The Effects of Task-Oriented Circuit Training Using Rehabilitation Tools on the Upper-Extremity Functions and Daily Activities of Patients with Acute Stroke: A Randomized Controlled Pilot Trial
Article information
Abstract
Objectives
The purpose of this study was to investigate the effect of task-oriented circuit training (TOCT) using the rehabilitation tools for upper extremity function upon the daily life of patients with acute stroke.
Methods
Eighteen patients with acute stroke were randomly allocated into either the experimental group or the control group. The experimental group performed the TOCT program using rehabilitation tools, whilst the control group had neuro-developmental treatment. Both groups received 30 minutes of treatment per session, 5~6 times per week, for 4 weeks. The assessments conducted were the Fugl-Meyer assessment, motor activity log and stroke impact scale to compare the upper extremity function and activities of daily living.
Results
The results showed a significant improvement in the TOCT group compared with the neuro-developmental treatment group in the amount of motor activity use and high stroke impact score, indicating recovery (p < 0.05).
Conclusion
The TOCT program using rehabilitation tools could have a positive impact on acute stroke patients use of their upper extremity.
Introduction
Stroke is characterized by neurological deficits resulting from cerebrovascular damage and causes neurological problems such as cognitive, motor and sensory, speech and language, and emotional disorders. These problems limit participation in daily activities after a stroke and cause major life changes [1]. The earlier rehabilitation occurs the better the prognosis for the acute stroke patient [2]. The patient’s neurological condition will dictate an appropriate intervention [3] which may be constraint-induced movement therapy, mirror therapy, motor imagery training, task-oriented training (TOT), and biofeedback for the function of upper extremities [4–8]. Task-oriented training is a clinical therapeutic approach based on rehabilitation science and is grounded in the principles of motor learning, motor control, and neuroplasticity. It enables patients with functional disabilities to self-motivate; they select and perform various tasks and practice them accordingly [9]. This intervention is referred to using various terms, including task-based, task-related, activity-based, goal-oriented, and task-specific training [1]. Circuit training is a training method that controls the intensity of training systematically and gradually as an intervention to help the repeated training of a larger number of tasks [10]. Many studies have found circuit training to be effective at improving lower extremity functions in patients after chronic stroke [10–12]. Occupational therapists have assigned such training to suit the functional characteristics of upper-extremity movement patterns [13]. They have also used rehabilitation tools in TOT for many decades [14–16] but the effects of task-oriented circuit training (TOCT) on upper extremity functions and activities of daily living (ADL) have not yet been clearly identified, and studies on its effects on acute stroke patients are limited. In addition, few studies have examined the use of rehabilitation tools in TOCT. Therefore, the purpose of this study was to investigate the effects of TOCT using rehabilitation tools on upper extremity functions and ADL in acute stroke patients.
Materials and Methods
1. Participants
Eighteen subjects were recruited and consented to participate in the study. The subjects were from two different hospitals in South Korea, one located in Incheon and one in Bucheon. The inclusion criteria were as follows: (1) acute stroke patients who developed their condition within the past 30 days and were confirmed to have hemiparesis due to cerebral infarction; (2) those who scored 24 points or above in the Mini-Mental State Examination Korean version, and could understand instructions; (3) those who did not have serious joint contracture, or musculoskeletal pain or fracture; (4) those whose Brunnstrom recovery stage in the proximal and distal regions of the affected upper extremities was 3 or below; and (5) those who had sufficient endurance to engage in 30 minute training sessions. The exclusion criteria were as follows: (1) those who had cognitive disorders such as neglect and apraxia; (2) those who had retrograde conditions such as dementia; and (3) those who had serious depression. All participants were informed of the aim of the study and signed an informed consent form. The study was approved by the Jungwon University Ethics Committee for Human Investigations before patient participation (1044297-HR-201610-013-01).
2. Measurements
2.1. Fugl-Meyer assessment of the upper extremity
The Fugl-Meyer assessment of the upper extremity (FMA-UE) is used to test the degree of functional recovery in the upper extremity function of stroke patients [17,18]. The maximum score of the FMA-UE is 66 and the rating is based on direct observation of the motor performance at each item using a 3-point ordinal scale (0 = cannot perform, 1 = performs partially, and 2 = performs fully). In the FMA-UE, the inter-rater and intra-rater reliability is 0.97 [19].
2.2. Motor activity log
The motor activity log (MAL) is a semi-structured, interview-based measuring method that measures 30 daily activities to identify the degree of independence in the affected upper extremity [20,21]. Performance of each activity is measured by determining the amount of use and the quality of movement. Both the amount of use and the quality of movement are based on a scale of 0 to 5. For the amount of use, 0 indicates “not using at all” and 5 indicates “using the affected side as often as before the occurrence of the disease.” For the quality of movement, 0 indicates “not being able to use the affected side during activities” and 5 indicates “being able to use the affected side as much as before the occurrence of the disease.” The MAL-14 item version was used for this study. The MAL is a testing tool with high levels of reliability; the internal consistency is 0.88–0.95, the inter-rater reliability is 0.90, and the test-retest reliability is 0.94 [22].
2.3. Stroke impact scale
The stroke impact scale (SIS) is a self-perception measuring tool based on a 5-point scale. The SIS is comprised of 64 items in the 8 areas of muscular strength, memory and thinking, feeling and emotion, communication, basic daily activities and instrumental daily activities, movability, hand function, and social participation. The total score ranges from 0 to 100, with 0 indicating “having not recovered at all” and 100 indicating “having recovered to the fullest.” Using the SIS Korean 3.0 version, the 4 domains (strength, hand function, ADL, stroke recovery) were assessed according to the purpose of the study. The inter-rater reliability was 0.570 in strength, 0.635 in hand function, 0.595 in ADL, and 0.527 in stroke recovery [23].
3. Procedures
Eighteen subjects were selected according to the study’s selection criteria, and the methods and procedures were explained to them before starting the experiment. After a preliminary evaluation to identify their present functional levels, subjects were randomly assigned to either an experimental group for TOCT, or a control group for neurodevelopmental treatment (NDT). Both groups participated in training sessions for 30 minutes a day, 5 to 6 days per week, over a period of 4 weeks, for a total of 22–24 sessions.
There were 6 rehabilitation tools (putty, skate, incline board, stacking cone, range of motion arc, ring) selected which are used widely in occupational therapy [24]. TOCT included 6 different tasks in which subjects performed for 5 minutes in each task in a circular manner. Each task was based on 4 levels of difficulty and the therapist provided a task fit for the subject’s ability level. The guidelines required that tasks should be easily performable in a clinical environment, and that training should aim for active movements, induce the suppression of compensatory movements, gradually increase in speed and frequency, encourage the subject to make further efforts, and increase the difficulty level when a subject’s function improves [25].
The control group underwent NDT to improve the functions of the trunk and upper extremities. NDT aims not only to improve muscle tone and reflexive and abnormal movement patterns and postures, but also to normalize sensorimotor elements such as sense, perception, and memory [1]. In this study, the NDT group performed its training without using tools under the guidance of therapists. The intervention consisted of a preliminary exercise for 10 minutes and an NDT-based manual exercise for 20 minutes [26].
4. Statistical analysis
The data were analyzed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). For descriptive statistics, Chi-square test and Mann-Whitney U test were performed. Wilcoxon signed rank test was performed to compare the FMA, MAL, and SIS scores of the 2 groups. The statistical significance level was set at α = 0.05.
Results
The experimental and control groups did not show statistically significant differences in age, gender, education level, affected side, dominant hand, damaged location, disease duration, MMSE score, and clinical experience of therapists (p > 0.05). The subjects’ general characteristics are shown in Table 1. Comparing the number of treatment sessions between the 2 groups also did not show statistically significant differences.
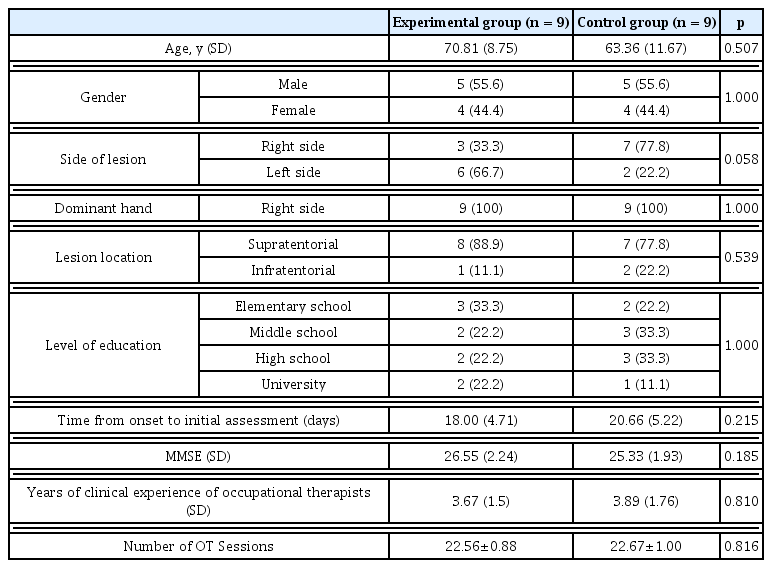
The general characteristics of the subjects.
Each group exhibited statistically significant improvements in FMA, MAL, and SIS scores for all except “using the spoon & chopsticks” in the control group (p < 0.05). The TOCT group achieved statistically significant improvement in the MAL, arm and grip strengths on the affected side, and “using the spoon & chopsticks” in the SIS, when compared to the control group [p < 0.05 (Table 2, 3)].
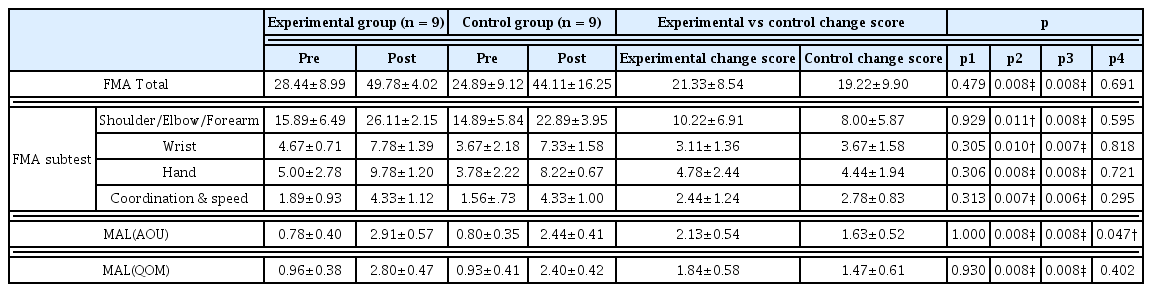
Comparison of upper extremity functions (FMA, MAL) for two groups.
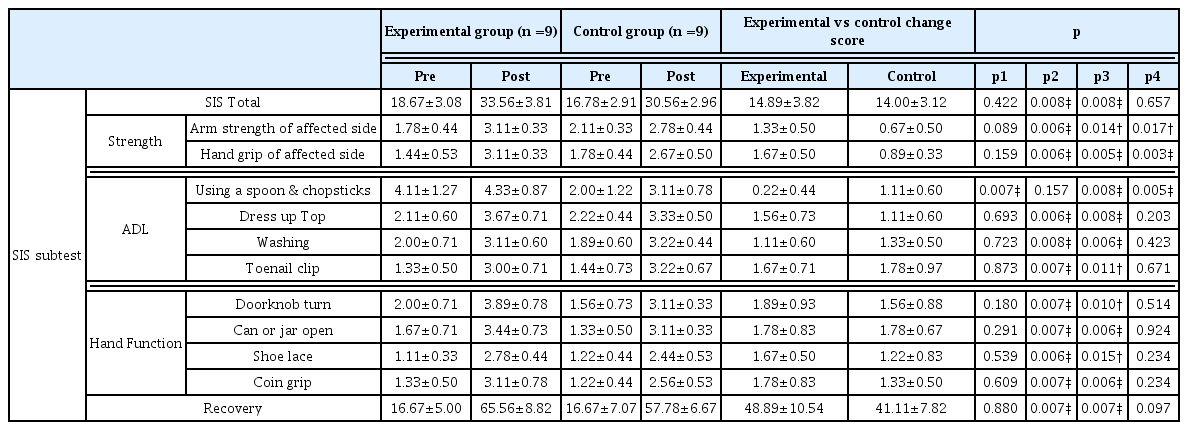
Comparison of stroke impact scale for two groups.
Discussion
This study was conducted to confirm the effects of a TOCT program using rehabilitation tools on upper-extremity functions and daily activities of stroke patients. The results showed that both TOCT and NDT can improve stroke patients’ use of upper extremities in the acute phase, but that TOCT led to an overall higher level of improvement than NDT in functional recovery.
Jang et al reported that the specificity, duration, and frequency of tasks brought statistically significant changes in the recovery of the upper extremities and neural reorganization in stroke patients [27].
In the present study, repetitive training of the upper extremities through TOCT had positive effects on patients’ recovery and neural reorganization. However, the NDT group focused on normalizing muscle tone and supporting the affected side, so they achieved a comparatively lower level of functional recovery than the TOCT group. The NDT group showed statistically significant differences in the “using the spoon & chopsticks” item of SIS. This is probably because the control group has a greater number of patients with paralysis in the non-dominant (left) hand. The results are similar to the previous study which reported that circuit training showed significant improvements on lower-extremity motor control, balance, gait endurance and daily activities when compared to the NDT group in subacute stroke inpatients [28]. Also, other studies reported TOCT also had a positive effect on mobility and upper limb functions in acute and chronic stroke patients [29,30]. These findings suggest that TOCT is effective in improving functional outcomes during stroke rehabilitation.
This study has some limitations. Firstly, simple exercises were conducted using rehabilitation tools, not ADL tasks. Some improvement was seen in SIS scores, but changes in ADL task abilities were not examined. Secondly, the affected side was not controlled between the 2 groups before the intervention. Because of the difference in the affected side, the 2 groups showed significantly different results in the SIS task of “using the spoon & chopsticks” before the intervention. This may have been due to the small sample size. Thirdly, patients with acute stroke can have spontaneous recovery, so therapists should apply TOCT according to functional recovery. Future studies should target chronic stroke patients, and long-term follow-up studies should involve a larger number of subjects to generalize the research results.
Acknowledgments
This work was supported by the Jungwon University Research Grant (Code: 2016-052).
Notes
Conflicts of Interest
No potential conflicts of interest relevant to this article was reported.