
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 4(2); 2013 > Article
-
Original Article
Peer-to-Peer JXTA Architecture for Continuing Mobile Medical Education Incorporated in Rural Public Health Centers - Rajkumar Rajasekaran, Nallani Chackravatula Sriman Narayana Iyengar
-
Osong Public Health and Research Perspectives 2013;4(2):99-106.
DOI: https://doi.org/10.1016/j.phrp.2013.03.004
Published online: April 30, 2013
Vellore Institute of Technology, School of Computing Science and Engineering, Vellore, India.
- *Corresponding author. E-mail: vitrajkumar@gmail.com
Copyright ©2013, Korea Centers for Disease Control and Prevention
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives:
- Mobile technology helps to improve continuing medical education; this includes all aspects of public health care as well as keeping one’s knowledge up-to-date. The program of continuing medical and health education is intertwined with mobile health technology, which forms an imperative component of national strategies in health. Continuing mobile medical education (CMME) programs are designed to ensure that all medical and health-care professionals stay up-to-date with the knowledge required through mobile JXTA to appraise modernized strategies so as to achieve national goals of health-care information distribution.
-
Methods:
- In this study, a 20-item questionnaire was distributed to 280 health professionals practicing traditional training learning methodologies (180 nurses, 60 doctors, and 40 health inspectors) in 25 rural hospitals. Among the 83% respondents, 56% are eager to take new learning methodologies as part of their evaluation, which is considered for promotion to higher grades, increments, or as part of their work-related activities.
-
Results:
- The proposed model was executed in five public health centers in which nurses and health inspectors registered in the JXTA network were referred to the record peer group by administrators. A mobile training program on immunization was conducted through the ADVT, with the lectures delivered on their mobiles. Credits are given after taking the course and completing an evaluation test. The system is faster compared with traditional learning.
-
Conclusion:
- Medical knowledge management and mobile-streaming application support the CMME system through JXTA. The mobile system includes online lectures and practice quizzes, as well as assignments and interactions with health professionals. Evaluation and assessments are done online and credits certificates are provided based on the score the student obtains. The acceptance of mobile JXTA peer-to-peer learning has created a drastic change in learning methods among rural health professionals. The professionals undergo training and should pass an exam in order to obtain the credits. The system is controlled and monitored by the administrator peer group, which makes it more flexible and structured. Compared with traditional learning system, enhanced study improves cloud-based mobile medical education technology.
- The continuing mobile medical education (CMME) model is mostly used by the professionals in pharmaceutical industries, as the resources are increasingly shared in the industry. A lot of manual training programs and personnel involvement were required to keep one’s knowledge and technical skills up-to-date. Because of the rapid advancement in technology such as availability of fast internet access and massive storage capacity, computer-based learning models can be used as an alternative method to overcome these problems. This can be achieved by creating a system that can facilitate automatic CMME.
- Advancements in mobile technology and the use of the internet have attracted many to design various mobile-based applications that allow one to browse the web (mobile browsers), send/receive e-mails, as well as form discussion groups and share resources. The mobile learning system can be pictured as a model in which individuals receive continuing education in an online environment, typically using the JXTA network in their mobile devices. Because the existing paper-based models may not be the best to try out these applications efficiently, there is a need for alternative model to handle such applications. One such kind is the peer-to-peer (P2P) JXTA technology that enables individuals to try these applications without any intervention or collation.
- P2P works in an environment in which computers or mobile hosts communicate with each other in a distributed fashion without using a centralized control point to route or connect data traffic. In practice, P2P technologies deployed today adopt a network-based computing style that neither excludes nor inherently depends on centralized control points. To have an interoperable and secure communication among different peers, an open-source Java framework (JXTA) can be used. JXTA for the mobile environment is known as JXTA Micro Edition (JXME) and allows different mobile devices to participate in the JXTA network. We maintained a 5-year cycle, in which doctors, nurses, health inspectors, and fellows of public health centers require 400 credits, with a minimum of 25 credits obtained in each year of the cycle. Depending of the type of learning activity undertaken, one or two credits are earned per hour. The Ministry of Health (MOH) requires 250 credit hours over a 5-year cycle. A total of 50 credits must be obtained for each year of the cycle. In the same way, each state requires a complete documentation of on-going CMME for licensure. The scenario that motivates this paper is a common problem faced by mobile users, that is, interoperability and security in P2P M-learning applications. While exchanging data among peers in a closed group, the main things to be considered are security, authentication, and updating knowledge. Even for P2P continuing mobile medical learning system, these things should be considered. We are hoping that these issues could be solved through the JXTA/JXME framework architecture proposed in this paper. This provides an attractive generic infrastructure to define and implement custom P2P services rapidly.
Introduction
- Continuing mobile medical learning is knowledge in hand. The system can deliver a complete set of course or parts of it. We define mobile medical learning as all “mobile knowledge.” It includes the use of JXTA in mobile/handheld devices to perform or deliver education/learning (administration), provide faster communications/collaboration (for end users), conduct assessments/evaluations (review), and finally performance support/knowledge (assessment).
- With the present growth in mobile technology, a number of portable devices can be made use of to quickly and easily deliver a public health update. Cell phones (smartphones), multigame devices, personal media players, personal digital assistants (PDAs), or wireless single-purpose devices can help deliver coaching and mentoring as well as conduct assessments and evaluations (e.g., quizzes, tests, surveys/polls, and certifications), deliver podcasts, update alerts, forms, and checklists. Mobile devices with JXTA embark as powerful data-collection tools and facilitate the capture of user-created content.
- The central administrator (CA) will control the data exchange through an interstate-level administrator (SA) who reports to the MOH. The roles and responsibilities of a CA include maintaining records to track activities performed by the SAs and checking the authentication of data forwarded by SAs that will authorize user access (as and when the request for accession is received). The CA is also in-charge of sending periodic reports to the MOH for license renewal and cancellation (according to the credit system). The SA is responsible for maintenance of data in all the districts of the state. There is one SA for each state and each SA will be appointed by the CA (Figure 1).
- Roles and responsibilities of the SA are maintaining records and tracking activities performed by district administrators (DAs), appointing DAs, checking the data/information forwarded for further authentication by CA. The SAs are eligible for defining and following a protocol for data exchange between DAs of the state as well as between the DAs and the CA. The DAs are the smallest but the most important part of the hierarchy as they have direct access to the database containing the details of all the registered users (doctors, health professionals, etc.) in the district. The users should approach them for registration. They lay down the format for information intake and act as a bridge between the SAs and the users of the district. They will ensure the enforcement of protocols in hospitals and will forward license renewal/cancellation reports (according to the credit system; “n” credits in “x” years) to the respective SAs. They maintain a system for storing user’s personal information such as their ID, password, personal identification number, name, age, gender, qualification, experience. CMME users are mostly doctors, hospital staff, nurses, health inspectors from pharmacies, research laboratories, pathology laboratories, etc. These registered users will be allowed access to the JXTA network containing existing data as well as to a cloud network containing latest updates. They will have a username and a password that would authenticate their access to the system through the authorization check center (ACC).
- The ACC that stores confidential user information in a secure manner is handled through the JXTA network. The center will check for authentication of users when they try to access the data in the network during which their username and password are verified by the CA. The registered users are granted access to the next level (database administrator). An administrator links the resources to the system. Any request that is processed and sent from the ACC with a positive review is immediately processed by the administrator. An administrator can be an authorised group that has complete control over the information resources. Analysis and research has been performed to facilitate the user, in a way to avoid surfing the internet for different data; this system has a provision of linking up with existing data on the JXTA network. New technology and research performed are updated according to the data storage area through a different and very simple method. This information along with a set of protocols can be directly submitted in the system. Information can be updated by anyone who has access to the system, and in addition, the update policy is compulsory for the hospital authorities. For example, a chief medical officer updates newly registered cases in their respective hospitals, which can be referred to by other doctors in the JXTA network. While adding new updates, there is a mandatory protocol to complete paper submission, in which the author frames a set of minimum n multiple choice queries based on his/her article (paper). This query has a role in the credit system for authorized health workers such as doctors, nurses.
- 2.1. Credit system
- The main aim of this paper is implementing continuing medical education (CME) into technology. Therefore, it is necessary for the authorized health workers to achieve a target of x credits in n periods. For example, currently a doctor has to attend 30 hours of lectures over a period of 5 years, at a minimum level. Violation of this may lead to cancelation of the practice license, which is renewed postreview after a length of time n. The authorized medical worker will have to open up recourse information request and should answer the questionnaire that will be visible along with the information. Upon completion of the questionnaire, the authorized account will be given credits. The same paper cannot be answered again, although the medical workers can access the data anytime and anywhere. A review committee handles new updates that are sent to them for validation from different locations. Each state has its own review committee. The minimum requirement of a rural public health center is to have two medical officers, nine nurses with three for hospitals and six as village health nurses, and five health inspectors (Table 1).
- These data will be sent to the review committee. After validating the data provided and checking whether the submission is done without violation of any of the protocols, the data are forwarded to administrators or else it is rejected. The new data set is stored in a database, which is the space taken up on the internet in a definite amount and all the information is stored in it. Mobile JXTA is implemented here for its durability and fast-access capabilities. The main functions are to maintain the new data resource, i.e., any new data from two different review committees are not the same or the fresh update is not present as such in the existing data. In other words, it checks that the data are not repeated in the database. It also manages the access given to any of the users to the information present in the JXTA network as well as acting as a link between the MOH and the data information. It is a legalized procedure through which the government is given access to the information.
Materials and Methods
- This includes tasks and knowledge gained by the health inspectors and medical officers. They will be actively taking part in arranging and organizing all training programs through mobile JXTA for the trainees. The role of health inspectors in primary health center (PHC) is to conduct trainings up to the subcentral level and carry out instructions issued from time to time. The health inspector also has to educate and inform communities about the various medical services available in PHC, maintain online reports for all programs, responsible for arranging health-related camps around the area, and undergoes online training through the mobile JXTA network to stay up-to-date.
- The role of a medical officer in PHC is to develop staff capabilities through training, improve clinical knowledge of the staff and provide online training to other PHC doctors. A medical officer undergoes online training with new updates on complicated surgery procedures through the registered mobile JXTA network. The role of a nurse in a PHC is to conduct staff meeting and discuss ways to improve service through training. A nurse also arranges for clinical experience of the nursing students, conducts examination for the students, and practices continuing learning through mobile JXTA P2P.
Outdoor Tasks Supporting Module
- A variety of protocols, architectures, and implementations can analyze the results of existing P2P solutions. Technologists often use diverse methodologies that are all asynchronous based on the query–response model. Using these protocols, peers can discover each other or find network resources. Peers are not required to implement all the protocols; instead, they can just implement what they need. JXTA protocols have been used as a foundation for building CMME applications. The identification of various protocols that could be used in the JXTA framework with various functionalities is analyzed. We considered a peer membership protocol (PMP) using the JXTA framework.
- 4.1. P2P secure communication
- Security is one of the major factors considered in any network environment, and P2P networks are no exceptions from these security issues. Security attacks in P2P systems can be classified into two broad categories, namely, active and passive network attack [1]. JXTA has many built-in security features that can enhance applications built over it. Some of the security features provided by JXTA are as follows:
- For the proposed architecture, personal security environment would be the best choice because it provides peer ID and a password for every individual participating in the knowledge update process. This personal security environment helps in defending the local attackers or loss of mobile phones.
- 4.2. Proxyless and proxied peers
- Mobile devices (peers) that do not rely or depend on any super peer to communicate with other peers are called proxyless peers. Mobile devices (peers) with limited resources and less capability are connected to a special peer called relay peer or rendezvous peer in order to communicate with other peer groups in the JXTA/JXME network. A relay peer is capable of handling 150 peers and is helpful in effective communication among different peers.
- 4.3. Hungry individual peers
- Hungry individuals are always looking to undergo training programs. They will be allowed to join admin peer to discover new learning courses. They will publish responses from (PPG1 and PPG2) individuals and will typically select training programs depending on the number of criteria (credits, course duration, and evaluation CMME) as well as look for the best offer and best program to update their knowledge (Figure 2).
- Peer group id. In the proposed system we make groupid ( ) through the mkgrp community.
- JXTA > MKPgrp PPG1 (Public Health Center 1) JXTA > MKPgrp PPG2 (Public Health Center 2) JXTA > Groups
- MOBILEARN net. The peer group defines the scope of interaction and discovery between all peer entities involved in the CMME learning. It involves all peers who participate in learning either as a learner or as a trainee.
- Admin peers. The admin provides any update and displays advertisement (ADVT), e-Learning continuing medical education readiness index (eCMERI) to the hungry peers. They discover and join MOBILEARN net peer group based on their training topics and receive response for their requests.
-
Peer group advertisement. An advertisement is sent to proxy peer groups PPG1 and PPG2, which describes specific resources such as name, group ID, description, specification, and service parameters.
<xs: element name=“PPG1” type=“jxta: PPG1”/>
<xs: element name=“GID” type=“JXTAID”/>
<xs: element name=“MSID” type=“JXTAID”/>
<xs: element name=“Name” type=“xs: string” minoccurs=“1”/>
<xs: element name=“Desc” type=“xs: any type” minoccurs=“1”/>
<xs:elementname=“Svc” type=“jxta:serviceParam”minoccurs=“0” maxoccurs=“unbounded”/>
</xs: complex type>
- GID refers to the peergroupID that uniquely identifies a peer group (PPG1, PPG2). MSID lists the specification ID describing the training programs in the peer group. Name is uniquely given to the public health centers (PPG1 and PPG2). DESC gives the descriptive information used to index and search for a peer group. SVC describes the association between the group services.
- 4.4. PMP
- A peer includes a PMP for joining and leaving peer group1 (PHC1) and peer group2 (PHC2). PMP identifies the following methods accessed by peers and JXTA messages for CMME:
- Request: Membership requests are sent to the authenticator if the mobile peer is interested in undergoing a training program after entering the group. The response message or an acknowledgement is sent back by the authenticator to the peer.
- Add: After applying, the peer is added to the peer group, allowing him/her to select the required course.
- Modify and update: A renewal message is used for updating the membership information if it needs to change.
- Performance and evaluation: To be eligible for certification, the mobile peers are assessed on their knowledge gained from the course.
- Reject: Peers can also reject their peer membership group from taking the training.
- Functionality: It creates groups and publishes the advertisement. The architecture advertisement ADVT protocol also provides code for the membership policies. Thus, authentication and authorization can be achieved using this implementation. Using this protocol any peer (user) can automatically change the group ID by leaving the present group and joining in another new group. Here, any peer in proxy group can leave that group using the “finish” command and can join in another group as proxy group two.
P2P JXTA Protocols
- The CME modules received modest use over 1 year by patrons outside of the test-bed network, while no usage of the CME modules was recorded by patrons of the test-bed network. Barriers to success were clearly identified [2]. A previous study reported on online CME courses through the enhancement of the Sharable Content Object Reference Model (SCORM) and the use of metadata, using a SCORM-compliant open-source learning management system platform, namely, modular object-oriented dynamic learning environment, also called moodle, assumes the definition of learning objects and learning outcomes for a specific target audience of the course design of an instructional module that incorporates several types of learning material in a medical practice in Greece [3]. A number of technologies have been adopted in medical education, for example, virtual practice or virtual patients, learning using online guides, web-based instruction, and distance learning method. Several recommendations for incorporating or adopting technology in medical education are also determined [4]. The aim of the paper is to present the results of the European Union Erasmus project called GEROM, which among others resulted in the online gerontological interdisciplinary-focused master curriculum. It is flexible, innovative, diverse, contemporary, and information and communications technology based (in both content and implementation). The project focused on meeting the needs of older people and their careers, with the aim of promoting the health and well being of elderly [5]. Factors to be considered before incorporating PDAs to medical education have been identified. What is yet to be determined is the strategy for incorporating these devices into the problem-based learning context, the kind of information necessary for students to be carried on their PDAs, the information that would be suitable for students in evidence-based medicine, as well as the ways to ensure that incorporation of PDAs provides students and medical faculties effective learning, given the cost and resource implications involved [6]. The importance of CME and eLearning eCMERI is expected to provide not only a relevant research insight into the field, but also to help CME managers implement eCME programs more effectively and efficiently [7]. A comprehensive review of the use of M-learning includes reviewing the definition, benefit, and the current technology. Compared with traditional learning environments, mobile technologies have opened the doors for providing medical learning experiences outside of the classroom [8]. All these modes have their own advantages and disadvantages [9]. In this context, online P2P mobile JXTA continuing education service would be more flexible and secure. There are a number of companies that allow online P2P systems in their workplace, and it can be explained that peers in different peer groups can communicate with each other through a relay peer [10]. A social network can be viewed as two distinctive and interacting networks. The first one is a network of persons, including authors, potential authors, and final users of learning objects (students, or teachers or others, e.g., educational managers).
- The second is a network of published learning objects [11]. However, technical challenges of mobile health-cloud controller exist. A survey was conducted to identify key technologies, partition off-loading, and context-based services [12]. Some studies in the literature aimed at overcoming the problems of P2P applications using JXTA in both desktop and mobile environments. For example, Tahsin et al [10] established a network connection and created a P2P message-passing application, while Leong et al [13] proposed a mobile service-oriented architecture based on mobile agents, in which agents are in-built programs that are capable of reacting to active changes in their environment [14]. In the collaborative ubiquitous learning environment, people can easily create materials and post it to the server, which could be synchronous and asynchronous. To make the M-learning model interactive, artificial intelligence in mobile learning is carried out [15], and this includes a teaching-support system and a decision-support system. Considering all these approaches of P2P in m-commerce, we have proposed the architecture of an m-commerce application, i.e., a mobile auction based on JXTA/JXME network, which provides interoperability and security among different peers.
Discussion
- Standards for delivering the mobile JXTA were established in our proposed design, which includes technology, security, and privacy. The objective of keeping knowledge up-to-date includes proving access and usage effectiveness of learning delivered through P2P mobile JXTA toward the CMME.
- 6.1. Training program on immunization
- The objectives of this program are as follows:
Deliver continuous training with no degradation to learning effectiveness.
Achieve 50% of eligible participation.
Achieve a comparable average score to the peer groups.
Obtain a 20% higher completion rate in a lesser time.
CMME training on the following through JXTA to the mobile device:
How to obtain latest policy and universal coverage with respect to PHC.
Procedure to get adequate supply of vaccines from time to time.
Procedure for proper storage of vaccines.
How to investigate and report all complications.
How to ensure regular surveillance of all vaccine-preventable diseases.
How to carry out surveys and arrange to refer cases.
- Users underwent training and took online exams; they obtained high scores half of the time. Users who completed the training did so in 54 minutes or less and tested higher on the final assessment tests than the others of the firm. Of the 250 eligible employees, 6% launched the content at least once and 56 people completed the courses (Table 2). Overall, the mobile learners obtained a 56% higher knowledge gain completion rate in 30% less time than the control group. A total of 70 employees responded to a survey indicating more than 75% praised the benefits of convenience, time management, and training through mobile JXTA. Additional results will be forthcoming, but these initial results are very encouraging. Each state has many pharmacists, research labs, doctors, nurses, health inspectors, and medical staff. CMME is a legalized forum which is implemented for all medical workers to update their knowledge according to the development of technology. Figures 3 and 4 show the M-learning on a tablet and mobile phone.
Submitting an Event “CMME schedule”
- In order to prove the credentials of the web-based services, a social networking page is launched (http://localhost:80/cmme.php/immunisation.htm), where users register for knowledge update management. The implementation of the suggested CME linkage with the technology can be given an aid by the fastest growing site www.facebook.com. A page has already been created on the social networking site and is named as CMME UPDATES. The function of this page is to keep the authorized medical staff up-to-date with different new additions of information into the database. Moreover, any new user entry can be intimated here, so users can be familiar to one another. Social networking sites make communication among people in same fields easier. For example, when a new paper has been uploaded by a user through the review committee, an update is made on the page about this new entry into the database. The users who have consent with this particular research opens and views it through their logins in the system created. As a result, all health professionals keep their knowledge up-to-date using the database very easily and effectively.
CMME Schedule on a Social Networking Page
- 1. Brookshire D, Govoni D, Krishnan N, et al. JXTA—JAVA P2P Programming. Sams Publishing; 2002.
- 2. Mei PY, Jun ZX, Li L. Learning can happen anytime and anywhere: the application of M-learning in medical education. In: 2nd International Workshop on Education Technology and Computer Science (ETCS); 2010. p. 508−11.
- 3. Bachmann L, Cantoni L, Coyne J, et al. Are we ready for a CME eLearning Readiness Index (eCMERI)? A map and a literature review. In: 3rd International Conference on Human System Interactions (HSI); 2010. p. 513−9.Article
- 4. Bamidis P, Nikolaidou M, Konstantinidis S, et al. A proposed framework for accreditation of online continuing medical education. In: 20th IEEE International Symposium on Computer-Based Medical Systems (CBMS’07); 2007. p. 693−700.Article
- 5. Blazun H, Kokol P. In: 23rd IEEE International Symposium on Computer-Based Medical Systems (CBMS); 2010. p. 445−9.
- 6. D’Alessandro M, Galvin J, Choi J, et al. Continuing medical education to the point of care using a digital library and intimate computers In: Proceedings of the IEEE International Forum on Research and Technology Advances in Digital Libraries; 1997; (ADL ’97). 1997. p. 95−101.
- 7. Luanrattana R. Considerable factors of incorporating PDAs to medical education. In: International Conference on Information Technology Based Higher Education and Training (ITHET); 2011. p. 1−8.Article
- 8. Luanrattana R. A review of information technology use in medical education: an overview. In: 7th International Conference on Advanced Information Management and Service (ICIPM); Seogwipo, South Korea. 2011. p. 121−4.
- 9. Mäkeläinen SI. From B2C to C2C e-commerce. Course Essay: Department of Computer Science, University of Helsinki; 2006.
- 10. Tahsin T, Choudhury LF, Rahman L. Peer-to-peer mobile applications using JXTA/JXME. In: Proceedings of the 11th International Conference on Computer and Information Technology (ICCIT 2008); 2008 Dec 25–27; Khulna, Bangladesh.Article
- 11. Kaldoudi E, Dovrolis N, Konstantinidis S, et al. Social networking for learning object repurposing in medical education. J Inform Technol Healthcare 2009;7(4). 233−43.
- 12. Nkosi M, Mekuria F. Cloud computing for enhanced mobile health applications. In: IEEE 2nd International Conference on Cloud Computing Technology and Science (CloudCom); 2010. p. 629−33.Article
- 13. Leong IP, Miao C, Lim BK, et al. Agent mediated peer-to-peer mobile service-oriented architecture. In: Inaugural IEEE International Conference on Digital Ecosystems and Technologies (IEEE DEST 2007); 2007.Article
- 14. Shih Y. Language in action: applying mobile classroom in foreign language learning In: 5th IEEE International Conference on Advanced Learning Technologies (ICALT 2005); 2005. p. 548−9.
- 15. Yang Q. Research of e-learning resource management and distribution system using JXTA P2P network. In: International Conference on Internet Technology and Applications; 20–22 Aug. 2010; Network Center, China Univ. of Geosci., Wuhan, China. 2010. p. 1−3.Article
References
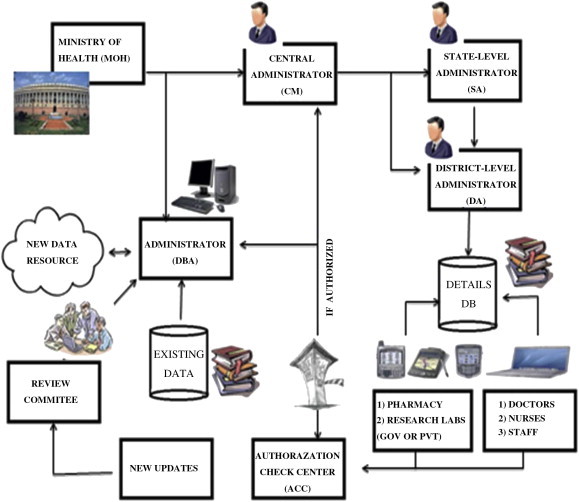
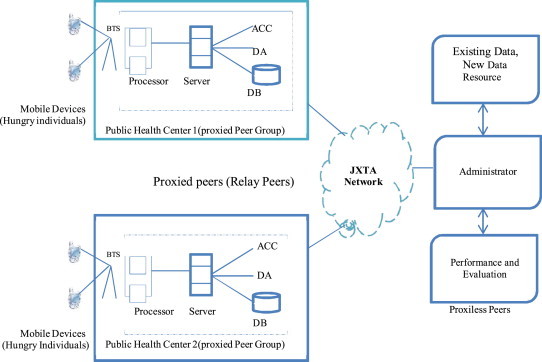

Figure & Data
References
Citations
- The effects of mobile applications in cardiopulmonary assessment education
In-Young Yoo, Young-Mi Lee
Nurse Education Today.2015; 35(2): e19. CrossRef
 PubReader
PubReader Cite
Cite



