
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 9(5); 2018 > Article
-
Original Article
Factors Affecting Smoking Cessation Success of Heavy Smokers Registered in the Intensive Care Smoking Cessation Camp (Data from the National Tobacco Control Center) - Hansol Yeoma, Hee-Sook Lima,b, Jihyun Minc, Seoni Leec, Yoon-Hyung Parka,c
-
Osong Public Health and Research Perspectives 2018;9(5):240-247.
DOI: https://doi.org/10.24171/j.phrp.2018.9.5.05
Published online: October 31, 2018
aDepartment of Preventive Medicine, Soonchunhyang University, Cheonan, Korea
bDepartment of Food and Nutrition, Yeonsung University, Anyang, Korea
cChungnam Tobacco Control Center, Cheonan, Korea
- *Corresponding author: Yoon Hyung Park, Department of Preventive Medicine, Soonchunhyang University, Cheonan, Korea, E-mail: parky@sch.ac.kr
• Received: May 17, 2018 • Revised: September 20, 2018 • Accepted: September 6, 2018
Copyright ©2018, Korea Centers for Disease Control and Prevention
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
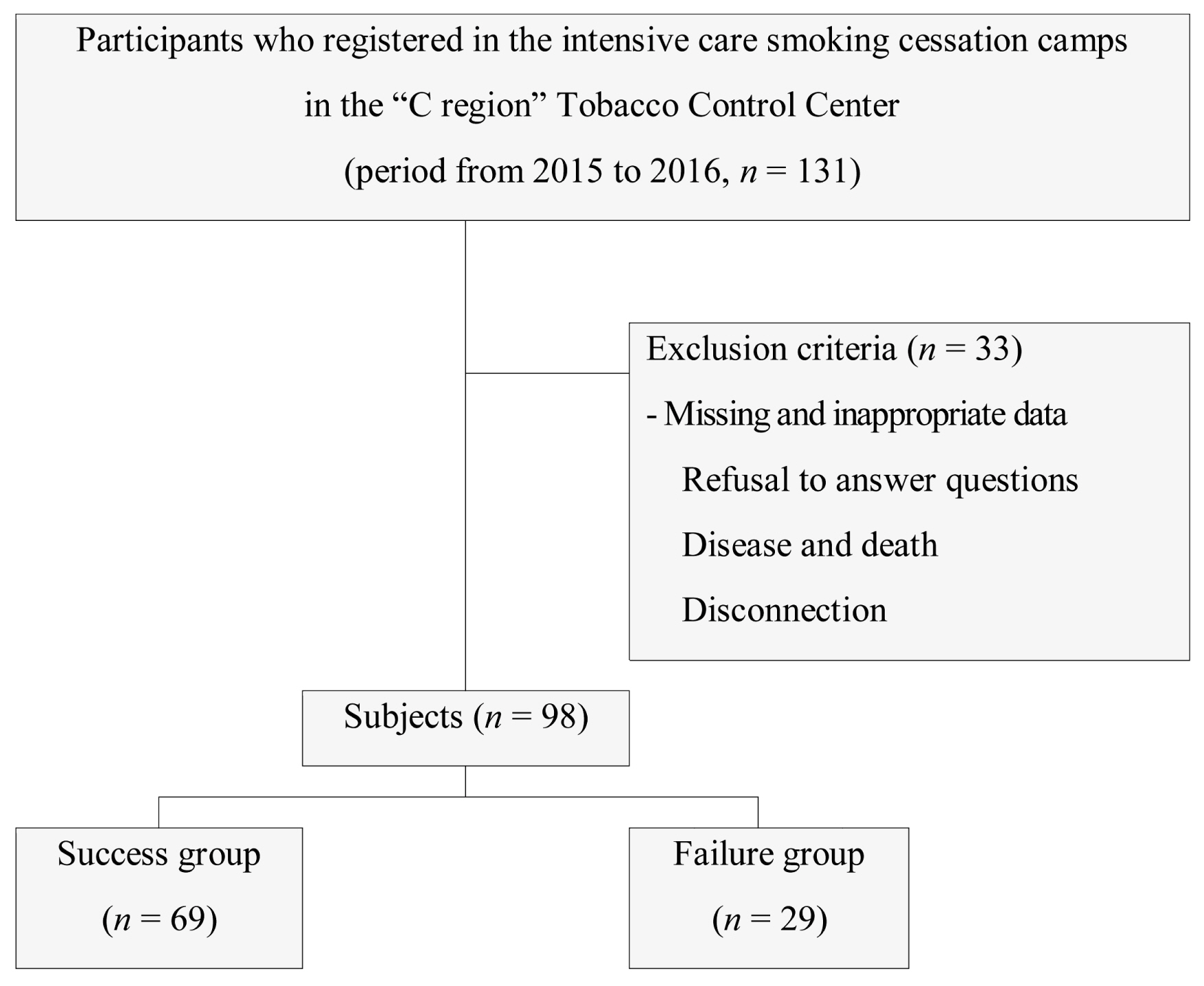
Figure & Data
References
Citations
Citations to this article as recorded by 
- Evaluation of Smoking Cessation Intervention Effectiveness in Smoking Cessation Clinics — China, 2019–2021
Li Xie, Yongfu Yan, Yan Yang, Yi Nan, Lin Xiao
China CDC Weekly.2023; 5(21): 469. CrossRef - Factors Associated with Smokers Attending More Than One Smoking Cessation Clinic Visit
Oh Beom Kwon, Chihoon Jung, Auk Kim, Gihwan Byeon, Seung-Joon Lee, Woo Jin Kim
Journal of Clinical Medicine.2023; 12(23): 7222. CrossRef - Effects of a supportive workplace environment on the success rate for smoking cessation camp
Woojin Kim, A Ram Kim, Minsu Ock, Young-Jee Jeon, Heun Lee, Daehwan Kim, Minjun Kim, Cheolin Yoo
Annals of Occupational and Environmental Medicine.2023;[Epub] CrossRef - Sigara Bırakma Polikliniğine Başvuran Bireylerde Tedavi Başarısını Etkileyen Faktörler
Derya KOCAKAYA, Hatice ŞENOL, Sezer ASLAN, Ahmed Mahmud ÇIRAKOĞLU, Merve ÇAKIR, Hatice TELCİ, Mehmet ÇETİNKAYA, Sehnaz OLGUN, Ayşe Nilüfer ÖZAYDIN, Ceyhan BERRİN
Bağımlılık Dergisi.2022; 23(1): 69. CrossRef - Smoking cessation rates in elderly and nonelderly smokers after participating in an intensive care smoking cessation camp
Jae-Kyeong Lee, Yu-Il Kim, Sun-Seog Kweon, In-Jae Oh, Yong-Soo Kwon, Hong-Joon Shin, Yu-Ri Choe, Ha-Young Park, Young-Ok Na, Hwa-Kyung Park
Medicine.2022; 101(30): e29886. CrossRef - Patterns and predictors of smoking relapse among inpatient smoking intervention participants: a 1-year follow-up study in Korea
Seung Eun Lee, Chul-Woung Kim, Hyo-Bin Im, Myungwha Jang
Epidemiology and Health.2021; 43: e2021043. CrossRef - Factors affecting smoking initiation and cessation among
adult smokers in Fiji: A qualitative study
Masoud Mohammadnezhad, Mondha Kengganpanich
Tobacco Induced Diseases.2021; 19(December): 1. CrossRef - “STOP the PUFF! Tayo’y mag bagong BAGA, SIGARILYO ay ITIGIL”: A Pilot Community-based Tobacco Intervention Project in an Urban Settlement
Irene Salve D Joson-Vergara, Julie T Li-Yu
Journal of Medicine, University of Santo Tomas.2021; 5(1): 586. CrossRef - Smoking cessation correlates with a decrease in infection rates following total joint arthroplasty
Christina Herrero, Alex Tang, Amy Wasterlain, Scott Sherman, Joseph Bosco, Claudette Lajam, Ran Schwarzkopf, James Slover
Journal of Orthopaedics.2020; 21: 390. CrossRef
 PubReader
PubReader Cite
Cite
