Study on Cardiopulmonary Function, Maximal Oxygen Uptake, and Obesity Index according to Smoking Status in Middle-Aged and Older Office Workers
Article information
Abstract
Objectives
To investigate the effect of smoking upon cardiopulmonary function, maximal oxygen uptake, and obesity index, in middle-aged and older workers to propose guidelines on healthcare for these age groups.
Methods
This study analyzed medical data from 2,753 white-collar workers aged 50 years or older from workplaces located in Seoul, South Korea. Blood pressure (BP), resting heart rate, maximal oxygen uptake (VO2max), and body mass index (BMI) of each subject were measured. The collected data were analyzed using SPSS 21.0.
Results
In the smoking group BP and resting heart rate were significantly higher than in the non-smoking and smoking-cessation groups (p < 0.05). In addition, VO2max was lower in the smoking group compared to the other 2 groups. BP closely correlated with resting heart rate, abdominal fat ratio, and BMI. BMI was the highest in the group that stopped smoking and, BMI and abdominal fat ratio negatively correlated with VO2max.
Conclusion
Smoking increases the risk of cardiopulmonary disease but obesity may be caused by stopping smoking. Therefore, healthcare guidelines on smoking cessation should also include nutritional advice.
Introduction
Population aging is becoming a serious concern worldwide due to the increasing demand on healthcare costs. In 2000, 7% of the population of South Korea was elderly (aged 65 years and older), and this is expected to reach 14.3% in 2018, and 20.8% by 2026, which will make South Korea a super-aged society [1]. South Korea is aging at the fastest rate amongst all the countries in the Organization for Economic Cooperation and Development [2]. Of concern, aging may cause many social and economic problems but one of the most prominent concerns related to aging is the increased working-age of the population. Generally, the generation aged between 25 to 49 years old is the most economically active in a society. However, numbers of this age group in South Korea are predicted to decrease from 59.6% in 2006 to 45.2% by 2050. It is also predicted that the population aged between 50 to 64 years will increase from 20.5% to 40.5% in the same period [3]. As the aging of workers increases, it may lead to a decline in productivity and an increase in medical expenses, which will be a considerable burden for the workers and the nation. Companies tend to offer older workers early retirement but this approach does not always solve the problem [4]. Increasing the productivity of middle-aged and older workers by promoting healthy living will be an important challenge for Korea and all countries [5]. Health policies for workers are shifting from dealing with accidents, such as industrial accidents or exposure to harmful substances, to health promotion policies that are closely related to daily life, such as smoking, drinking, and physical activities [6]. Generally, health risk behaviors amongst middle-aged and older workers are highly likely to have persisted for a long period of time, and are associated with more serious problems, such as physical disabilities in older age, depressive symptoms, and mortality, as well as decreased productivity [7]. In particular, smoking as a habit with well-known risk factors for various preventable and life-threatening diseases. In South Korea, the prevalence of premature death attributable to smoking was reported to be 57.7% in males and 11.4% in females annually [8]. Cigarette smoking is associated with an increased risk of cancer [9], cardiovascular and digestive diseases as well as lung diseases. Hypertension and obesity are typical factors that can cause disease by smoking and should be managed in middle-aged people to avoid the risk of a stroke. VO2max is the most significant fitness factor related to health promotion and is closely associated with lifestyle-related diseases [10].
This study investigated whether there were correlations between smoking status, cardiopulmonary function, obesity index, and VO2max in middle-aged and older workers.
Materials and Methods
1. Participants
The present study was conducted in 2,753 white-collar workers who volunteered to participate, were aged 50 years and above, and worked in Seoul, South Korea. Researchers collected general information and measured BP, heart rate, VO2max, BMI, and basal metabolic rate. Smoking status was divided into: smoking, non-smoking, and smoking cessation (a state of previously smoking but currently non-smoking). There were 2,284 males and 469 female participants. The mean age in the smoking group was 53.35 ± 3.37 years, 53.01 ± 3.05 years in the non-smoking group, and 53.12 ± 3.09 years in the smoking cessation group.
2. Measurements
The BP was measured twice in the right upper arm by mercury sphygmomanometer after allowing each participant to rest for more than 10 minutes; the mean value was used as the BP level of each participant. The cutoff points for BP were divided into systolic BP ≤ 120 mmHg (normal), 120–139 mmHg (pre-hypertension), and ≥ 140 mmHg (hypertension); and diastolic BP ≤ 80 mmHg (normal), 80–89 mmHg (pre-hypertension), and ≥ 90 mmHg (hypertension).
The resting heart rate was measured after each participant had rested for more than 10 minutes by counting the number of heart beats in 15 seconds and multiplying by 4.
The VO2max was measured using the Bruce Protocol where the speed and inclination of the treadmill was elevated at 3-minute intervals to increase workload. The test was performed until each subject reached maximal heart rate or maximal rating of perceived exertion [11].
The BMI, as calculated using body weight (kg)/height (m2). The cut-off points for BMI were divided into ≤ 18.5 (low-weight), 18.5–22.9 (normal weight), 23.0–24.9 (over-weight), and ≥ 25.0 (obese).
The abdominal fat ratio was measured using the bioelectrical impedance fatness analysis (GIF-891DX). The measuring postures allow the legs to spread on the bed. The electrode should be rubbed sufficiently with alcohol cotton on the back of the hand and the foot, then apply the electrode gel to the skin. The body fat percentage is determined by the value indicated from the estimation formula embedded in the measuring instrument. Abdominal fat ratio could be said to be very serious when the male is over 0.95 and the female is over 0.85.
3. Statistical analysis
Data was analyzed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). Comparisons of mean values of cardiopulmonary function, obesity index, and VO2max according to participants’ smoking status were tested using ANOVA, and the post-hoc test was performed using the Scheffe test. The distribution of cardiopulmonary, obesity index, and VO2max according to smoking status was tested using the chi-square test. Pearson’s correlation coefficients were used to investigate the correlations between the elements. Statistical significance was accepted for p < 0.05.
Results
1. Comparisons of cardiopulmonary function, maximal oxygen uptake, and obesity index according to smoking status
The smoking, non-smoking, and smoking cessation groups had 782 (28.4%), 1,222 (44.4%), and 749 (27.2%) participants, respectively. There was no statistically significant difference between the ages of the subjects in each group. The systolic BP and diastolic BP levels were significantly higher in the smoking group than in the non-smoking and smoking cessation groups (p < 0.01), as was the heart rate (p < 0.001; Table 1). VO2max was the highest in the non-smoking group, followed by the smoking cessation and smoking groups (p < 0.001; Table 1). No significant difference was found in the abdominal fat ratio between the groups, however, BMI was significantly greater in the smoking cessation group (p < 0.05; Table 1).

Comparisons of cardiopulmonary function, maximal oxygen uptake, and obesity index according to smoking status (n = 2,753).
2. Distribution of cardiopulmonary function, obesity index, and maximal oxygen uptake according to smoking status
Subjects in the non-smoking group were most likely to have a lower systolic BP of ≤ 120 mmHg, whereas in the smoking group, a BP of ≥ 120 mmHg was most prevalent (p < 0.001). Those participants with a diastolic BP of ≤ 80 mmHg were the most prevalent in the smoking cessation group, and those with a diastolic BP of ≥ 80 mmHg were most likely to be in the smoking group (p < 0.05; Table 2). The proportion of participants with an abdominal fat ratio of ≥ 0.95 (severe abdominal fat), was the highest in the smoking cessation group (p < 0.01) and the number of those with a BMI of ≥ 25.0 (obese subjects), was the highest in the non-smoking group, but it was not statistically significant (Table 2). The proportion of those with a VO2max of ≥ 31 was the highest in the non-smoking group (p < 0.001) compared to the other 2 groups, and the number of those with a resting heat rate of ≥ 81 bpm was the highest in the smoking group (p < 0.001; Table 2).
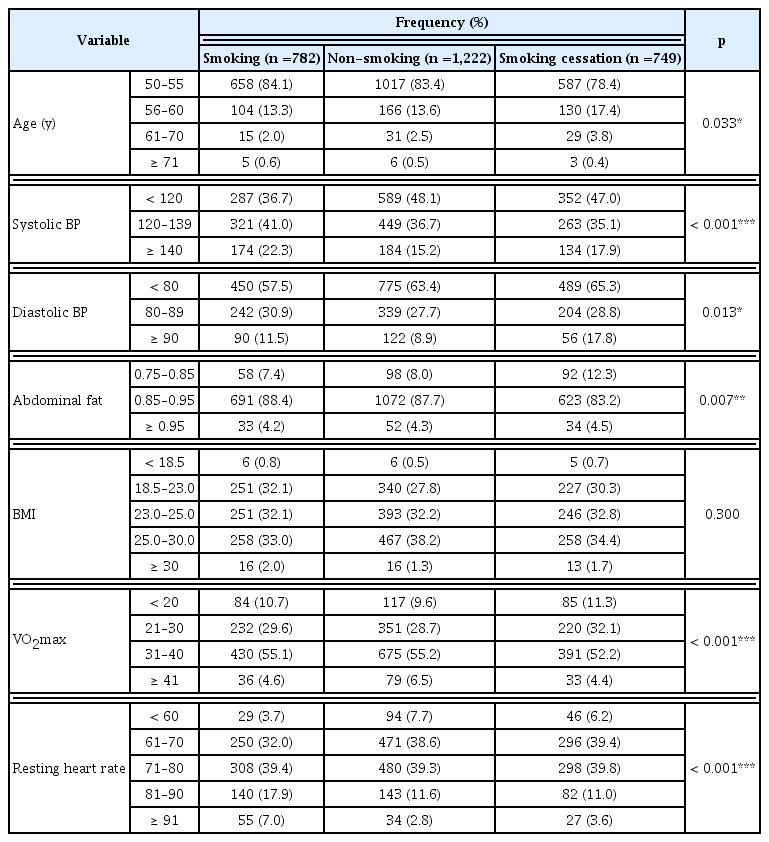
Distribution of cardiopulmonary function, obesity index, and maximal oxygen uptake according to smoking status (n =2,753).
3. Correlations between the cardiopulmonary function, obesity index, and VO2max and smoking status
Systolic and diastolic BP levels were significantly correlated with cardiopulmonary dysfunction and high BMI, except for VO2max (p < 0.001; Table 3). Resting heart rate was correlated with age (r = −0.043, p < 0.05), systolic BP (r = 0.228, p < 0.001), and diastolic BP (r = 0.209, p < 0.001; Table 3). VO2max was correlated with abdominal fat ratio (r = −0.087, p < 0.001), and BMI (r = −0.151, p < 0.001; Table 3). Abdominal fat ratio was correlated with age (r = 0.068, p < 0.001), systolic BP (r = 0.254, p < 0.001), diastolic BP (r = 0.227, p < 0.001), VO2max (r = −0.087, p < 0.001), and BMI (r = 0.823, p < 0.001; Table 3). BMI was correlated with systolic BP (r = 0.223, p < 0.001), diastolic BP (r = 0.195, p < 0.001), VO2max (r = −0.151, p < 0.001), and abdominal fat ratio (r = 0.823, p < 0.001; Table 3).

Correlations between the elements measured.
Discussion
The present study investigated the effect of smoking status upon, cardiopulmonary function, obesity, and VO2max in middle-aged and older workers, with the aim of providing health management guidelines to these workers.
The general characteristics of the participants revealed that over 80% were male. The mean age of those in the smoking, smoking cessation, and non-smoking groups was similar, showing no statistically significant difference. The results showed that systolic BP and diastolic BP were significantly highest in the smoking group. Previous studies have shown that BP is higher in the smoking group than in the non-smoking or smoking cessation group [9,12]. In contrast, Kushima et al. [13] reported no difference in BP between smokers and non-smokers. In the past it was thought that smoking itself was deemed to have no effect on BP, as other physical functions may have more effects on BP [12]. However, a recent study on nicotine reported that BP rises for the duration that nicotine remains in the body, and if this phenomenon persists, people are exposed to the risk of cardiovascular disease due to hypertension [14]. It has been suggested that when smoking is stopped, BP is temporarily lowered; and it is necessary to have stopped smoking for more than a month to maintain this BP lowering effect. The resting heart rate was found to be significantly highest in the smoking group, and the proportion of those with a resting heart rate of ≥ 81 was the highest in the smoking group. Several studies have revealed that an increased heart rate during rest is associated with an increased risk of heart disease [15,16]. The result of the present study showed that resting heart rate is high in smokers, suggesting that smoking may be a risk factor for increasing the risk of heart disease.
Furthermore, VO2max was higher in the non-smoking and smoking cessation groups than in the smoking group, in the present study. The number of those with a VO2max of ≥ 31 was also the highest in the non-smoking group indicating that smoking may affect aerobic capacity. This finding supports the promotion of a healthier lifestyle in smokers to encourage them to stop smoking and exercise more [9]. Carbon monoxide inhaled from smoking cigarettes affects aerobic capacity by interfering with oxygen transport, which is thought to be the reason for lowering the VO2max in smokers, but this effect is reversible. In this study the group that had stopped smoking had a significantly higher VO2max than smokers.
The results of this study showed no significant difference in abdominal fat ratio according to smoking status; BMI was the highest in the smoking cessation group. Gordon [17] reported that it is highly likely that body weight increases in the short term after smoking cessation, and then the increased weight will be maintained. Obesity is associated with cardiovascular disease as age increases. Therefore, education on eating habits and nutrition after smoking cessation should be provided.
BP was found to be correlated with cardiopulmonary function, BMI and abdominal fat; BP did not correlate with VO2max. The determinants of VO2max include pulmonary ventilation, oxygen binding capacity of the blood, and cardiac output, however, no previous studies have shown that BP has a direct effect on VO2max. The results of this study showed that BP is closely related with resting heart rate, abdominal fat ratio, and BMI, suggesting that BP and weight management have an effect on the cardiovascular system. In particular, abdominal fat ratio and BMI was found to be negatively correlated with maximal oxygen uptake. Kim et al [18] examined the relationship between VO2max and metabolic syndrome in 185 male and female college students and reported that waist circumference was significantly greater in those with a lower cardiopulmonary fitness than those with a higher cardiopulmonary fitness. Nagano et al [19] investigated the relationship between abdominal fat and VO2max in 200 male and female adults with type 2 diabetes, and demonstrated a correlation between visceral fat and VO2max. This suggests that obesity has a direct effect on cardiopulmonary fitness, and exposes people to the risk of heart disease and diabetes that increases with age. Reduced body fat will increase VO2max, which will reduce the risk of insulin resistance and blood lipids, and is considered to be a good way to prevent cardiovascular disease.
The results of this study can forma health promotion program for industrial health that can be presented to the workers similar to the “Health Plan 2010,” which emphasized a nationwide healthy lifestyle such as non-smoking, moderation in alcohol consumption, exercise and nutrition improvement [20]. To maintain a healthy working environment, group health initiatives to stop smoking and provide nicotine patches. People need to realize what is “a safe amount of alcohol to drink.” Employee exercise clubs need funding and workers need to monitor lifestyle choices in what they choose to eat and whether they choose to walk or use the elevator. Education about dietary habits is really important in particular when people are giving up smoking where possible weight gain may be an issue that requires greater awareness. Weight and smoking status was investigated by Williamson et al [21] during the first National Health and Nutrition Survey conducted between 1971 and 1975 for American adults aged 25 years to 74 years, with a follow up from 1982 to 1984. This study found that out of 748 men and 1,137 women who smoked, 409 men and 359 women tried to stop smoking for more than 1 year, and gained average weight of 2.8 kg and 3.8 kg, respectively. Recognizing that smoking may lead to obesity, and stopping smoking may lead to weight gain, people need to plan and maintain exercise and nutrition management after giving up smoking.
This study had a wide range of subjects: Smoking group, non-smoking group, and smoking cessation group, unlike other studies. This study also showed that weight gain may occur when smoking is stopped. Since this study was carried out on middle-aged and older workers, the results can be used as a guide to take various measures against diseases that occur in elderly workers. The study was also limited to white-collar workers in specific organizations located in Seoul, South Korea and not field workers. Therefore, further studies are needed to expand the scope of subjects to yield a more representative study of the population. Studies on duration of smoking abstinence and lifestyle habits, are also needed. Based on the results of the present study, programs for exercise prescriptions for workers could be developed, and related studies should be conducted in the future.
Notes
Conflicts of Interest
The author has no conflicts of interest to declare.