Comparison of Purgative Manna Drop and Phototherapy with Phototherapy Treatment of Neonatal Jaundice: A Randomized Double-Blind Clinical Trial
Article information
Abstract
Objectives
Herbal remedies such as purgative manna are used to treat neonatal jaundice. In this study Bilineaster drop (purgative manna) and phototherapy, and phototherapy treatment alone were compared by assessing phototherapy duration and number of days in hospital.
Methods
There were 150 consecutive term neonates with jaundice, weighting from 2,500 g to 4,000 g enrolled in this randomized double blind clinical trial. The neonates were randomly assigned to intervention and control groups. The control patients received only phototherapy and the intervention group underwent phototherapy treatment and purgative manna drop (5 drops per kg of body weight, 3 times a day). Direct and total measurements of bilirubin concentration in the serum were measured and the reduction in concentration of bilirubin was calculated.
Results
There were 28% of patients whose hospital duration following phototherapy was 2 days, for Bilineaster and phototherapy treatment this was 49.3% of patients. At 48 hours and 72 hours the reduction in the concentration of total bilirubin in the serum was statistically significantly different across groups (p < 0.05) but at 24 hours and 96 hours there were no significant differences between groups (p > 0.05). The reduction in direct bilirubin concentration in the serum was significantly different between groups at 72 hours and 96 hours (p > 0.001).
Conclusion
Purgative manna and phototherapy, can statistically significantly reduce total bilirubin concentration at 48 hours and 72 hours compared with phototherapy alone, and reduce the length of hospital stay for jaundiced neonates at 2 days compared with phototherapy treatment.
Introduction
Neonatal hyperbilirubinemia is a common problem observed in approximately 60% of term and 80% of preterm newborns [1–3] and may lead to kernicterus in severe cases [1,4]. The treatment is usually phototherapy or exchange transfusion [2]. In less severe cases (the vast majority), phototherapy is the most commonly used treatment method [2,5,6]. However in more severe cases, intensive phototherapy methods are used which may result in some adverse effects in neonates [7]. This would require monitoring of the neonates for therapeutic treatment response and adverse events [8,9].
Categorization of neonates hyperbilirubinemia into mild, moderate, and severe according to the bilirubin concentration would be useful for treatment selection [10,11]. The main mechanism of action of phototherapy is transformation of bilirubin to conjugated forms [12–14]. There are side effects of phototherapy treatment including retinal damage, diarrhea, and skin rashes in neonates [15,16]. In addition, the rate of nosocomial infections may be increased due to phototherapy [16,17]. The use of alternative therapeutic methods offered by traditional medicine such as herbal remedies may be beneficial in the recovery of infants from hyperbilirubinemia [18–22].
Bilineaster solution is an extract of purgative manna from the cotoneaster isocolor herb. Each mL of this herbal remedy contains 300 mg manitol. It is administered orally and absorbed minimally from alimentary tract leading to osmotic diarrhea aiding the excretion of different isomers of bilirubin. This diarrhea results in decreased serum levels of bilirubin; there were no serious adverse effects of Bilineaster [23]. In this study, the effect of Bilineaster drop and phototherapy was compared with phototherapy alone to determine whether phototherapy duration and the hospital stay could be reduced for in newborns with jaundice.
Materials and Methods
The study was approved by the Iranian Registry of Clinical Trials (IRCT2013110710933N2), on the 12th May 2014. This interventional study was performed as a randomized clinical trial. There were 150 consecutive term neonates (37 weeks to 40 weeks) that had developed jaundice (after 36 hours to 14 days of age), weighed 2,500 g to 4,000 g, and who were candidates for phototherapy, were enrolled in this trial. Patients who met the inclusion criteria were randomized using sequentially numbered, opaque sealed envelopes. In this system, the envelope containing the treatment allocation was opened by the clinician at the time of registration of the participant, (the clinician did not open the envelope before randomizing the participant) [24,25]. The exclusion criteria applied when there was a need to perform exchange transfusion or intensive phototherapy, or the neonates were; preterm, postdate, had congenital malformations or comorbidity (such as sepsis and infections), weighed < 2,500 g or > 4,000 g, developed jaundice after 2 weeks, had reduced neonatal reflexes, were ABO/Rh mismatch, had direct hyperbilirubinemia, or were fed with formula milk. In this study neonates who were born assisted via vacuum or forceps vaginal delivery were not excluded and the number of assisted births were comparable between groups. The neonates were randomly assigned to intervention or control group [26]. The control patients received only phototherapy (Philips Co., Tehran, Iran) and the intervention group underwent treatment with both phototherapy and Bilineaster drop (Sobhan Daru CO., Tehran, Iran) at a dose of 5 drops per kilogram of body weight, 3 times a day.
The bilirubin serum levels were measured at the time of admission as a baseline measurement, and every 24 hours across the groups using bilirubin-specific kits (Abnova CO.), and this data was compared across groups. The phototherapy was continued until the level of bilirubin in the serum was 10 mg/dL and if the neonate was generally healthy they were discharged from hospital. The length of hospital stay was determined and compared as a mean value between groups. The bilirubin molecule absorbs visible light (irradiance) ranging from 400 nm to 500 nm, with peaks around 460 nm [27,28]. Therefore, a phototherapy lamp with visible light (irradiance) ranging from 400 nm and 460 nm was used for all neonates across groups.
1. Ethical considerations
This study was approved be Hamadan University of Medical Sciences under the grant number of 16/35/9/3569 in January 2014. Written informed consent was given by all parents. The study was approved by the ethics committee and registration in Iranian Registry of Clinical Trials (IRCT2013110710933N2). All procedures involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments.
2. Statistical analysis
The Kolmogorov-Smirnov test was applied to determine the normal distribution of variables [27,29–32]. Data analysis was performed for 150 neonates including 75 patients in the control group and 75 newborns in the intervention group. Data analysis was performed by Statistical Package for the Social Sciences, version 20 software (IBM Corp., Armonk, NY, USA) [26,28,33–36]. Independent-Sample-T and repeated-measure ANOVA tests were used [37–41] and were considered statistically significant when p < 0.05.
Results
The control and intervention group were similar at baseline for all variables except birth weight and direct bilirubin concentration in the serum but these differences were not statistically significant (Table 1). As shown in Figure 1, > 90% of the patients in the intervention group, and < 80% in the control group were discharged within the first 3 days of admission. The mean length of time for hospital stay was 2.95 ± 1.01 days and 2.57 ± 0.68 days in the control and intervention groups respectively, but there was no statistically significant difference between groups (p = 0.06).
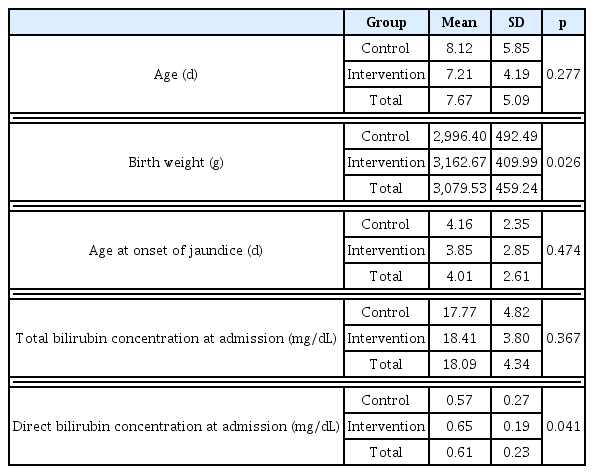
Baseline characteristics.
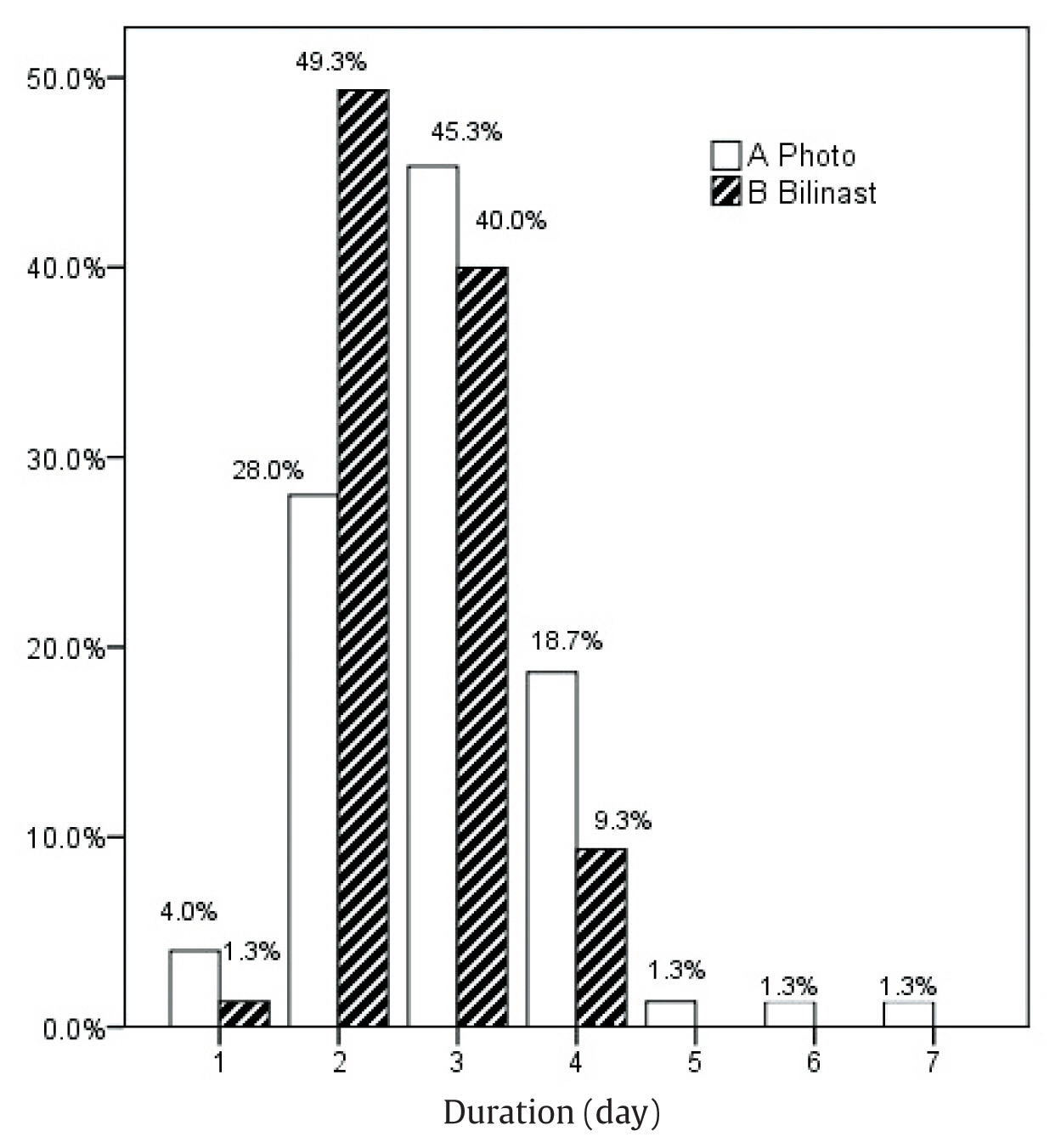
Hospital stay.
The serum concentration for total and direct bilirubin levels are shown as mean values in Figures 2 and 3, respectively. The reduced concentration of bilirubin in each group is shown in Table 2 as a mean value. The reduction in total bilirubin concentration from baseline was statistically significantly different across the groups at 48 hours (p < 0.001) and 72 hours (p < 0.001) but, not at 24 hours and 96 hours (Figure 2). The reduction in direct bilirubin concentration from baseline was statistically significantly different across the groups at 72 hours (p < 0.001) and 96 hours (p < 0.001) but, not at 24 hours and 48 hours (Figure 3).
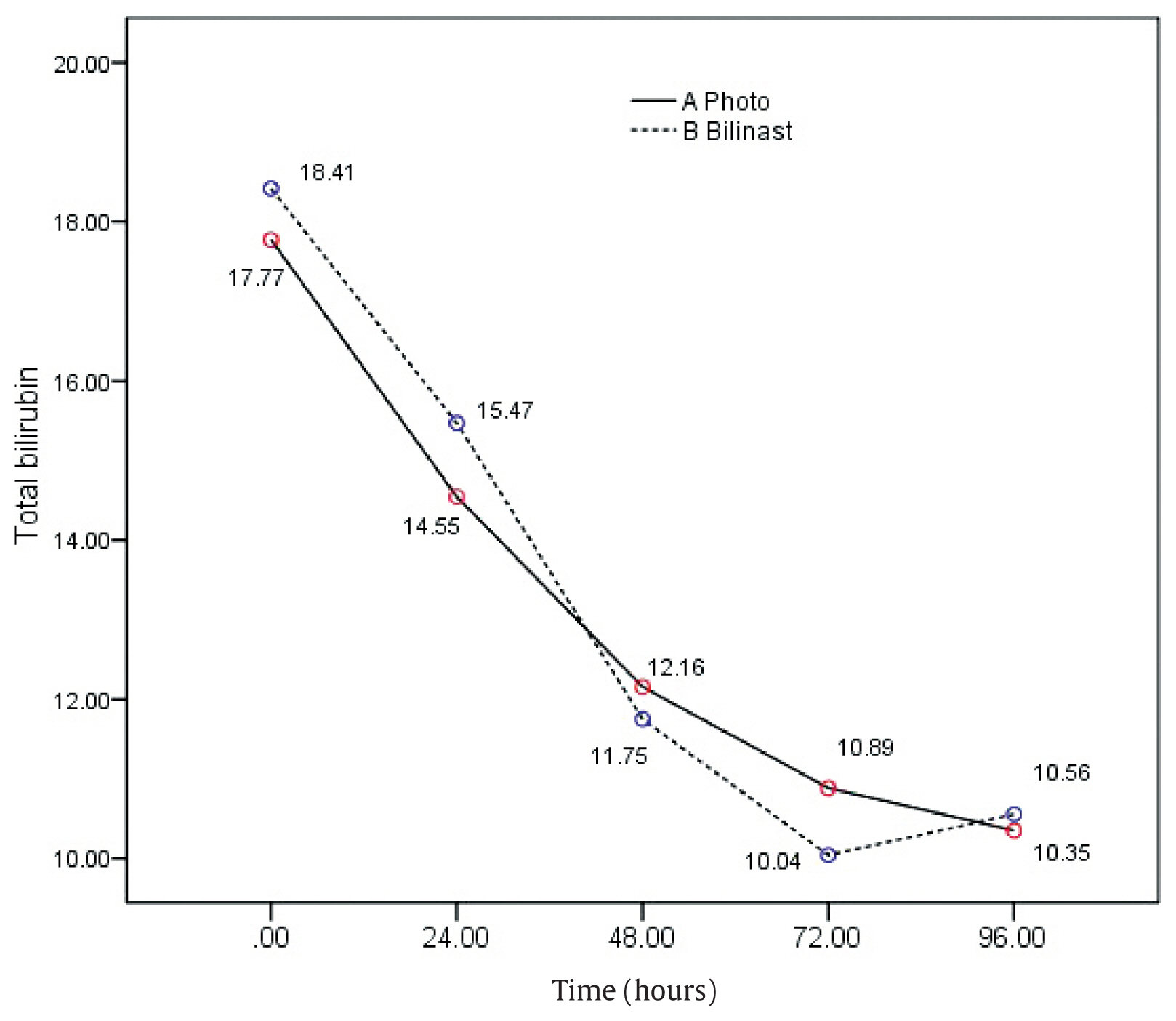
Total bilirubin concentration (mg/dL) expressed as a mean value, over time. The serum concentration of bilirubin expressed as a mean value for the groups was statistically significantly reduced at 72 hours in the Bilinaster and Phototherapy group compared with the Phototherapy treatment group p = 0.001.
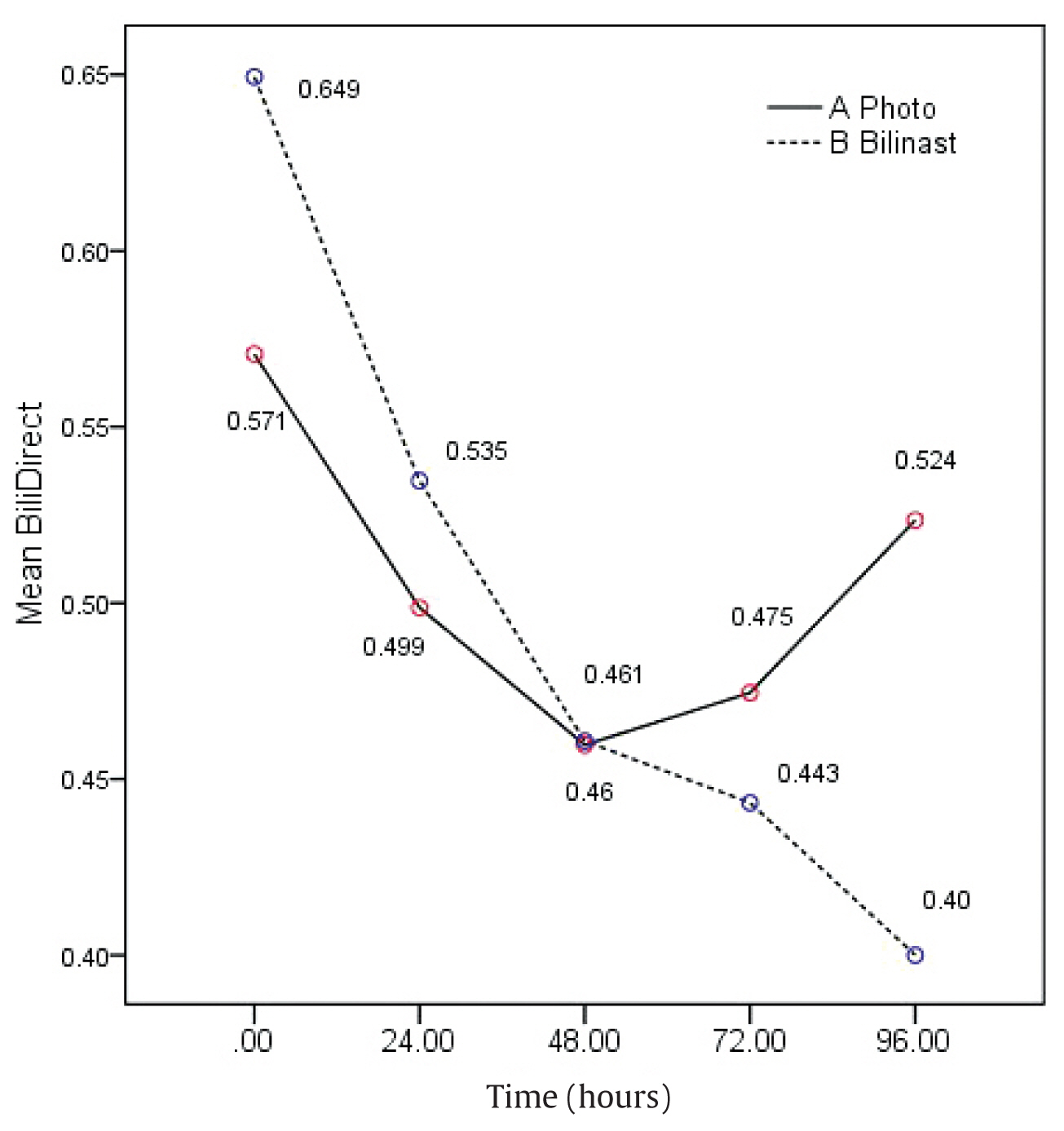
Direct bilirubin concentration (mg/dL) in the serum expressed as a mean value, over time.
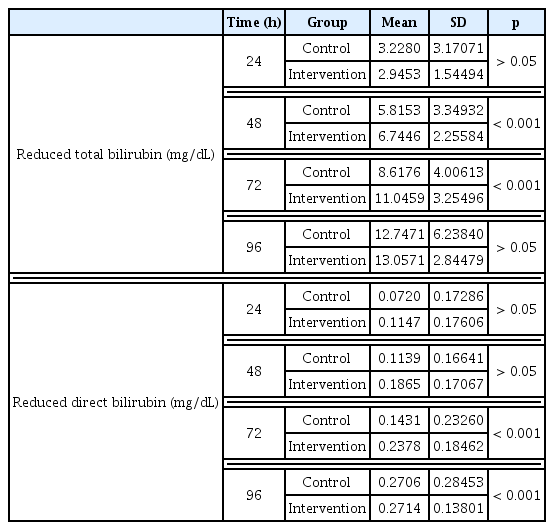
Reduction of bilirubin serum concentration following treatment.
The patients with higher baseline bilirubin concentrations had higher reduction rates due to treatment, and this was a statistically significant direct correlation (p < 0.001). However, age was not statistically significantly associated with reduced bilirubin concentration (p > 0.05), but birth weight in both groups was statistically significantly inversely correlated with reduced concentration of bilirubin (p = 0.001).
Discussion
Jaundice is a common clinical condition among newborns and it can be dangerous even among healthy term neonates. Phototherapy is the treatment of choice for jaundice and was given to both intervention and control groups in this study to determine the role of Bilineaster treatment as an intervention in the reduction of bilirubin concentration in the blood. The groups were of similar age and age of onset of jaundice. Only the birth weight was higher in the intervention group in comparison with the control group but this difference was not statistically significant (p = 0.026).
More than 90% of patients in intervention group and < 80% in control group were discharged during first 3 days of admission. However, the mean hospital stay was not statistically significantly different across the groups (p = 0.06). This lack of difference across the groups may be due to higher direct bilirubin serum concentration at baseline resulting from a higher birth weight in the intervention group. However, it should be mentioned that the baseline direct bilirubin concentration was statistically significantly higher in intervention group, p > 0.05 but the hospital stay was 0.4 days less than the control group. However, this the positive effect of Bilineaster was not statistically significant. In a similar study in Iran [11] where the intervention and control groups had the same baseline concentration of bilirubin, the hospital stay was statistically significantly less in the intervention group. In addition, there was a third group for comparison in that study; mothers that had consumed Bilineaster [11]. A statistically significant reduction in total bilirubin concentration was seen in all groups showing the effect of phototherapy. The decrease in bilirubin concentration in the phototherapy group at 24 hours was slightly greater in the control group compared with the intervention group, but this was not statistically significantly different. This could be due to a shorter half-life of Bilineaster or lack of initiation of effect. The other etiology is a higher initial direct bilirubin concentration in the intervention group. The reduction of bilirubin concentration in the serum at 48 hours and 72 hours revealed a positive additive effect of Bilineaster on bilirubin concentration. This may be due to binding of the resin in Bilineaster and inhibition of entrance to entrohepatic cycle. However, for a better understanding the mechanism of action of this substance, further studies with larger sample size and hematological studies are recommended. At 96 hours, the reduction in bilirubin concentration was greater in the intervention group compared with the control group but there was no statistically significant difference between groups. This could be due to the small sample size [24 patients (7 patients from the intervention group and 17 neonates in control group)] which may be too small to substantiate a statistically significant association. One study reported similar finding to this current study; a reduction of bilirubin concentration in the intervention group (Bilineaster and phototherapy) at 24 hours of treatment which was greater than the control group (phototherapy) [42]. However, in that study reduction of bilirubin concentration with Bilineaster treatment was not statistically significant different between groups. This difference in results between studies may be due to the assessment of therapeutic effect as described this current study rather than the prophylactic effect studied by Raeisi et al [42]. In addition, the dose of Bilineaster used was higher in this current study. So, the use of higher doses of Bilineaster for assessment of prophylactic effects is recommended. Rafieian-Kopaei et al assessed the effect of cotoneaster isocolor herb (an extract of which is purgative manna) among 100 newborns, and observed that the herbal remedy and phototherapy, was effective in the treatment of neonatal hyperbilirubinemia [43]; a finding similar to this current study. In addition, Ghotbi et al similarly reported that cotoneaster was effective in the treatment of neonatal hyperbilirubinemia resulting in a rapid decline in serum bilirubin concentration and cotoneaster treatment resulted in a reduced hospital stay duration [44].
Conclusion
In this study, treatment of jaundiced neonates with purgative manna (Bilineaster) resulted in a greater reduction of bilirubin concentration in the blood and had additive effects when combined with phototherapy treatment. Moreover, in the Bilineaster and phototherapy group the number of neonates leaving hospital at 2 days was higher than phototherapy treatment alone, although the mean length of stay was not significantly different between groups. Further studies with a larger sample size, mothers who receive Bilineaster, and assessment of prophylactic and therapeutic effects is required.
Acknowledgments
The authors are indebted to Dr. Fardmal for his assistance in statistical analysis, and Mrs. Fattahi for her practical help, and the Research Center of Hamadan University of Medical Sciences for their support.
Notes
Conflicts of Interest
The authors declared that they have no competing interests.