Risk Factors in Early Life for Preschool Children in Korea that are Associated with Being Overweight or Obese
Article information
Abstract
Objectives
The present study addressed the risk factors in early life for Korean preschool children that are associated with being overweight or obese.
Methods
A descriptive cross-sectional design was used to conduct this study, which included 507 mothers with preschool children aged 3–5 years, who attended daycare centers. Data were acquired via a self-administered questionnaire completed by the mothers. Of the 650 questionnaires that were distributed, 507 (78%) were completed and sent back. Multivariate logistic regression analyses were used to identify risk factors in early life, which may contribute to being overweight or obese in preschool children.
Results
Fifty-eight (11.4%) preschool children were overweight and 41 (8.1%) were obese. Multivariate logistic regression analysis with adjustment for covariates, revealed a significant association with the introduction of solid foods before 4 months of age [adjusted odds ratio (aOR) = 9.49, p = 0.029] and a nonresponsive feeding style (aOR = 2.80, p = 0.043) with being overweight or obese in preschool children.
Conclusion
The findings of this study highlighted the need for parenting education programs on feeding practices to increase their understanding of hunger and satiety cues in infants, and appropriate timing for the introduction of solid foods.
Introduction
Obesity is a major health concern for children because it significantly affects development [1]. In particular, an American study conducted in 2015–2016 including children aged 2–5 years, reported the incidence of obesity and severe obesity to be 26% [1]. According to the 2013–2014 Korea National Health and Nutrition Examination Survey, 14.9% Korean children aged 3–5 years were reported to be overweight or obese [2]. Obesity during early childhood is associated with a rapid increase in the number and size of fat cells [3]. Moreover, this increase in fat cells is difficult to control with exercise or diet modifications [4]. Therefore, younger children such as those at preschool, are at a higher risk of obesity than are children at any other developmental stage [5]. Furthermore, obesity during childhood is often associated with adult obesity [6]. Therefore, investigation into the risk factors related to obesity during early childhood, is crucial for any early intervention for the prevention of obesity during childhood and later life [7].
Monasta et al [8] categorized reasons for obesity in preschool children as a combination of factors influenced by children, and their parents, and their environment. It has been reported that gender, sedentary screen-based activity, physical activity, and sleep duration are contributing factors for children being overweight or obese [7,9]. Parental factors that influence childhood obesity include the mother’s age at childbirth, body mass index (BMI) of the parents, provision of sweet beverages to the children, provision of high-calorie snacks, and encouragement of excessive eating regardless of the child’s satiety cues [10,11]. Environmental factors that influence childhood obesity include the availability of a park or space close to home for outdoor play, a history of diabetes mellitus in the family, current maternal employment, the maternal marital status, the maternal educational level, the family’s current socioeconomic status, and the socioeconomic status of the family at the time of the child’s birth [12–14].
Prenatal stages, including pre-pregnancy, pregnancy, and infancy (< 12 months old), are considered critical periods for predicting childhood obesity [15]. A Korean study reported infantile risk factors including feeding on formula milk, rapid weight gain during the first 6 months, and maternal obesity, to be significantly associated with being obese in preschool children [16]. Young et al [17] proposed that becoming overweight in young children was influenced by maternal intake of high-fat food, and obesity during pregnancy. In addition, previous studies have shown that prenatal factors, including maternal obesity prior to pregnancy [18], high weight gain, and smoking during pregnancy [9,10], maternal depression during the prenatal stage [7], and pregnancy-associated diabetes [19], are positively associated with obesity in early childhood.
Furthermore, according to a contextual model for predicting childhood obesity [20], adiposity in children has been associated with characteristics such as gender, age, and eating habits as well as parenting factors such as formula and food supplementation types. Previous studies have also claimed a positive association of cesarean section births [10] and birth weight > 4,000 g [7,9] with early childhood obesity. Maternal parenting factors during infancy, such as introduction of solid foods < 4 months after birth [9], increase the likelihood of obesity in preschool children. However, exclusive breastfeeding and feeding according to the infants’ hunger cues and satiety are reportedly associated with a decreased risk for obesity among preschool children [21]. Therefore, identification of modifiable determinants of early-life risk factors has been proposed as an effective strategy for preventing childhood obesity [7].
Meanwhile, previous studies have reported that the risk factors contributing to childhood obesity or being overweight, differ depending on race and ethnicity [22,23]. In addition, early-life risk factors that contribute to obesity in childhood differ with cultural and social backgrounds, which has influenced the perception of early childhood obesity, and traditional or recommended lifestyle behaviors, associated with the development of early childhood obesity [23]. Korean infants have significant risk factors, including a social norm favoring excessive maternal weight during pregnancy, a lower prevalence of breastfeeding, and misperception of being overweight in childhood [16,24]. Traditionally, Korean people believe that the weight gained during pregnancy reflects mothers’ health and fetal growth status [24]. Therefore, there is a tendency to encourage excessive eating to gain weight during pregnancy despite overweight women not being acceptable in Korean society. The prevalence of exclusively breastfeeding at 5–6 months after childbirth was reported to be 14.9% in 2018. The objective of the 2020 Korean Health Plan is for 66.8% mothers to be exclusively breastfeeding at 6 months after childbirth [25]. The low rate of exclusive breastfeeding is probably attributed to early return to work after taking 12 weeks of maternity leave. In addition, workplaces often do not offer adequate support in the workplace for breastfeeding [26]. Similar to the Chinese, Koreans have a perception that “chubby” children are healthy and well developed [27]. Therefore, there may be a tendency to feed more food than necessary, even if the infant displays a feeling of satiety [27]. In this respect, the risk factors associated with early-life obesity in Korean children are likely to differ from similar factors in Western countries. However, many of the studies dealing with early-life risk factors for obesity in children have been conducted in Western countries [18,19,21,28]. Consequently, identification of early-life risk factors during the prenatal stage, and infancy, is crucial for developing tailored interventions to prevent obesity in Korean children, and controlling the covariates associated with the development of obesity in preschool children.
In the present study, based on models by Young et al [17] and Davison et al [20], early-life risk factors associated with obesity or being overweight in preschool children, were categorized as prenatal maternal factors, children’s factors during infancy, and maternal parenting factors for preschool children during infancy. To control for the various risk factors, covariates were categorized as children’s factors, parental factors, and environmental factors according to Monasta et al [8]. The focus was on identifying early-life risk factors during the prenatal stage, and infancy, that contribute to obesity in Korean preschool children, after controlling for covariates that enhance the risk of being overweight or obese in this population.
Materials and Methods
1. Study Design
This descriptive, cross-sectional study was based on a model that proposes prenatal factors linked with being overweight or obese in early childhood [17], as well as a contextual model that explains the connection between parenting factors, and children’s risk factors of becoming overweight or obese in childhood [20]. In the models by Young et al [17] and Davison et al [20], early-life risk factors associated with obesity and being overweight in preschool children were categorized as (1) prenatal maternal factors, (2) children’s factors during infancy, and (3) maternal parenting factors for preschool children during infancy (Figure 1).
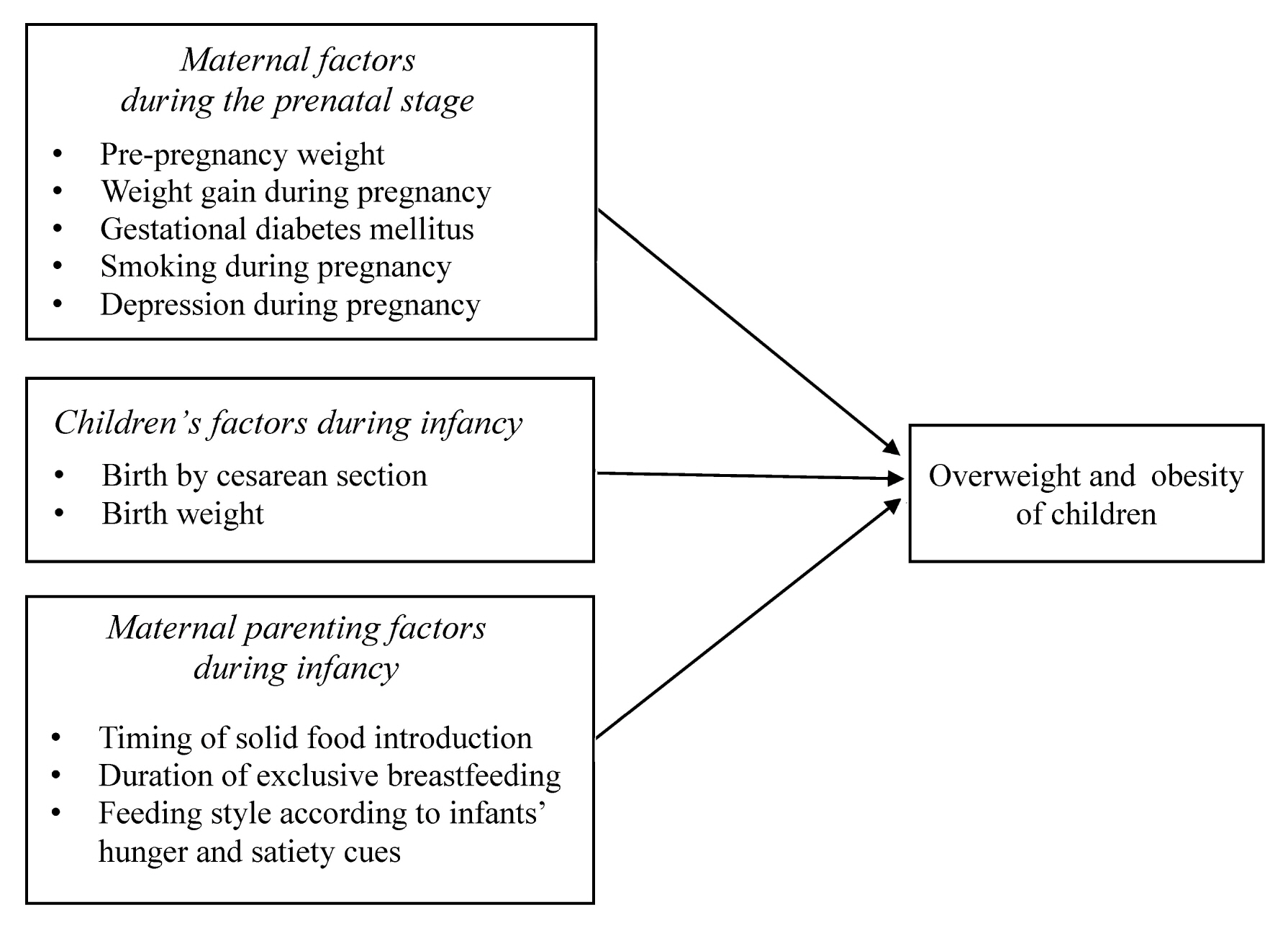
Hypothesized model.
2. Study participants
Obesity and being overweight can be evaluated in children from 3 years of age [29]. Thus, this study’s participants comprised of mothers with 3- to 5-year-old children who were attending day care centers located in Daejeon (a metropolis), and Jecheon city (a medium-sized city) in South Korea. For the selection of day care centers, a simple random sampling method was applied using random selection software (Excel Random Sample Software, 7.0). Mothers and children from each day care center were selected using the convenience sampling method, in accordance with the defined exclusion and inclusion criteria. Participants were included in this study according to the following criteria: (1) mothers and children (3–5 years) who gave their consent to participate, (2) children who were born following a gestation period of 37 weeks, (3) children who co-operated during the measurement of height and weight, and (4) mothers who could read, understand and provide answers in the questionnaire without seeking help. The exclusion criteria were as follows: (1) born prematurely or twins, (2) children born with health issues that affect weight gain (e.g., gastrointestinal disease, diabetes mellitus, kidney disease, cardiac disease, and hormonal disorders), and any genetic disorders, and (3) children who received medical, and nonmedical interventions for obesity.
A sample size of 408 mother-child pairs was determined in accordance with an odds ratio of 1.42 in a previous study [9], with an α of 0.05, and a power of 0.08 using the G*Power program version 3.1 [30]. A total of 507 mother (23–54 years)-child (266 girls and 241 boys, 3–5 years) pairs were included in the study.
3. Data collection
Data were collected between June and August 2017. Using a simple random sampling procedure using a random selection software (Excel Random Sample Software, 7.0), trained research assistants selected day care centers in Daejeon and Jecheon cities in South Korea that hosted more than 50 children. Of the 79 centers, 23 (29.1%) agreed to participate. Following this, the research assistants dispatched letters of recruitment to the mothers of the preschool children attending the selected day care centers. They then selected mothers who met the eligibility criteria (from mothers who responded to the recruitment letters). Teachers in each day care center distributed the self-administered questionnaires only to mothers who met the eligibility criteria. The questionnaires were completed by mothers at home and returned to their respective day care centers. The trained research assistants provided an explanation about answering the questionnaire via letters containing a contact phone number and email address 1 day before delivery of the questionnaire. If the mothers asked for additional information regarding the data collection process, including completion of the questionnaire, by phone or email, we provided information until mothers were satisfied. Of the 650 distributed questionnaires, 507 (78%) were returned with responses and were included in the statistical analysis. In addition, the research assistants explained and demonstrated the measurement process for height and weight to the preschool children, and received a verbal agreement from the children before measurements were taken. Furthermore, the research assistants explained that the preschool children who could not participate in the measurement process would be excluded from the study.
4. Ethical considerations
All research methods were approved by the institutional review board of the research institute at C National University, where the study was performed (2-1-46781-A-N-01-2017-HR-011). The study participants (mothers and preschool children) could refuse participation and leave at any stage. The mothers who participated provided written informed consent. Approximately 10 US dollars (10,000 won in Korea) were provided to the participating mothers.
5. Measurements
5.1. Outcome variables
5.1.1. Adiposity of children
Adiposity of the children was assessed using BMI. For BMI calculation, the weight of the children with their underwear was assessed to the nearest 0.1 kg using standard digital weighing scales (Tanita Um-075, Tanita Corp., Japan). Height was measured without shoes to the nearest 0.1 cm using a stadiometer. The trained research assistants measured the children’s weight and height twice and the mean values were then used to calculate BMI using the formula below.
The BMI value was transformed into a percentile and used to classify the children as obese (≥ 95th percentile), overweight (≥ 85th and < 95th percentile), normal weight (≥ 5th and < 85th percentile), or underweight (< 5th percentile) according to the Korean national growth chart for children and adolescents [31]. For logistic regression analysis, underweight and normal weight were categorized as non-overweight, while overweight and obese were categorized as obese.
5.2. Independent variables
Independent variables were measured with a self-administered questionnaire using the memory recall of mothers with preschool children. The long-term memory recall of mothers about their experiences at the time of pregnancy and childbirth, for example, gestational weight gain, smoking, health problems, birth weight, and birth by cesarean section, reportedly show good validity [32].
5.2.1. Maternal factors during the prenatal stage
5.2.1.1. Pre-pregnancy weight
For pre-pregnancy weight assessment, the BMI of the mothers was from self-reported heights and weights prior to pregnancy. The mothers were accordingly categorized as obese (≥ 25 kg/m2), overweight (≥ 23 kg/m2 and < 25 kg/m2), normal weight (≥ 18.5 kg/m2 and < 23 kg/m2), or underweight (< 18.5 kg/m2) according to recommendations of the Korean Society for the Study of Obesity [33].
5.2.1.2. Weight gain during pregnancy
A single question, “How much weight did you gain during pregnancy?” was used to assess the during-pregnancy weight gain. By adapting the criteria for weight-gain during pregnancy, in accordance with the weight status before pregnancy for Korean women, the suitable weight-gain range was considered as 16.7–24.7 kg for underweight, 11.5–21.5 kg for normal weight, 8–17.7 kg for overweight, and 7.5–21.9 kg for obese [34]. If the weight gain was below the recommended range, it was considered an inadequate amount of weight gain, and if it exceeded the recommended range, it was considered an excessive amount of weight gain.
5.2.1.3. Gestational diabetes mellitus
Gestational diabetes mellitus was assessed by a single question about a diagnosis of diabetes during pregnancy. Mothers responded with a “yes” or “no.”
5.2.1.4. Smoking during pregnancy
Smoking during pregnancy was assessed by a question about active (direct) smoking during pregnancy. Again, mothers responded with a “yes” or “no.”
5.2.1.5. Depression during pregnancy
Depression during pregnancy was assessed by asking the mothers if they were diagnosed or treated for depression by a certified psychiatrist during pregnancy. Mothers responded with a “yes” or “no.”
5.2.2. Children’s factors during infancy
5.2.2.1. Birth by cesarean section
Cesarean section birth was assessed by a question regarding the mode of delivery (natural or cesarean). Mothers responded with a “yes” or “no.”
5.2.2.2. Birth weight
The children’s birth weight was recorded via a question regarding this information and classified as < 2,500 g, ≥ 2,500 g < 4,000 g, and ≥ 4,000 g [29].
5.2.3. Maternal parenting factors during infancy
5.2.3.1. Timing of introduction of solid foods
The timing of solid food introduction was determined by a question asking the mothers about the age at which they introduced solid food to their infants. The timing of solid food introduction was classified as < 4 months, 4–6 months, 7–11 months, and ≥ 12 months after birth [10].
5.2.3.2. Duration of exclusive breastfeeding
The duration of exclusive breastfeeding was assessed by a question about the number of months for which the mothers breastfed their child without additional feeding with formula milk. The recorded duration of exclusive breastfeeding was classified as none, ≤ 3, 4–6, 7–11, and ≥ 12 months after birth [10].
5.2.3.3. Feeding style according to the infants’ hunger and satiety cues
The Infant Feeding Practices Questionnaire was utilized for evaluating the feeding style of mothers according to the hunger and satiety cues of their infants [35]. This questionnaire contained 2 questions, 1) “Did you feed the infant without a fixed feeding schedule i.e., when the infant gave a cue for hunger?” and 2) “Did you feed the infant according to a fixed feeding schedule regardless of the infant’s hunger and satiety cue?” Answers for each question were recorded as “never,” “almost never,” “occasionally,” “often,” and “always.” Mothers were considered to have a “responsive feeding” style if they answered “often” or “always” for the first question, and “never” or “almost never” for the second one. On the other hand, if the mothers answered “never” or “almost never” for the first question, and “often” or “always” for the second question, their feeding style was categorized as “non-responsive.” Mothers with other responses including “occasionally” were determined as a “mixed responsive” and “non-responsive” feeding style.
5.3. Covariates
Children’s gender was categorized as boys or girls. The sedentary screen-based activity was assessed with a single question about the average number of hours per day of screen-based activity (e.g., watching television and videos and using a smartphone and a computer) was permitted [36]. Responses were categorized as < 2, ≥ 2 < 4, ≥ 4 < 6, ≥ 6 < 8, and ≥ 8 hours per day [36]. Physical activity was assessed with a single question about the number of days where there were ≥ 60 minutes of vigorous physical activity performed during the week [7]. Responses were categorized as ≤ 3 and ≥ 4 days per week [7]. Sleep duration was assessed with a single question regarding the mean hours of sleep per day [7]. Responses were categorized as < 8, ≥ 8 < 10, and ≥ 10 hours per day [7].
Parental factors were evaluated using the mother’s age at childbirth (recorded by asking the age of the mother when she gave birth) ≤ 20, 21–25, 26–30, 31–35, or > 35 years. BMI of the parents was assessed from self-reported height and weight, and the parents were classified as obese (≥ 25 kg/m2), overweight (≥ 23 kg/m2 and < 25 kg/m2), normal weight (≥ 18.5 kg/m2 and < 23 kg/m2), or underweight (< 18.5 kg/m2) [33]. Finally, the weight status of the parents was classified as “not overweight” (normal or underweight) for both the parents, “not overweight” for 1 of the parents and “overweight/obese” for the other parent, and “overweight/obese” for both parents. The consumption of sweet beverages by the children was evaluated by a single question, “How many days per week, is your child permitted to drink a sweet beverage?” [37]. Responses were categorized as every day, 3–4 days per week, 1–2 days per week, and never [37]. The question for assessing the consumption of high-calorie snacks was, “Do you provide high-calorie snacks such as fried, or sugar-containing cookies, or bread between meals?” [37]. Responses were categorized as, often, occasionally, and almost never [37]. Parental feeding practices that encouraged more eating regardless of the children’s satiety cues were evaluated by the following question, “Do you encourage your children to eat even if they indicate satiety?” [37]. Responses were categorized as often, occasionally, and almost never [37].
Environmental factors were outdoor play which was assessed by a question about the presence of a park or space near the residence and answers were recorded as yes or no. With regard to a family history of diabetes mellitus, the participants were questioned about the occurrence of maternal or paternal diabetes in the family and the answer was “yes” or “no.” The maternal employment status was assessed and classified as no paid work (housewife), part-time job, and a full-time job. The marital status was classified as married, divorced, or other. The educational level of mother was classified as below high school level, high school level, and above high school level (including 2 years of college, university, and graduate school). The present socioeconomic status of the family and the socioeconomic status at the time of the child’s birth, were categorized as low, middle, and high.
6. Statistical analysis
Data were analyzed using SPSS (version 24.0 for Windows, IBM Corp., Armonk, NY, USA). Descriptive analysis was performed to present the characteristics of maternal factors during the prenatal stage, children’s factors during infancy, and maternal parenting factors during infancy. Using multivariate analysis, significant risk factors for early-life obesity in preschool children were identified.
In the first step, a simple logistic regression analysis was performed to identify each set of factors associated with obesity in preschool children. In the second step, significant factors (p < 0.25) associated with obesity in preschool children in univariate analysis were entered into a model for the multivariate logistic regression analysis [38]. Since a statistical significance level (p) of < 0.05 may have missed significant factors, Bursac et al [38] proposed a significance level of < 0.25 from univariate analysis. Multicollinearity was examined using variance inflation factors.
Results
1. Adiposity of preschool children
More than half [392 (77.3%) of 507] the preschool children had a normal weight. Fifty-eight (11.4%) preschool children were overweight, and 41 (8.1%) were obese. Sixteen preschool children (3.2%) were underweight.
2. Characteristics of maternal factors during the prenatal stage, children’s factors during infancy, maternal parenting factors during infancy, and covariates
With respect to maternal factors during the prenatal stage, more than half (65.3%) the mothers had a normal weight before pregnancy. The proportion of mothers who were overweight or obese before pregnancy was 21.3%, and mothers with gestational diabetes mellitus accounted for 8.5%. The proportion of mothers who smoked during pregnancy was 11.2%. Most mothers (98%) did not experience depression during pregnancy. With respect to children’s factors during infancy, 41.4% of children were born via cesarean section. The birth weight of most children (89%) was ≥ 2,500 g and < 4,000 g. With respect to maternal parenting factors during infancy, the majority of the mothers introduced solid foods (40.6%) between 4 and 6 months after birth. More than 69% of mothers (69.4%) did not practice exclusive breastfeeding at all. There were 25.8% of mothers who practiced exclusive breastfeeding up to 12 months after the birth of their child. Approximately a quarter of the mothers (28.6%) practiced a responsive feeding style (Table 1).

Characteristics of early-life risk factors associated with being overweight or obese in preschool children (N = 507).
The covariate analysis for children’s factors showed that 36.7% of the preschool children were exposed to sedentary screen-based activities for ≥ 2 < 4 hours per day, and 66.7% of the children slept for more than 10 hours per day. Covariate analysis of parental factors showed that 37.2% of the mothers “occasionally” encouraged their child to eat more, 26.4% “often” encouraged their child to eat more (10.8%) regardless of their child’s expression of satiety. For environmental factors, most preschool children (93.1%) had a park or space near their home to play outside, and 48.9% of the children had a family history of diabetes mellitus (Table 1).
3. Risk factors in early life associated with being overweight or obese as a preschool child
Univariate logistic regression analyses for maternal factors during the prenatal stage that statistically significantly (p < 0.25) influenced preschool children becoming overweight or obese, were insufficient weight gain during pregnancy [odds ratio (OR) = 0.52, p = 0.007], and gestational diabetes mellitus (OR = 1.91, p = 0.068). Among children’s factors during infancy that statistically significantly influenced preschool children becoming overweight or obese, were birth by cesarean section (OR = 1.36, p = 0.174), and a birth weight of ≥ 2,500 g < 4,000 g (OR = 2.48, p = 0.142). Among maternal parenting factors during infancy that statistically significantly (p < 0.25) influenced preschool children becoming overweight or obese, were the introduction of solid foods < 4 months after birth (OR = 5.73, p = 0.024), and a non-responsive feeding style (OR = 1.68, p = 0.085; Table 2).
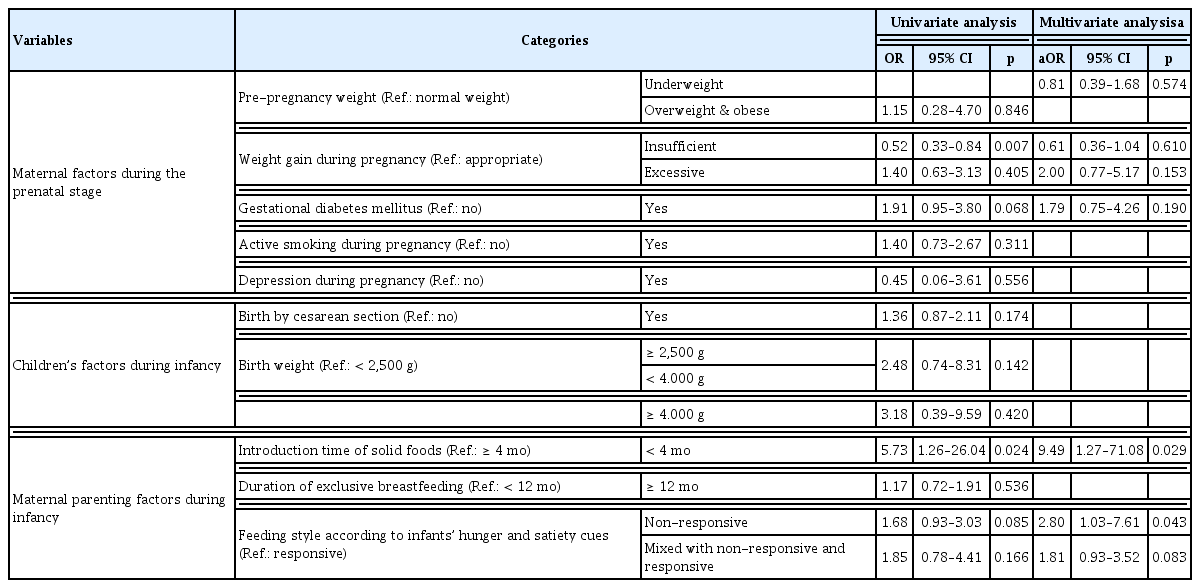
Early-life risk factors associated with preschool children being overweight and obese (N = 507).
Multivariate logistic regression analysis after controlling for covariates, showed that the introduction of solid foods < 4 months after birth [adjusted OR (aOR) = 9.49, p = 0.029)], and a non-responsive feeding style (aOR = 2.80, p = 0.043) were associated with preschool children becoming overweight or obese (Table 2).
Discussion
This study identified the risk factors associated with early-life obesity or being overweight in Korean preschool children. According to this study, the introduction of solid foods < 4 months after birth, and a nonresponsive feeding style (wherein parents fed their children regularly without paying heed to their hunger and satiety cues), were significantly associated with preschool children becoming overweight or obese. This trend was not observed for maternal factors during the prenatal stage and children’s factors during infancy.
It has been reported that maternal feeding of an infant that is characterized by a lack of response to the infants’ hunger and satiety cues, results in the child becoming overweight in early childhood [39]. In the same context, mothers with children at high risk for obesity demonstrated more restrictive feeding styles, with the assumption that mothers can recognize their infant’s hunger and satiety cues [40]. Worobey et al [41] reported that a lack of maternal sensitivity toward the satiety cues of infants led to overfeeding due to the increased frequency or amount of feeding, and this was associated with early childhood obesity. Meanwhile, maternal feeding practices in line with the infants’ hunger and satiety cues supported self-regulatory eating among infants [42]. This energy intake during a responsive type of feeding, may provide the necessary conditions required to facilitate the development of regulatory capacity and autonomy throughout infancy and into childhood [43]. In previous studies, a decreased risk for children becoming overweight was reported in breastfed infants, relative to the risk in formula-fed infants, and was associated with the ability to self-regulate energy intake, which was acquired during breastfeeding. This may encourage maternal responsiveness toward the infants’ hunger and satiety cues [44,45]. According to the Bright Future parent handout by the American Academy of Pediatrics [46], it is recommended that from the 4th month onwards, parents should avoid feeding their infants too much, and the parent should follow the signs of fullness indicated by the infant which may include leaning back, and turning away. In addition, interventions focusing on early feeding practices, including responsive feeding during infancy, were effective for the prevention of early childhood obesity [47,48]. Thus, responsive feeding is considered an important prevention strategy for obesity during infancy [47].
In Korea, similar to China [27], overweight children in early childhood and infancy are considered to have superior growth, as a result of successful maternal parenting. In addition, the amount of feeding may reflect the health status, and potential growth in young children. Thus, Korean mothers may excessively feed their children by ignoring their infants’ satiety cues, or regularly feed their infant despite the lack of hunger cues. These factors may lead to obesity in preschool children. Therefore, interventions promoting responsive feeding among Korean mothers may highlight the role of this type of feeding in self-regulatory eating behavior in infants. In order to improve Korean parents’ social awareness of early childhood obesity, a community program should promote the importance of choosing the appropriate type of maternal feeding, and early-life risk factors associated with obesity in Korean preschool children.
In addition, the introduction of solid foods < 4 months after birth increased the likelihood of becoming overweight at 3–5 years of age [49]. Grummer-Strawn et al [50] proposed that the early introduction of solid food may result in increased consumption of foods containing high levels of fat and sugar during infancy. Furthermore, consumption of high-calorie solid foods during infancy has been linked to the consumption of high-calorie foods in older children [51]. Thus, the early introduction of solid foods containing sugar and fat, may contribute to the development of eating patterns that may result in children becoming overweight [52]. The American Academy of Pediatrics advises parents to introduce solid foods at approximately 6 months [53]. Parents should be educated about the appropriate time for the introduction of solid foods to help prevent obesity in preschool children.
Infancy is an important period in the development of eating habits [54]. In addition, infants depend on a primary caregiver, mostly their mothers, to provide healthy foods and the appropriate amount of energy to be healthy [40]. Therefore, parenting behaviors, especially feeding during infancy, have been considered to be a significant component for intervention in the prevention of early childhood obesity [42]. Pediatric nurses play an important role in the evaluation of children’s development and health status, in addition to providing counseling and guidance for health promotion, and normal development in clinics and communities. The United States Institute of Medicine introduced an early-childhood obesity prevention guidance program, suggesting that healthcare professionals should undertake regular growth monitoring, and consider the risk factors for obesity during infancy [55]. Similarly, pediatric nurses should identify the early risk factors associated with childhood obesity, and develop, and provide interventions for the modification of parenting styles, such as feeding behaviors.
The current study has some limitations. Firstly, data from mothers was obtained by employing a self-administered questionnaire, and this may not be entirely reliable and objective. Therefore, the recorded results could have been compromised because of social pressure biases (such as questions on height, weight, breastfeeding, and smoking), and the data obtained may have skewed the results and may have presented a false negative missing a real relationship between parameters. Secondly, a cross-sectional survey design was employed in this study, which limits the inferences of causality between the dependent and independent variables. Therefore, it is necessary to conduct a well-organized prospective cohort study in the future to establish the causality of the relationship between risk factors in early life, and obesity in preschool children. Thirdly, the 2007 version of the Korean national growth chart for children and adolescents was used in this study therefore, there is a possibility of misclassification errors by not using the current version of growth charts. Further research using the latest version should be conducted in order to increase the accuracy of the study.
Despite these limitations, this is the first study of early-life risk factors during the prenatal stage and infancy, for obesity in Korean preschool children, after controlling for children’s factors, parental factors, and the environmental factors as the covariates.
Conclusion
The introduction of solid foods < 4 months after birth, and a non-responsive feeding style by parents during infancy, were significant early risk factors for Korean preschool children becoming overweight or obese. However, maternal factors during the prenatal stage, and children’s factors during infancy, were not associated with preschool children becoming overweight or obese. These results suggest the need for parenting education programs to support parental understanding of an infant’s hunger and satiety cues, the appropriate age for introducing solid foods, and the appropriate foods to give to children in the prevention of obesity in preschool children. Thus, as primary health providers, pediatric nurses should develop, and provide intervention programs focusing on early feeding management for the prevention of early childhood obesity.
Acknowledgments
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government, Ministry of Science, ICT and Future Planning (2017R1C1B1003762).
Notes
Conflicts of Interest
The authors have no conflicts of interest to declare.