The Association Between Lung Function and Type 2 Diabetes in Koreans
Article information
Abstract
Objectives
This study was performed to test the association between lung function and type 2 diabetes mellitus (T2DM) in Korean patients.
Methods
Data from the 6th Korea National Health and Nutrition Examination Survey (2013 to 2015) was used in this study. There were 3,466 individuals aged between 40 and 80 years, with T2DM, who had a smoking and alcohol status listed, and blood analysis (including blood pressure), were included in this study. Lung function, measured by spirometer ventilatory dysfunction was categorized into 3 patterns: normal, restrictive ventilatory dysfunction, and obstructive ventilatory dysfunction (OVD).
Results
Based on multivariate logistic regression analysis, individuals with restrictive ventilatory dysfunction had an increased odds ratio (OR 1.615, 95% CI 1.137–2.294) for T2DM compared with individuals with normal ventilatory function, whereas OVD had no increase in the odds ratio (OR 1.169, 95 % CI 0.857–1.594). Model 1, which adjusted for age and gender, showed that the probability of having restrictive disorder was 1.559 times (95% CI 1.617–2.082) higher for prediabetes patients, and 2.320 times (95% CI 1.611–3.343) higher for T2DM patients, compared to normal individuals. For Model 4, which was fully adjusted for variables, the probability of having a restrictive disorder was 1.837 times higher for T2DM patients (95% CI 1.260–2.679).
Conclusion
Restrictive ventilatory dysfunction, but not OVD, was associated independently with T2DM.
Introduction
Reduced pulmonary function is defined by obstructive and restrictive patterns, and increases the risk of hypertension, and systematic low-grade inflammation in the lungs [1]. Additionally, a reduction in pulmonary function has been associated previously with an increased risk of death after adjusting for the patient’s age, gender, race, and smoking status [2]. Interestingly, several studies have reported a strong association between reduced lung function and type 2 diabetes mellitus (T2DM) [3–5].
A condition causing an obstructive pattern of reduced pulmonary function, hinders a person’s ability to exhale air from their lungs. This is observed as a significant reduction in the forced expiratory volume in 1 second (FEV1), in relation to the forced vital capacity (FVC) that can be displaced from the lung. Chronic obstructive pulmonary disease is the main type of obstructive lung disease [6].
On the other hand, a restrictive, but not an obstructive pattern of reduced pulmonary function, shows a significant reduction in both the FVC and FEV1, mainly due to a defect in thoracic compliance [7]. A restrictive pattern of reduced pulmonary function has been reported to be present in 10–15% of individuals older than 70 years, and can be caused by several pathological conditions, such as diabetes, obesity, heart failure, nonspecific lung fibrosis, and muscular weakness [8]. A restrictive pattern of reduced pulmonary function has also been reported to be associated with an increased risk of T2DM. Furthermore, in a previous study, diabetic patients showed a significantly reduced predicted FVC and FEV1 compared to non-diabetic patients at the baseline [9].
There is still a lack of large scale studies that have investigated diabetic and non-diabetic patients and lung dysfunction in Asians, and fewer studies that have investigated T2DM. As such, this study’s aim was to assess whether reduced pulmonary function or selective restrictive/obstructive pattern was associated with T2DM. Data from the Korea National Health and Nutrition Survey (KNHANES) was used in this study.
Materials and Methods
1. Data source and study population
This study used the data from the 6th KNHANES (2013–2015), which is a nationally representative population-based survey. The survey is cross-sectional and designed to examine the health and nutritional status of the non-institutionalized Korean population, and is conducted by the Division of Chronic Disease Surveillance, Korea Centers for Disease Control and Prevention. The KNHANES survey consists of 4 different components: 1) a health interview, 2) a health behavior survey, 3) a health examination, and 4) a nutrition survey. The survey information was collected by face-to-face interviews after the agreement of the individual, followed by a health examination.
Among the 22,948 individuals who participated in the KNHANES, a total of 14,116 (who had not had a spirometry test), and 940 others (not measured type 2 diabetes mellitus status) were excluded. In addition, individuals were selected for those ≥ 40 < 80 years old. Furthermore, individuals with an unknown smoking or alcohol status (n = 147) or lacking blood analysis (n = 4,279), including blood pressure, were all excluded from this study. After passing the study selection criteria, a total of 3,466 participants were included in this study for analysis.
2. Covariates
The general patient-characteristic information including age, gender, body mass index (BMI), waist circumference (WC), low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglyceride, systolic blood pressure, diastolic blood pressure, and smoking status were included as covariates in the analysis model. The weight of the patient was measured on a calibrated balance-beam scale, and their height was measured in an upright position, using a stadiometer. The BMI was calculated by dividing weight (kg) by height (cm2). In the KNHANES, the respondents’ height and weight were measured by trained examiners. The WC was measured at the midpoint between the bottom of the rib cage and the top of the lateral border of the iliac crest during full expiration. Blood samples were collected from individuals in the morning after overnight fasting and were analyzed at a national central laboratory. The participants blood pressure was measured using a mercury sphygmomanometer, in a seated position, and after a 10-minute rest period. Two measurements were taken for every individual at a 5-minute interval. An average of 2 measurements was used for the data analyses. Cigarette smoking was categorized as never smoked, ex-smoker, or current smoker, and alcohol status was dichotomized as current user and non-user of cigarettes.
3. T2DM
The KNHANES classified an individual with diabetes using 3 different measures. Firstly, participants were asked whether or not they had a diabetic condition, and whether they had ever been diagnosed with diabetes by a physician. Individuals who self-reported that they had been diagnosed with diabetes by a physician were classified as diabetic. Secondly, individuals were classified as having diabetes during the health examination if their fasting glucose level was > 126 mg/dL. Lastly, individuals who self-reported that they were receiving treatment for diabetes were also classified as having a diabetic condition.
Based on these 3 indicators for diabetes, all individuals were recategorized into a diabetic and non-diabetic condition. In addition, the level of fasting glucose was divided into normal (< 100 mg/dL), prediabetic (100–125 mg/dL), and T2DM (≥ 126 mg/dL) to test for an association of ventilatory dysfunction, with an individual’s probability of developing T2DM. The KNHANES did not list the type of diabetes. Thus, it was assumed that if a respondent was diagnosed with diabetes before the age of 19 years, their diabetes was type 1, and it was assumed that none of them were affected by lung dysfunction.
4. Measurement of lung function
Lung function was measured by using a dry rolling seal spirometer (Model 2130; Sensor Medics, Yorba Linda, CA, USA) according to the criteria of the American Thoracic Society and the European Respiratory Society for standardization [10]. Spirometric data obtained on-site by clinical technicians were transferred to an internet review center for processing. The data were carefully examined and compared against criteria metrics for acceptability, reproducibility, and quality control. A principal investigator validated and stored the data in a Korea Centers for Disease Control and Prevention repository management system.
The participants were classified in groups according to their respiratory patterns: normal (FEV1/FVC ≥ 0.70, FVC ≥ 80% predicted), restrictive ventilatory dysfunction (RVD), (FVC < 80% predicted, FEV1/FVC ≥ 0.70), and obstructive ventilatory dysfunction (OVD), (FEV1/FVC < 0.70) [11].
5. Statistical analysis
Data were analyzed using SPSS 22.0 (IBM Corp., Armonk, NY, USA). Differences among groups were assessed using χ2 test for categorical variables, and the analysis of variance (ANOVA) for continuous variables. Bonferroni’s test was used for post hoc multiple comparisons in ANOVA. Multivariate logistic regression analyses were used to estimate the odds ratios (ORs) with 95% confidence intervals (CI) for T2DM, and prediabetes, using the fasting glucose levels of the normal group as a reference category, after adjusting for other clinical and biochemical variables. p < 0.05 were considered statistically significant.
Results
The clinical characteristics of the individuals according to the ventilatory function are shown in Table 1. From the 3,466 participants, 2,663 (76.83%) were placed in the normal group, 315 (9.14%) in the RVD group, and 488 (14.07%) in the OVD group. When comparing the characteristics of the individuals’ ventilatory function, the prevalence rates of T2DM were reported at 13.7% for the normal group, 26.4% for the RVD group, and 23.0% for the OVD group. Individuals placed in the RVD group had higher fasting glucose levels, BMI, WC, and triglyceride values than the individuals in the normal and OVD groups.
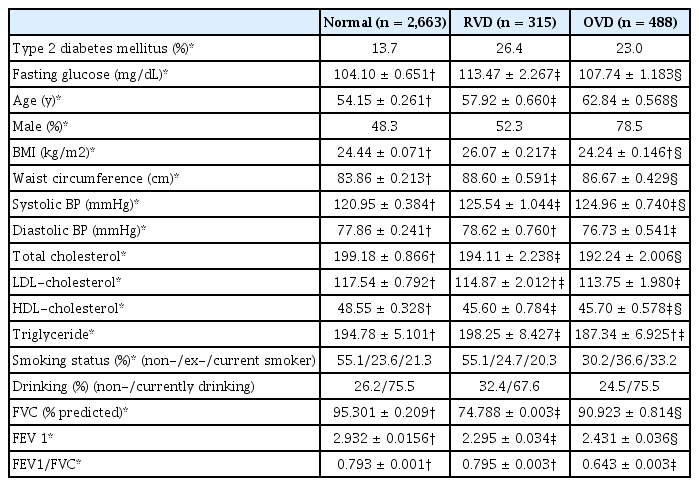
Clinical characteristics of individuals with normal, restrictive and obstructive ventilatory dysfunction.
Based on the fasting glucose status of the individuals (Table 2), there were 1,820 (53.52%) with normal values, 1,065 (30.73%) with prediabetes, and 581 (16.76%) with T2DM. Additionally, the prevalence of RVD in these groups was reported at 6.2%, 9.9%, and 14.3%, respectively, indicating that those with a higher fasting glucose level had a higher prevalence of RVD. Furthermore, a significant relationship was determined between a higher fasting glucose level and a lower FVC, FEV1, and FEV1/FVC.
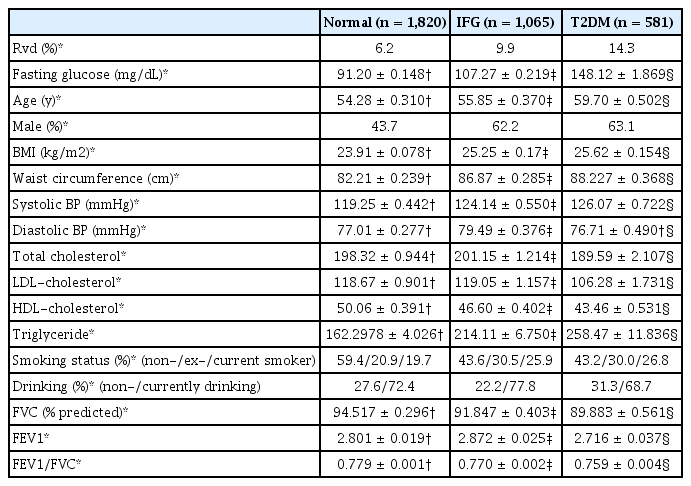
Respiratory function (spirometric parameters) in normal, impaired fasting glucose, and type 2 diabetic individuals.
Based on the multivariate logistic regression analysis, individuals with RVD were determined to have an increased OR (1.615, 95% CI 1.137–2.294) for T2DM when compared with individuals with normal ventilatory function (p < 0.01). However, with regards to OVD, the OR was similar (OR 1.169, 95% CI 0.857–1.594) and this was after fully adjusting for Model 4 (Table 3).
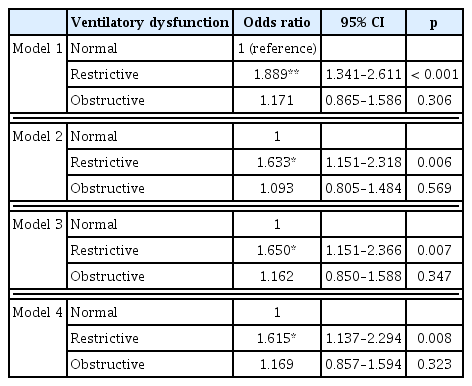
The adjusted odds ratios for type 2 diabetes mellitus according to the ventilatory dysfunction by multivariate logistic regression analysis.
To determine whether ventilation dysfunction in individuals who were not classified as diabetic, but were likely to develop T2DM, a multivariate logistic regression analysis was performed using 3 fasting glucose groups: normal (< 100 mg/dL), prediabetic (100–125 mg/dL), and T2DM (≥ 126 mg/dL; Table 4). Model 1, which was adjusted for age and gender, showed the probability of having a restrictive lung disorder was 1.559 times higher (95% CI 1.617–2.082) in the prediabetes group (p < 0.01), and 2.320 times higher (95% CI 1.611–3.343) in the T2DM 1 (p < 0.001), compared to those in the normal group. In Model 4, which was fully adjusted for variables, the probability of having a restrictive lung disorder was 1.837 times (95% CI 1.260–2.679), which was significantly higher in the T2DM group compared with the normal group (p < 0.01). In contrast, there was no association between OVD and fasting glucose levels in any model.

The adjusted odds ratios for ventilatory dysfunction according to the fasting glucose level by multivariate logistic regression analysis.
Discussion
The main finding of this study illustrated that ventilatory dysfunction was positively associated with abnormal glucose levels. Particularly a restrictive, but not obstructive respiratory pattern of reduced pulmonary function was determined to be linked to an increased OR for T2DM, which was independent of major confounding factors such as individual’s age, obesity, or smoking status.
A previous study using cross-sectional research that investigated the relationship between ventilatory dysfunction and glucose levels in patients, did not distinguish between restrictive and obstructive respiratory patterns of reduced pulmonary function, and demonstrated an independent association between low lung volume and insulin resistance [5]. In contrast, in this current study, an association between the restrictive ventilatory pattern of reduced pulmonary function and T2DM was determined.
A previous study has shown that there are insulin receptors in the lung pleura, and that hyperglycemia can contribute to reduced lung capacity [12]. The outcome of this current study was consistent with those results, in which the average FVC, FEV1, and FEV1/FVC values in the prediabetes and T2DM groups, showed a significant reduction in lung capacity in the fasting glucose levels compared to the group with normal glucose levels (non-diabetic). A follow-up study showed that only RVD was associated with the prevalence of diabetes in men and women in North America, which was not the case for OVD [8]. In addition, a study of Swedish patients reported a negative correlation between RVD and prevalence of diabetes [1,13].
Studies investigating the correlation between reduced lung function and diabetes among Asians remain scarce. It has been reported that Japanese men had a low FVC and FEV1, but not a low FEV1/FVC ratio, which increased the risk of diabetes after adjusting the model for fasting glucose levels [14]. In another study in Korean men, the lowest quartiles of FVC and FEV1 showed an increased OR for T2DM [15]. However, a major shortcoming of these 2 studies was that only men were investigated. In contrast, in this study the association between T2DM and RVD was determined for both men and women.
It has been overwhelmingly shown that smoking has a significant adverse effect on lung function [16]. Although smoking is the major cause of lung dysfunction, the risk for T2DM that is positively associated with RVD, is independent of patients’ smoking status in this current study (Model 4). Other studies have also shown that the relationship between RVD and the prevalence of diabetes is not significantly dependent on a patient’s smoking status [1,8]. This implies that smoking status does not have a clear effect on the positive association between T2DM and ventilatory dysfunction.
Previous studies have shown that there may be a relationship between reduced ventilatory function and T2DM. Obesity, a condition well-known for its association with hyperglycemia, is not only a risk factor for T2DM, but also a major cause of reduced lung capacity [17]. In a systemic review, the findings showed that obese individuals had a significantly lower FVC compared to healthy ones, and there was a significant negative association between the restive response pattern and obesity [18]. However, based on the results in this current study, the OR of RVD with the highest fasting glucose level (T2DM) was reported at 1.835 (95% CI 1.261–2.670) after adjusting for the BMI and WC. Furthermore, no significant difference was reported for prediabetes fasting glucose levels. Thus, obesity may explain the association between lung restriction and prediabetes, but it does not appear to be the stage of diabetes. Additionally, insulin resistance, illustrated by cells that fail to respond normally to the hormone insulin, and a major etiology of T2DM may alter the glucose absorption of thoracic muscles, thereby causing a reduced respiratory muscle function, and eventually the RVD [19,20].
Despite several meaningful findings in this study, there are some limitations that must be mentioned. Firstly, although the association between RVD and T2DM may be helpful in providing additional information about the nature of this relationship, determination of the rudimentary cause of RVD and OVD in patients was not possible. For this reason, future studies should include mechanisms to clarify the relationship between impaired lung function and T2DM. Secondly, the limitation of the KNHANES is that the individuals who participated in this survey have relatively mild-to-moderate levels of comorbidities, that is, a small number of severe cases of diabetes or lung dysfunction in patients influence the analysis of the results. This limitation might be overcome by further case-control or cohort studies. Thirdly, the KNHANES data were conducted on respiratory function tests in the over 40’s. Type 1 diabetes is commonly known to occur in children. For this reason, it was not possible to investigate the relationship between T1DM and RVD. Therefore, future research should investigate the correlation between ventilatory dysfunction and the type of diabetes. Despite these limitations, this current study has significant clinical and research implications because it is representative of the Korean population, and is a large sample size, which allowed multiple statistical adjustments increasing the sensitivity, validity and robustness of the study.
The findings of this study showed that RVD, but not OVD, in Koreans is highly associated with the prevalence of T2DM, regardless of various diabetes risk factors that may confuse or mediate these associations.
Notes
Conflicts of Interest
The authors have no conflicts of interest to declare.