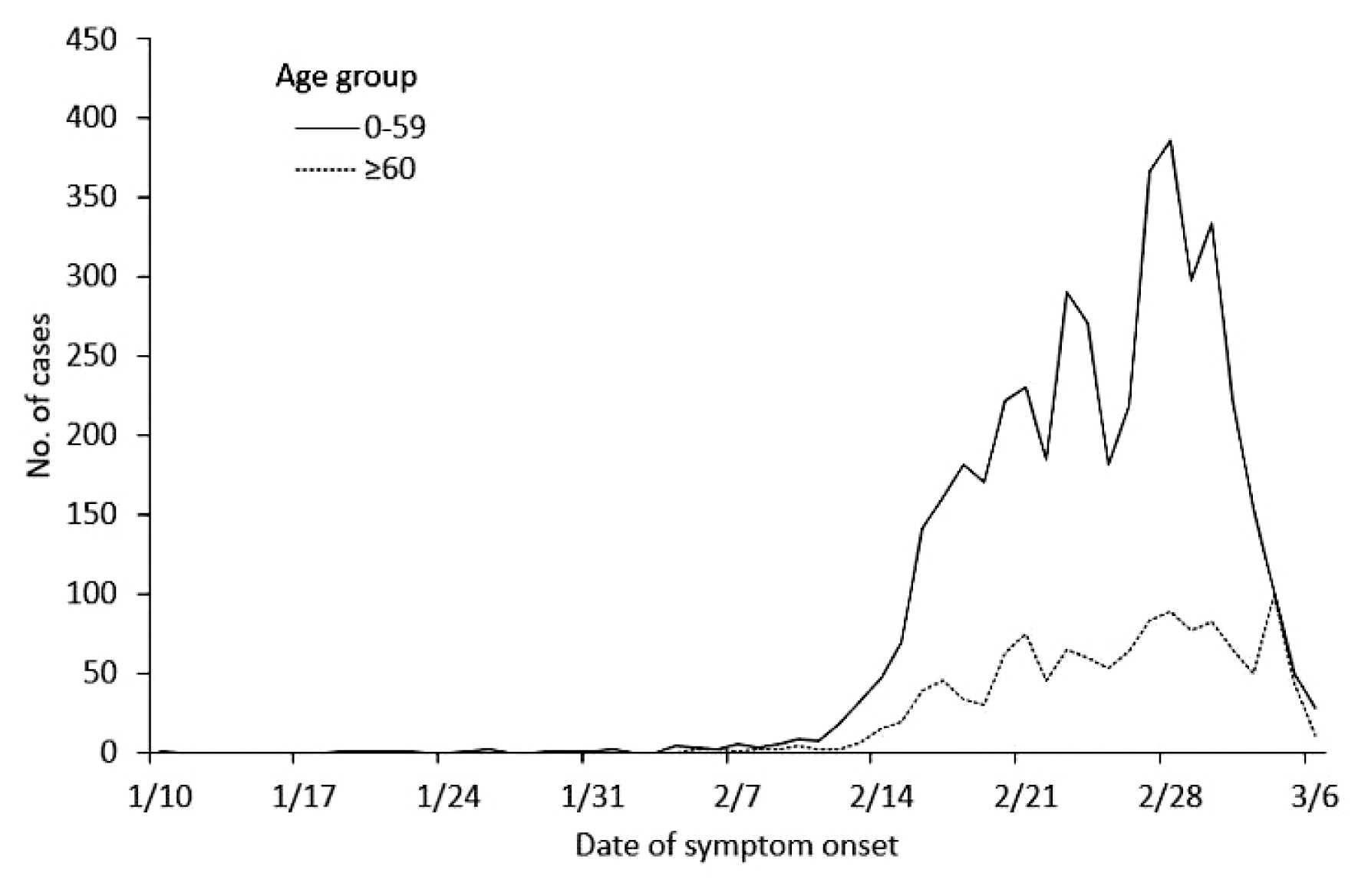
Age-specific epidemic curve of laboratory-confirmed coronavirus disease-19 cases by date of symptom onset, as of March 7, 2020, Republic of Korea.
Provisional data for date of symptom onset.
There were 66 laboratory-confirmed fatal cases of COVID-19, as of March 12th, 2020 (Table 3). The median age was 77 years (range, 35–93 years), and female-to-male ratio of 44:56. Of 63 cases, 96.8% were reported to have comorbidities: 47.6% hypertension, 36.5% diabetes, 16% neurodegenerative disorders, and 17.5% pulmonary diseases. There were 71.2% of fatal cases in Daegu and 24.2% were from Gyeongbuk. There were 5 patients who succumbed to death at home, and COVID-19 was identified as the cause of death in 11 individuals after their death. The median interval between onset of symptoms and death was 10 days (range 1–24 days), while the median interval between date of hospitalization and date of death was 5 days (range 0–16 days).
Discussion
The analysis of the first 7,755 cases of COVID-19 in Korea showed an initial increase in cases in specific geographical regions, comparable to the epidemiological situation in China and Italy [4,5]. In Korea, despite a sharp decline in the number of confirmed cases reported, there were still a relevant number of confirmed cases per week in late February and early March. With descriptive analysis of interim surveillance data, the data suggest that the patient outcome differed markedly between the geographic regions, highlighting the magnitude of surge of cases and access to hospitalization. The difference in age distribution of COVID-19 cases compared with China may reflect active surveillance of a cluster of religious groups tied to the outbreak.
A summary of the epidemiological characteristics of the first 7,755 COVID-19 cases in Korea confirms the contagiousness of COVID-19 that led to a nationwide outbreak in a few weeks. Triaging patients for hospitalization, social distancing (to reduce the number of contacts), and reporting the outbreak amongst vulnerable people in the population may have played a role in the recent decline in cases of COVID-19. However, in the initial response to COVID-19, quarantine, early detection, and isolation of suspected cases of COVID-19, may have contributed to lowering the wave of this epidemic in other parts of Korea. More severe cases were reported in the elderly with existing comorbidities, which warrants clear triage management and a high-risk approach in healthcare access prioritization. COVID-19 does not appear to be fatal among young adults and children, however their role in disease transmission should be further assessed.
This summary may help in the understanding of early phase disease dynamics for the COVID-19 outbreak, and guide future public health measures in other countries.
Acknowledgments
We thank the relevant ministries, including the Ministry of Interior and Safety, Si/Do and Si/Gun/Gu, medical staffs in health centers, and medical facilities for their efforts in responding to the COVID-19 outbreak.
Notes
Conflicts of Interest
The authors have no conflicts of interest to declare.
COVID-19 National Emergency Response Center, Epidemiology and Case Management Team
Korea Centers for Disease Control and Prevention (KCDC):
Eun Kyeong Jeong
Center for Disease Prevention, KCDC: Ok Park, Young Joon Park, Shin Young Park, Young-Man Kim, Jieun Kim, Joongho Jo, Jungwoo Kim, Taeyoung Kim, Sanghui Kweon, Yeonhee Woo, Minwoo Yum, Eunyoung Kim
Center for Public Health Emergency Preparedness and Response, KCDC: Jin Gwack, Jin Lee, Eunmi Park, Seong Sun Kim, Junghee Hyun, Boyeong Ryu, Yoon Suk Jang, Hwami Kim, Yeowon Jin, Hyeyoung Lee, Sangeun Lee, Seung Hwan Shin, Seung Woo Choi, Daehyeon Ko, Seonju Yi, Hee Kyoung Kim
Center for Infectious Disease Control, KCDC: Dongwook Kim, Byoung-Hak Jeon, Miyoung Kim, Si won Choi
Center for Genome Science, KCDC: Jung Hyun Lee, Jae Kyung Park
Bureau of Health Policy, Ministry of Health and Welfare:
Unna Kim
Department of Social and Preventive Medicine, Hallym University College of Medicine: Young June Choe