Health Problems Among Workers Who Recycle Electronic Waste in Southern Thailand
Article information
Abstract
Objectives
This study evaluated the prevalence of adverse health effects among recycling facility workers, and described their socioeconomic situation, health symptoms and work characteristics.
Methods
A cross-sectional study was conducted by interviewing 71 workers in 20 electronic waste (e-waste) recycling facilities in southern Thailand. Data were collected by questionnaire. Risk factors were evaluated using multiple logistic regression analysis.
Results
Recycling facility workers with blurred vision were significantly associated with being male (p = 0.035), over 40 years old (p = 0.020), and having ≤ secondary school education (p = 0.017). Rash/itching was associated with being male (p = 0.011), over 40 years (p = 0.018), having ≤ secondary school education (p = 0.012). not using a cloth mask (p = 0.019), not using gloves (p = 0.028), not washing hands before lunch (p = 0.005), not cleaning clothes daily (p = 0.025), and not having established ventilation systems in the place of work (p = 0.018). Hand-and-feet numbness were associated with being male (p = 0.025), and being over 40 years (p = 0.023). Headaches were associated with being male (p = 0.028).
Conclusion
Personal hygiene is important for this occupational group, and it should be emphasized in education programs.
Introduction
Electronic and electrical waste (e-waste), also referred to as waste electrical and electronic equipment, is defined as any end-of-life “equipment which is dependent on electrical currents or electromagnetic fields in order to work properly” [1]. Today, recycling e-waste has become an important goal worldwide, from the viewpoints of environmental preservation and resource utilization. The opportunities for dismantling these materials make them an interesting business, with the potential for reuse and recycling [2]. In 2016, Asia generated by far the largest amount of e-waste [18.2 metric tons (MT)], followed by Europe (12.3 MT), the Americas (11.3 MT), Africa (2.2 MT) and Oceania (0.7 MT) [3]. As of 2018, e-waste is now the fastest-growing waste stream in the world, with an estimated 48.5 million tons. E-waste components include many toxic substances, such as lead, cadmium, chromium, brominated flame retardants, polychlorinated biphenyls (PCBs) [4]. The e-waste environmental impact from these toxic substances can accumulate in soil, water and food sources. Once in the environment, they persist for long periods of time, a factor that increases exposure risk [4,5]. The health effects of e-waste exposure include respiratory problems, skin disorders, acute brain damage, stroke, asthma, coughing, bronchitis, reduced lung development, and high blood pressure [6].
In the current situation, high-volume informal recycling, which occurs in China [7], Ghana [8], Nigeria [9], India [10], Malaysia [11], the Philippines [12] and Vietnam [13], involves untrained workers performing dangerous procedures without personal protective equipment (PPE) [6].
In Thailand, Decharat [14], reported that the majority of informal e-waste recyclers did not use PPE to protect themselves from lead, cadmium [15], mercury [14] and other dangerous toxins which are released by processing e-waste. The typical self-reported symptoms included insomnia, muscle atrophy, weakness, and headaches [14–16]. Sorach [17] reported that 72.46% of people in the community where e-waste recycling occurred, were concerned about their health. In studies performed by Manomaivibool and Vassanadumrongdee [18,19] where e-waste recycling was occurring, it has been reported that the health of 31.02% of people in those communities, was adversely affected. E-waste separation and recycling operations lead to toxic material release which affects the workers’ health, as well as vulnerable members of the population (children and family members) [3]. Given the hazards of e-waste recycling, this study aimed to evaluate the prevalence of e-waste recycling exposure-related health effects among e-waste workers, and describe their socioeconomic situation and work characteristics.
Materials and Methods
1. Study population and samples
The Ethics Committee of the Institute of Research and Development, Thaksin University, approved this research. This cross-sectional descriptive study was conducted in workers from 20 e-waste recycling facilities in southern Thailand, between July and October 2016 using purposive sampling. Five factories located in Nakhon Si Thammarat Province, 5 in Trang province, 7 in Phatthalung Province, and 3 in Songkhla Province were sampled. The participant workers were recruited by purposive selection. Twenty-five % (71) of all the workers (284) at these 20-e-waste recycling agreed to participate in the study. Inclusion criteria for the participants were being 18–60 years old and in occupational contact with e-waste recycling for at least 1 year. Cooperative letters and informed verbal consent were obtained from all study participants.
2. Sample collection
A questionnaire was used to measure acute and chronic health effects, and PPE. Five experts approved the validity of this instrument. The content of this instrument had a validity score of 0.88 and a Kuder-Richardson 20 (KR-20) reliability score > 0.97. The questionnaire was conducted via face-to-face interview. Information on the following variables was collected: general information (gender and age), worker characteristics (duration of work in contact with e-waste, days worked per week) and personal hygiene behavior (PPE used, consumption of food and/or beverages in the work area, whether hands were washed before lunch, and whether clothes were changed after work). Respondents were asked about the practices that they performed, and the frequency of those activities which were categorized into “sometimes” or “always”, “yes” or “no.”
The occurrence of acute and chronic health effects amongst the workers was also observed. Acute effects included headache, blurred vision, nausea and vomiting, rash or itching, increased sweating, tight chest, palpitations, and hand-and-feet numbness. Chronic effects included stomach ache, weight reduction, constipation, lack of stability, permeation, convulsion, and coughing. The acute effects were noted either during the initial study time or during a 1-month recall period. The chronic effects were noted after a 6-month recall period. Information was also collected by self-reported complaints, and doctors’ diagnoses. Respondents were asked about the occurrence of each adverse health effect and were required to reply with “yes” or “no.”
3. Statistical analysis
Data were collected by questionnaire and analyzed using a software program. For descriptive statistics, percentages and frequency values were computed for the variables. Risk factors were evaluated using multiple logistic regression analysis. Adjusted odds ratio (ORadj) and 95% confidence interval (95% CI) were presented as statistically significant when the p value was < 0.05.
Results
1. Demographic characteristics
The study participants consisted of 71 workers (51 male and 20 female workers) in e-waste recycling facilities in Southern Thailand. More than half of the workers were > 40 years old (57.7%). The largest group had less than a secondary-school-level education (64.8%). The participants consisted of 32 smokers (45.1%), 39 non-smokers (54.9%), and 38 participants (53.5%) disclosed they consumed 2 units of alcohol per week.
The majority (62.0%) of all participants worked less than 8 hours per day, and 56.3% had worked in contact with e-waste for < 10 years. Most participants (60.6%) used masks (cloth masks), and 69.0% used gloves when handling e-waste. Almost all participants (95.8%) washed their hands before lunch. There were 71.8% of workers who ate lunch in the working areas, and 87.3% of all participants worked in clean clothes every day. There were 56.3% of all working areas that did not have established ventilation systems (Table 1).
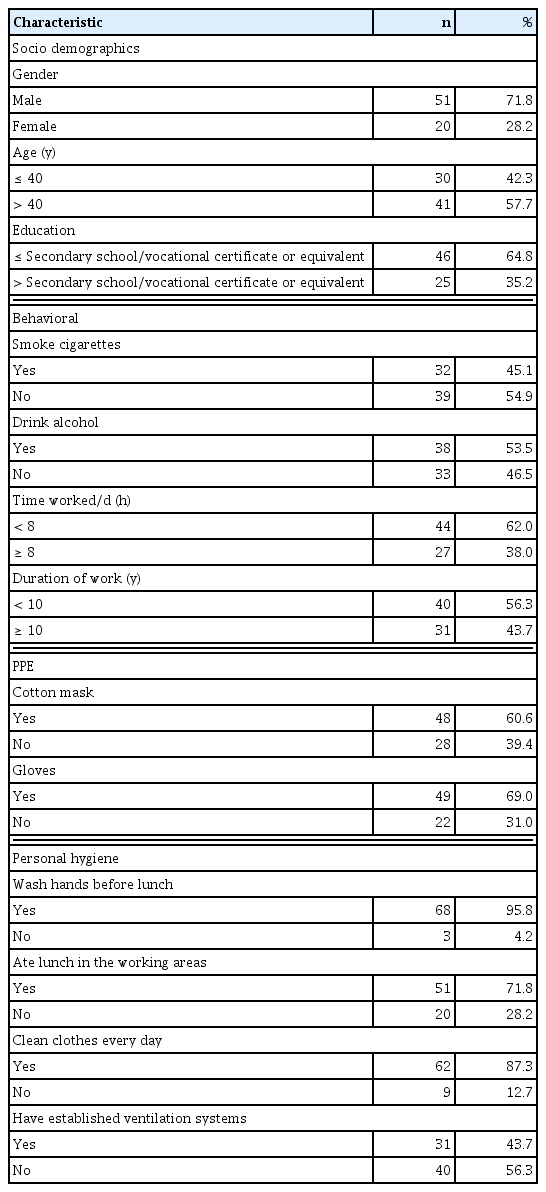
Demographics of workers in E-waste recycling (n = 71).
2. Prevalence of health symptoms among the participants
The prevalence of self-reported acute effects in the preceding 1 month are shown in Table 2. The prevalence of blurred vision (26.8%), rash or itching (26.8%), hand-and-feet numbness (25.4%) and headaches (23.9%) was notable in the sample. The relationship between these symptoms above, are shown for different sociodemographic independent variables, including gender, age, education level, smoking status, alcohol consumption, hours worked per day, duration of working in contact with e-waste, use of PPE and personal hygiene in Tables 3 and 4.
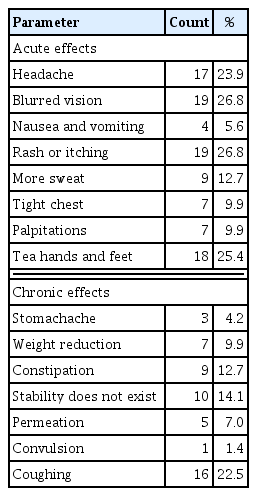
Prevalence (%) of health symptoms in workers during the previous month that work in e-waste recycling (n = 71).
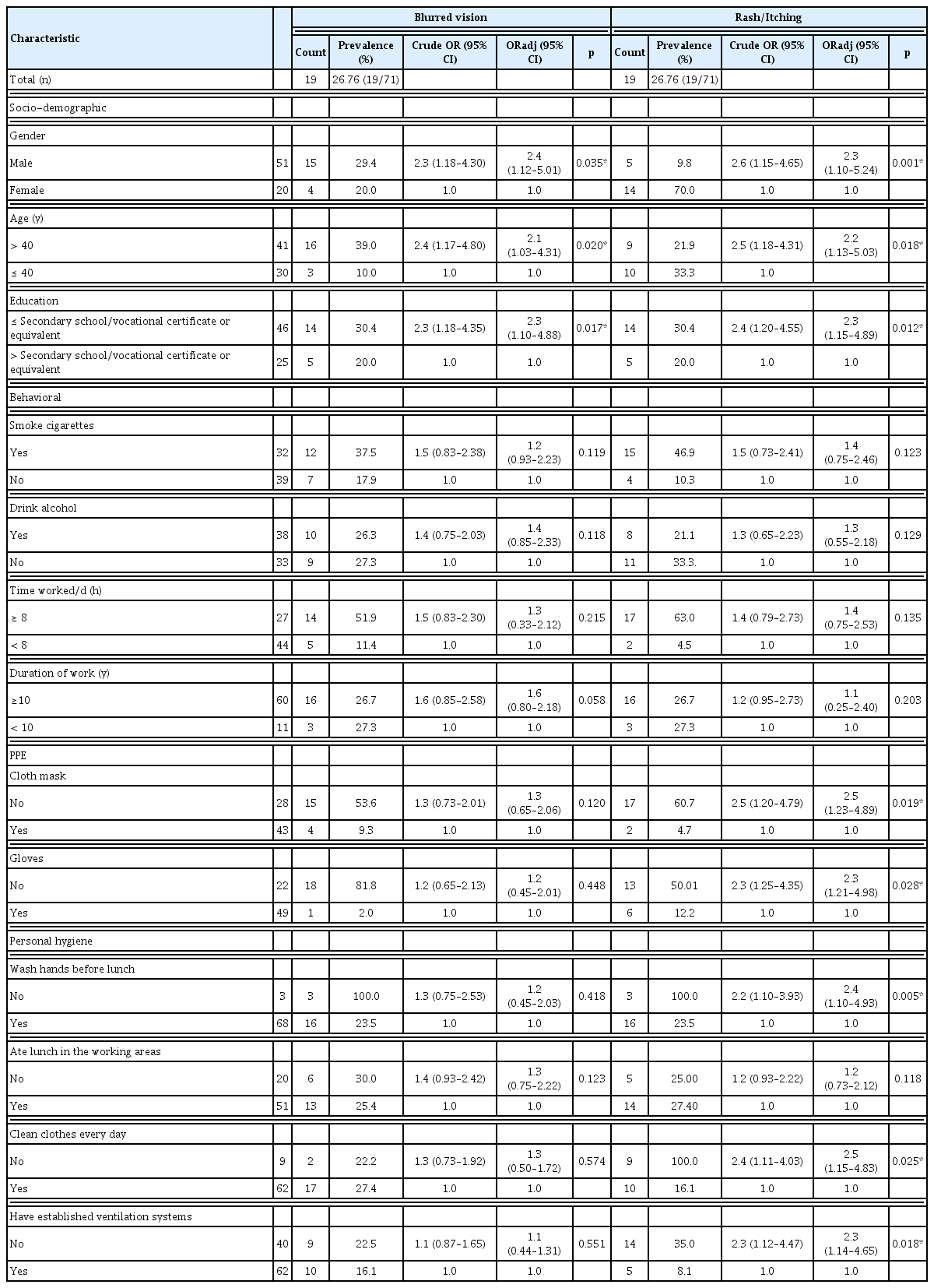
Prevalence of blurred vision and rash/itching symptoms in the previous month, according to participant characteristics.

Prevalence of hand-and-feet numbness and headaches in the previous month, according to participant characteristics.
The univariate analysis showed that statistically significant risk factors which were related to blurred vision amongst participants were being male (OR = 2.3; 95% CI =1.18–4.30), aged > 40 years (OR = 2.4; 95% CI = 1.17–4.80), and having an education ≤ secondary school/vocational certificate or equivalent (OR = 2.3; 95% CI = 1.18–4.35). Statistically significant risk factors related to rash/itching amongst participants were being female (OR = 2.6; 95% CI =1.15–4.65), aged ≤ 40 years (OR = 2.5; 95% CI = 1.18–4.31), having an education ≤ secondary school/vocational certificate or equivalent (OR = 2.4; 95% CI = 1.20–4.55), not using a cloth mask (OR = 2.5; 95% CI =1.20–4.79), not using gloves (OR = 2.3; 95% CI = 1.25–4.35), not washing hands before lunch (OR = 2.2; 95% CI =1.10–3.93), not wearing clean clothes every day (OR = 2.4; 95% CI = 1.11–4.03), and working in areas where ventilation systems were not established (OR = 2.3; 95% CI = 1.12–4.47).
The risk factors related to hand-and-feet numbness were being male (OR = 2.2; 95% CI = 1.10–4.10), and aged > 40 years (OR = 2.3; 95% CI = 1.13–4.28). The risk factor related to headaches was being male (OR = 2.4; 95% CI = 1.10–4.20).
The analysis of multiple variable logistic regression controlling for age, gender, and work experience variables, showed that statistically significant risk factors related to blurred vision amongst participants were being male (ORadj = 2.4; 95% CI = 1.12–5.01), aged > 40 years (ORadj = 2.1; 95% CI = 1.03–4.31), and having an education ≤ secondary school/vocational certificate or equivalent (ORadj = 2.3; 95% CI = 1.10–4.88).
For risk factors related to rash/itching amongst participants were being male (ORadj = 2.3; 95% CI = 1.10–5.00), aged > 40 years (ORadj = 2.2; 95% CI = 1.13–5.03), having an education ≤ secondary school/vocational certificate or equivalent (ORadj = 2.3; 95% CI =1.15–4.89), not using a cloth mask (ORadj = 2.5; 95% CI =1.23–4.89), not using gloves (ORadj = 2.3; 95% CI = 1.21–4.98), not washing hands before lunch (ORadj = 2.4; 95% CI = 1.10–4.93), not wearing clean clothes every day (ORadj = 2.5; 95% CI = 1.15–4.83), and not having an established ventilation system in the place of work (ORadj = 2.3; 95% CI = 1.14–4.63).
The risk factors related to hand-and-feet numbness were being male (ORadj = 2.3; 95% CI =1.12–4.50), and aged > 40 years (ORadj = 2.3; 95% CI =1.10–4.57).
The risk factor related to headaches was being male (OR = 2.4; 95% CI =1.12–4.40).
Discussion
In this study, blurred vision occurred in 26.8% of e-waste recycling workers. This result supports previous findings [20,21], which reported the effects of heavy metal (lead, cadmium and manganese) intoxication on eyesight. In addition, mercury has been reported to be significantly associated with dry eye disease [22]. Blurred vision can also be a symptom of more serious problems, including potentially sight-threatening eye diseases or neurological disorders. In this study, e-waste was observed to be recycled by casual labor recyclers, using low-tech methods such as manual dismantling, open burning and acid leaching, in order to recover gold, copper and other valuable metals. These methods generate subsistence livelihoods for workers, but also result in significant hazards to human health and the environment due to the toxic materials that are released from consumer electronics. Certain chemicals in the e- waste recycling processes can cause very serious burns inside the workers eyes causing irritation and damage. Among the most dangerous chemicals are alkalis, such as oven or drain cleaners, and fertilizers. They attack the tissues of the eye very quickly and cause damage or irritation to eye. During smelting, leaching, and other extraction processes used for the target metals, it was observed that the workers in e-waste recycling often do not wear masks or adequate protective clothing. In addition, often there are no emission control devices or emission filters being used, and hence they are exposed to toxic fumes and solvents that continuously endanger their health.
The prevalence of the skin diseases [23], namely rashes or itching, occurred in 26.8% of participants in this study. The Agency for Toxic Substances and Disease Registry [24] reported that symptoms of the skin including rashes, itching, redness and peeling from the hands, nose and soles of the feet, all of which can elicit allergies and dermatitis [25,26]. Additionally, Qiu et al [27] presented studies in the e-waste remanufacturing industry in Guiyu, China, where the residents had a high incidence of skin damage, headaches, vertigo, nausea, chronic gastritis, and gastric and duodenal ulcers [28,29].
There were also some neurological symptoms exhibited among the e-waste workers. There were 25.4% of the participants who reported hand-and-feet numbness. Symptoms usually include numbness and paresthesia in the peripheral polyneuropathies which is associated with exposure to heavy metals, drugs, infections and hereditary diseases [30]. The prevalence of headaches (23.9%) observed in participants, could be due to chronic poisoning when exposed to a chronic low dose of toxicants in the e-waste materials [31]. This result is supported by Jaishankar et al [32], who reported sources, and toxicological effects of some heavy metals in people. Several metals and metallic compounds act as neurotics and may cause impairments of the nervous system. These include arsenic (As), cadmium (Cd), mercury (Hg), lithium (Li), lead (Pb), and thallium (Tl). Other compounds, such as cobalt (Co), chromium (Cr), copper (Cu), lithium (Li), and nickel (Ni), are known to act as skin and eye irritants or as allergens. The inhalation of arsenic (As), beryllium (Be), cadmium (Cd), obalt (Co), chromium (Cr), and nickel (Ni) provokes the formation of pulmonary diseases affecting the respiratory system [26].
With regards to gender, males exhibited significantly more acute symptoms, including blurred vision, hand-and-feet numbness and headaches, than females. The majority of the participants in this study were male, and thus they were potentially at higher risk when compared to female participants. However, rash/itching was shown in more female compared to male participants. This result is supported by a previous study which reported gender differences in itch- and pain-related sensations [33]. The higher incidence of adverse symptoms in male workers may be indicative of differences in the types of labor performed in the facility compared with women.
In this current study age > 40 years was statistically significantly associated with the prevalence of blurred vision, rash/itching and hand-and-feet numbness. This result is similar to a previous study that reported that urinary 8-hydroxydeoxyguanosine levels are positively associated with heavy metal exposure, physical activity and age [34]. However, headaches were more prevalent in participants < 40 years old. A previous study that used age-stratified analysis showed that a higher concentration of lead in the blood was associated with a higher risk of asthma in younger individuals whilst active [35].
A lower education level was statistically significantly associated with the prevalence of blurred vision and rash/itching. Edith et al [36] reported that knowledge, perceptions and practices in relation to health risks were associated with exposure to e-waste recycling in participants at Agbogbloshie e-waste recycling and dump site in Accra, Ghana. Furthermore, Asampong et al [37] reported the finding that a lower level of education was likely to influence perceptions about the necessity of PPE and protective behaviors. This data highlighted the need for health education to improve workers’ health-seeking practices.
The prevalence of acute health symptoms was statistically significantly associated with appropriate personal hygiene and use of PPE used among the participants. Workers who engaged in hazardous techniques including cutting, acid baths, heating/smelting and open burning of materials, often performed them without PPE or engineering controls [38,39]. In this current study, cloth masks were used by workers recycling e-waste (60.6%), but the type of masks used were inappropriate for this type of work. Cloth masks do not protect the workers from pollution, just from dust. In addition, pollutants such as heavy metals can accumulate on the surface of cloth masks, penetrate the cloth mask and be inhaled. Furthermore, not washing hands before lunch, not wearing clean clothes every day, and not having established ventilation systems in the place of work were statistically significantly associated with the prevalence of rashes or symptoms of itching. Thus, the heavy metals can accumulate and penetrate the body [40]. Moreover, Yohannessen et al [41] reported the prevalence of injuries was high (an average of 3 injuries in the past 6 months), and the PPE use was generally low among Chilean e-waste workers. The conclusion in this study suggests that exposure to e-waste is harmful to the health of e-waste recycling workers. More well-designed epidemiological investigations in fetuses, pregnant women, elderly people and other vulnerable populations, especially pregnant women and children who live in e-waste management areas, are needed to confirm these associations. In addition, policy-level and technical interventions, implementation and capacity building and increasing the public awareness can change this challenge into an opportunity to show the world that Thailand is ready to deal with future problems and can set global credible standards concerning environmental and occupational health.
Acknowledgments
The authors thank the workers in the 20 e-waste recycling facilities in Nakhon Si Thammarat Province, 5 factories in Trang province, 7 factories in Phatthalung Province and 3 factories in Songkhla Province. The authors also thank the Institute of Research and Development, Thaksin University, who supported this research.
Notes
Conflicts of Interest
No potential conflicts of interest relevant to this article was reported.