Epidemiological Aspects of Visceral Leishmaniasis in Larestan and Ghiro-Karzin Counties, Southwest of Iran
Article information
Abstract
Objectives
Leishmania parasites are the causative agents of leishmaniasis. The Visceral leishmaniasis (VL) form of the disease is fatal if not treated in most cases. This study examined the epidemiological aspects of VL in two southwest counties of Iran.
Methods
This was a retrospective study of hospitalized patients with a laboratory confirmation of VL from Larestan and Ghiro-Karzin Counties.
Results
For Larestan county, a decline in the incidence of VL has been observed from 2004 to 2015. Significantly more males (n = 14) than females (n = 6) were infected with VL in this county (p < 0.05), >95% of cases in children under 5 years of age. In Ghiro-Karzin county, the results were similar to a decline in VL infection from 2004 to 2015, and slightly more males (n = 14) than females (n = 11). Similarly, the majority of the patients infected with VL were children under 5 years old (88%).
Conclusion
The results from this study indicate that although the incidence of VL infection has reduced over time, VL was more prevalent in boys under 5 years old, suggesting that more attention to controlling the parasite and its vector are required.
Introduction
Leishmania parasites are the causative agents of leishmaniasis, which has been classified by the World Health Organization as a neglected tropical disease [1] It is considered as one of the most important human parasitic diseases in the world [2]. The most common forms are cutaneous leishmaniasis, which causes skin ulcers, and visceral leishmaniasis (VL), also known as kala-azar, which affects internal organs. Diffuse cutaneous and muco-cutaneous leishmaniasis forms are rare [1,3]. Kala-azar is identified by irregular fever, hepatosplenomegaly, significant weight loss, adenopathy and anemia. If left untreated, the disease can have a fatality rate as high as 95%–100% within 2 years [4]. Leishmaniasis is endemic among 101 countries of the world, including Iran [3]. There are 2 main foci of visceral forms; one occurs in Northwestern Iran, East Azarbaijan (Meshkin Shahr and Ardabil), and the other in the Fars region (Kazeroun, Nourabad, Ghiro- karzin, Firouzabad) [5,6].
VL is caused by Leishmania infantum in Iran and Middle East, whilst in the Indian Subcontinent and Eastern Africa, the disease is caused by Leishmania donovani [5]. Recently, 90% of VL disease was reported in 5 countries, including Bangladesh, India, Sudan, Nepal, and Brazil. According to official reports, 59,000 deaths due to VL were reported annually [7]. The parasitic protozoans are transmitted between hosts by the bite of female phlebotomine sand flies [8]. Its vector in Iran is a species of the genus of Phlebotomus (sand fly) and some of its main reservoir hosts are dogs and other canines [9]. There are approximately 500 identified phlebotomine species, but only about 30 have been found to spread leishmaniasis. Phlebotomine sandflies are found throughout the tropics and sub-tropics, as well as in temperate regions of the world [10]. They have 4 developmental stages in their life cycle: egg; larva (4 instars); pupa; and adult. Eggs hatch after 5–20 days, and after 25 days, the larvae become adult depending on species and temperature [11, 12].
Based on entomological and parasitological studies carried out in VL endemic areas of Iran, Phlebotomus alexandri, Phlebotomus keshishiani and Phlebotomus major are documented as the probable VL vectors in southern parts of Iran. In Ghiro- karzin County, Fars province, Ph. keshishiani and Ph. major are recognized as the VL vectors [13,14]. In Larestan, the VL vectors are unknown. Ph. alexandri is frequently found in mountainous regions and has been reported throughout Iran [15]. Ph. major was reported in 17 provinces in Iran that were located mostly in mountainous areas [15]. Ph.kandelakii, Phlebotomus perfiliewi and Phlebotomus tobbi are other vectors of VL found in northwestern Iran [16,17]. There have been no recent studies to determine the trend of the disease in these areas. The aim of this study was to identify epidemiological characteristics of VL among children in Larestan and Ghiro- karzin, Fars province over a period of 11 years.
Materials and Methods
1. Geographical area
Fars is one of the 31 provinces of Iran, located in the southern part of the country (29.62° N, 52.53° E). Larestan and Ghir-Karzin are 2 counties in south and southwest of Fars province, respectively. Due to topographical characteristics, there are 3 distinct climatic parts to this province. The first part is a hilly area in the north and northwest of the province. The second, is the central part of the province with a relatively moderate temperature, with hot and dry weather in summer. The third, is the south and southeast lowland regions of the province with moderate temperature in winter, and very hot and wet weather in summer [18].
Larestan, is composed of 7 districts that contain; Evaz, Banaruyeh, Beyram, Juyom, Sahray-ye Bagh, and Gerash and is located at a distance of 244 miles from Shiraz (Fars capital) with an area of approximately 16.809 sq. km. The average annual temperature is 21.5 °C and about 173 mm of precipitation falls annually (Figure 1).

Geographical location of Larestan and Ghir-Karzin counties, Fars province, southern Iran.
Ghir-Karzin is subdivided into 2 districts. The central and Afzar districts have a population of 69,910, and an area of 3.4 km2. The weather is hot with a mean annual rainfall of 136.4 mm, relative humidity of 35%, and annual temperature of 28.8°C (Figure 1). The most common jobs of the residents in these regions are animal husbandry and agriculture.
2. Data collection and analysis
This study was a retrospective study of hospitalized patients with a laboratory confirmation of VL on the files (in the Laboratory), which were retrieved and analyzed. Analyses were conducted using SPSS software version 16, with a probability (p) value of < 0.05 considered as statistically significant. The data were the result of passive monitoring, based on the notifications registered by all medical staff. The database contained all patients’ data including gender, age, residence and recovery situation. Chi-square and Pearson correlation coefficient test were utilized for data analysis.
Results
1. Larestan
There were 20 patients with a confirmed diagnosis of VL from 2004 to 2015, with 6 cases diagnosed in nomads, 11 cases in rural patients, and 3 cases in patients living in urban areas (p = 0.6). The most frequent number of patients was seen in 2004 (n = 6), and the lowest were in 2007–2009 (n = 0), and 2012 (n = 0). This difference was statistically significant (p < 0.05) (Figure 2). There were significantly more males (n = 14) than females (n = 6) in this study (p < 0.05) (Figure 3). Assessment of age categories showed that there were 2 patients under 1-years old, 17 patients in the 1–5 years age group, and 1 patient over 5 years old (Figure 4). Among these patients, 19 had complete recovery, while 1 patient died in 2004.
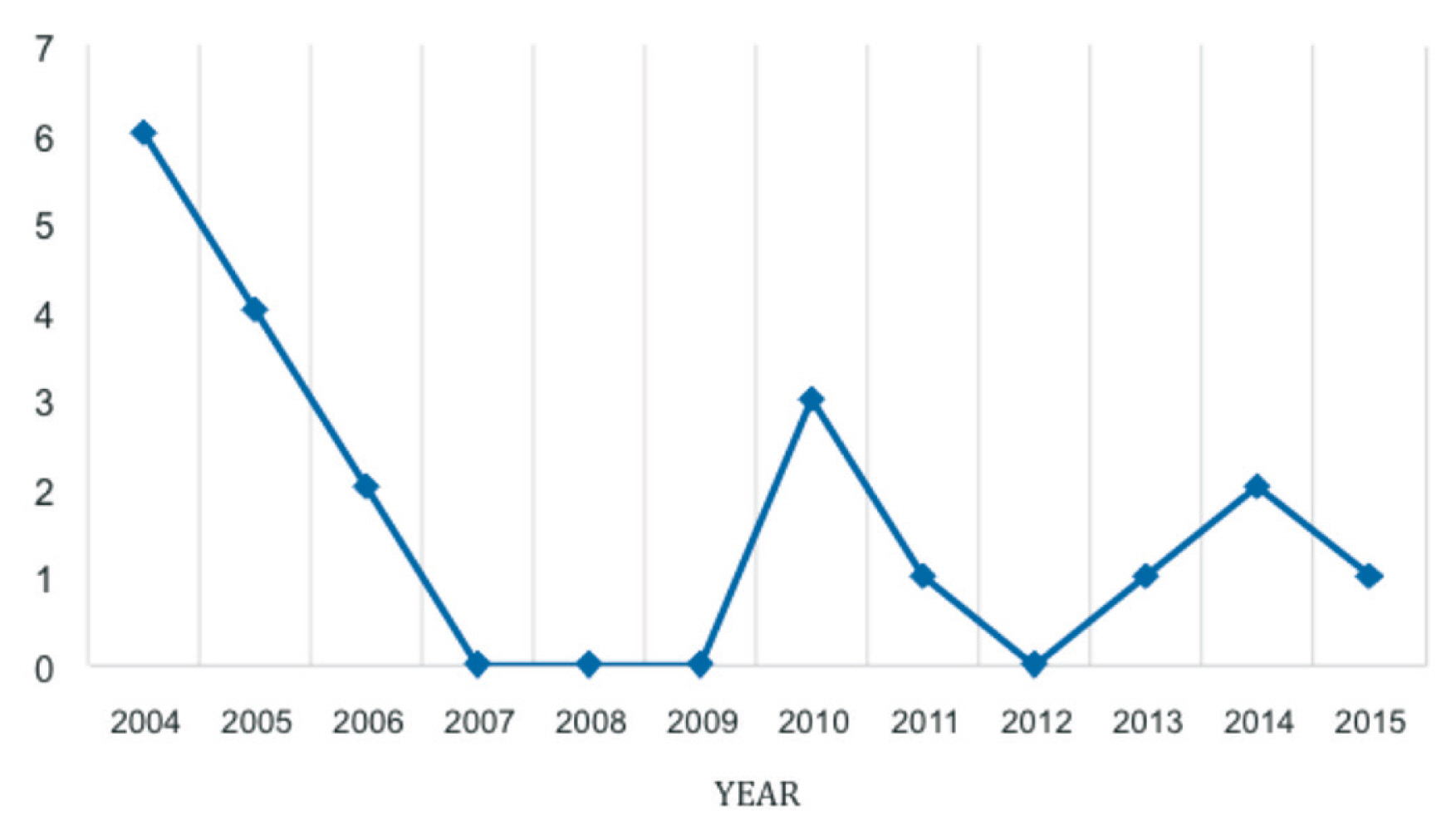
Frequency of VL cases in Larestan between 2004–2015.

The gender frequency of VL cases in Larestan based on year, between 2004–2015.
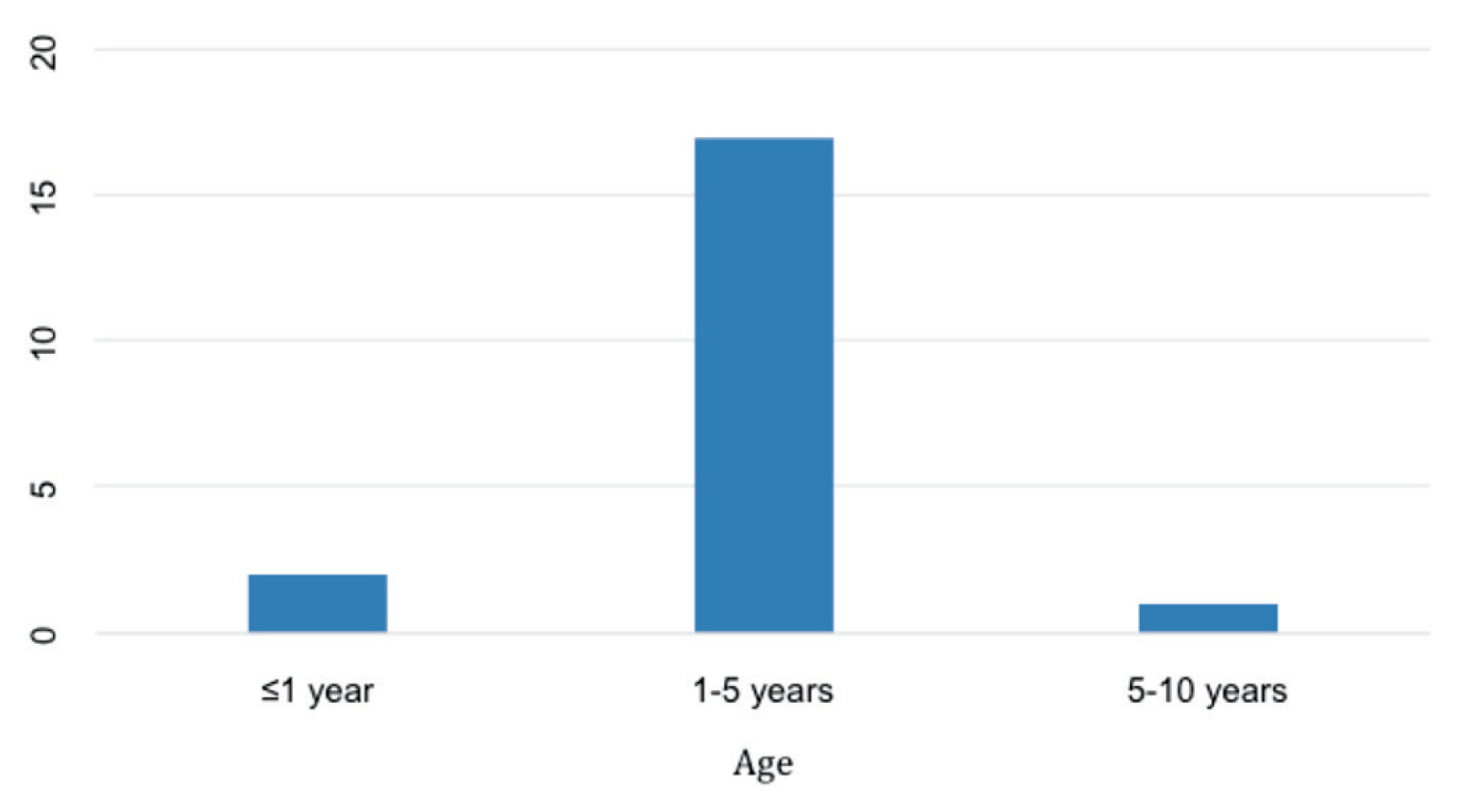
Frequency of VL cases in Larestan based on age between 2004–2015.
2. Ghir-Karzin
In the 25 patients with confirmed VL from 2004 to 2014, 1 patient was a nomad, 14 patients lived in rural areas, and 10 patients were living in urban areas (p > 0.05). There were 11 female patients and 14 males in this study (p > 0.05). In terms of age group categories, 4 patients were under 1-years old, 18 were in the 1–5 years age group, and 3 cases were over 5 years old (Table 1). The most frequent number of patients was seen in 2004 (n = 6) and the lowest were in the final years of 2011–14 (n = 1) and this difference was statistically significant (p < 0.05) (Figure 5). The highest numbers of patients were hospitalized in May, with 24 patients having complete recovery at discharge, while 1 patient died. Relapse has not been reported in these cases.
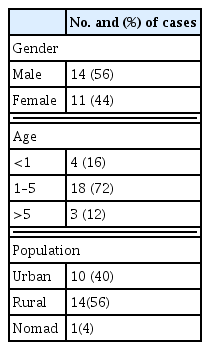
Distribution of VL cases according to demographics and population during 2004–2014 in Ghiro-Karzin County, southern Iran.
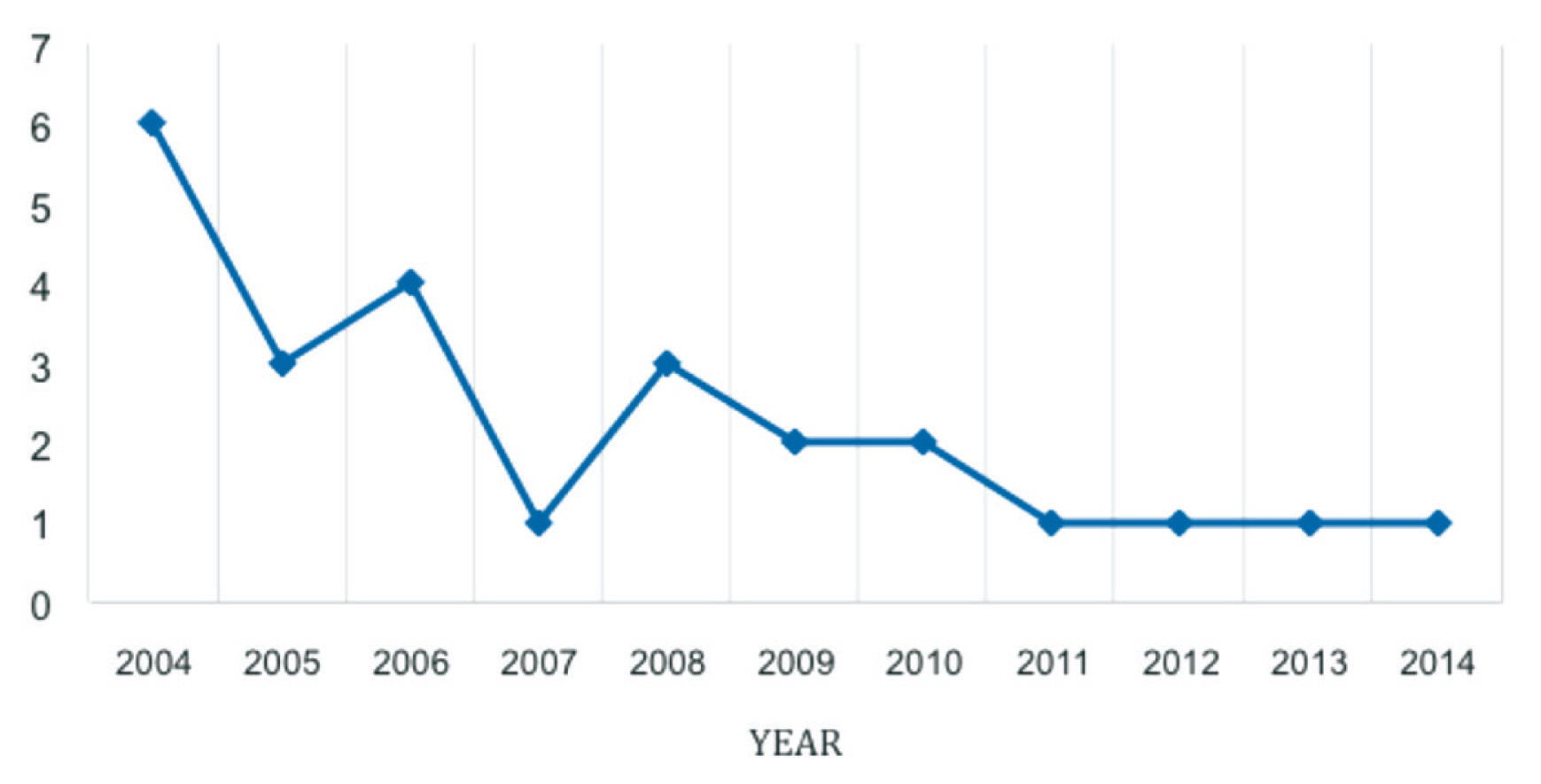
Frequency of VL cases in Ghir-Karzin, southern Iran, between 2004–2014.
The most common clinical symptoms in these 2 counties were prolonged fever, enlarged spleen and liver, anemia and weight loss, which was similar to previous reports [5,23]. Patients recovered within 2–4 weeks of treatment with Glucantime (mean dose 20 mg antimony/kg/day).
Discussion
Kala-azar is an arthropod-borne disease that affects millions of humans in more than 101 countries worldwide [1,3]. Due to the importance of this disease in Iran, in recent years, various studies examining aspects of VL have been conducted in the Fars Province, Southwestern Iran. A total of 260 cases of VL have been recorded between 2001 to 2009 in the south of Iran, based on hospital records. Mean age of patients was 3.5 years, with the highest prevalence in 2 year old patients. The disease appeared to be more common in males [5], and the results were identical to our findings. Nourabad, Kavar, Kazeroun, and Darab in Fars are known to be the main foci for the disease in south of Iran [19]. Based on this study, it seems that Larestan and Ghiro-Karzin are also important regions for the disease in Fars province. The prevalence of VL in the south of the country may be considered as the second focal region of the disease in Iran. The primary focus of the disease is in the north (Meshkine-Shahr) [20]. Between 1985 and 1990, 1,051 cases of VL were reported in Meshkin-Shahr [22], which was the region with the highest incidence of the disease [23]. A retrospective study on VL cases in Shiraz, Iran (from January 2010 to December 2013), showed that the highest rates of VL infection were in 2010, with 33 reported cases (62.3%), and the lowest rate in 2011, with 12 cases (37.5 %) [21]. Dashti and Dashtestan counties (Bushehr province) are other endemic regions of VL infection in the south of Iran, and between 1991 to 1997, 92 cases of VL were detected in those 2 counties [20,24]. Bushehr is near the south of Fars province, where this study was conducted. In the present study, 95% of the cases were from children under 5 years old. This feature could be due to a different immunological response in children to the parasite. Similarly, in the northwest of the country, 90% of VL cases were from children under 5 years old [22]. The main causative organism of VL in north and south Iran is L. infantum [4,5]. A few case reports have also shown the presence of L. major or L. tropica in patients with VL in Iran [25,26].
Zoonotic VL (ZVL) and anthroponotic VL (AVL) have been described as 2 main forms of VL. ZVL affects mainly young children and has the domestic dog as its main reservoir. It is the most dominant form in the Mediterranean basin and Brazil. AVL affects people of all ages and is transmitted from human-to-human via infectious sandfly bites. This form is epidemic in the northern Indian subcontinent and in the northeastern countries of Africa [27]. Therefore, it is important to pay attention to the control of vectors by indoor residual spraying (IRS) of households with insecticide and removal of infected dogs as the source of infection. Asymptomatic infected dogs play an important role in the epidemiology of VL in endemic areas and are the source of infection for both human and animals [28]. Various risk factors are involved in the disease, including socioeconomic status, environmental changes, malnutrition, population movement, and climate change [1].
The findings in this study indicate that there is a slightly higher incidence of VL in rural areas with the disease occurring more frequently in boys. This could be due to more exposure of boys to mosquitoes. Because the physical coverage is lower in boys than girls in Islamic countries. Despite a reduction in cases of the disease in recent years, continued attention in control methods should still be increased. Control measures including health education by public health professionals, improving the environment, and construction of new housing must be performed. In addition, further studies on the ecology, abundance and biology of vectors for disease control are required.
Acknowledgements
The authors gratefully acknowledge the cooperation of Health-Medical Systems of Larestan and Ghiro-Karzin Counties in executing this study.
Notes
Conflicts of Interest
The authors declare that there is no conflicts of interest.